
Abstract
Background: Post-traumatic stress disorder (PTSD) has been shown to be associated with migraine and drug abuse.
Methods: This was an analysis of data from the National Comorbidity Survey Replication (NCS-R) to evaluate the association of PTSD in those with episodic migraine (EM) and chronic daily headache (CDH).
Results: Our sample consisted of 5,692 participants. Lifetime and 12-month prevalence rates of PTSD were increased in those with EM and CDH. After adjustments, the lifetime odds ratio (OR) of PTSD was greater in those with EM (OR 3.07 confidence interval [CI]: 2.12, 4.46) compared to those without headache; was greater in men than women with EM (men: OR 6.86; CI: 3.11, 15.11; women: OR 2.77; CI: 1.83, 4.21); and was comparable or greater than the association between migraine with depression or anxiety. The lifetime OR of PTSD was also increased in CDH sufferers. The OR of illicit drug abuse was not increased in those with EM or CDH unless co-occurring with PTSD or depression.
Conclusion: The lifetime and 12-month OR of PTSD is increased in those with migraine or CDH, and is greater in men than women with migraine. The lifetime and 12-month OR of illicit drug abuse is not increased in those with migraine or CDH unless co-occurring with PTSD or depression.
Keywords
Introduction
Although there is substantial research documenting an association between the Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV mood and anxiety subtypes (including generalized anxiety disorder [GAD], obsessive compulsive disorder, panic disorder, and social phobia), an association between post-traumatic stress disorder (PTSD) and migraine has only recently been identified (1,2). In a general population sample of over 5,500 adults, the 12-month period prevalence of PTSD was 14.1% in episodic migraineurs, as compared to 2.6% of those without any headache disorder (1). This finding was supported by a large, multicenter, clinic-based, population study in which 22.4% of those with episodic migraine (EM) and 30.3% of those with chronic daily headache (CDH) fulfilled PTSD criteria (2). However, the effect of gender and illicit drug and alcohol abuse on this relationship was not explored in either study.
Both migraine and PTSD are more common in women than men (3–5). Additionally, drug and alcohol abuse have been shown to be increased in those with PTSD, with three major community studies reporting that women with PTSD are 3.1–4.5 times more like likely to abuse drugs and 1.4–3.1 times more likely to abuse alcohol than women without PTSD (5–8).
Thus, our current study was designed to evaluate the association between PTSD with EM and CDH as compared to those without headache and to examine the potential role of gender, mood disorders and drug and alcohol abuse in this association.
Methods
Sample
The National Comorbidity Survey Replication (NCS-R) is a cross-sectional, general population survey of mental disorders in the United States (US) conducted between February 2001 and April 2003. The NCS-R uses a structured research diagnostic interview to assess the prevalence and correlates of DSM-IV disorders. In brief, a total of 10,000 participants were selected from a multistage area probability sample of noninstitutionalized, civilian population in the United States. A letter was sent to targeted households describing the purpose and investigators of the study. This was followed by in-person contact with an interviewer who enumerated the household and selected a random household member to participate in the study. Recruitment and consent procedures were approved by the human subjects committees of Harvard Medical School and the University of Michigan. All participants were administered a core diagnostic interview, of which Part I included mood disorders and drug and alcohol abuse. All participants who screened positive for any disorder in Part I, plus approximately a one-in-three probability subsample of other Part I participants, received a Part II interview, which included questions about correlates and additional disorders, including migraine. The response rate for the data collection was 70.9% (N = 7,693) among those receiving the primary interview and 80.4% (N = 1,589) among secondary predesignated respondents.
The sample was weighted to adjust for differential probability of selection, differential sampling into Part II and residual discrepancies between sample and census population socio-demographic and geographic distributions. A more detailed discussion of NCS-R sampling and weighting has been previously described (9,10). All analyses herein use these weights.
Measures
Demographics
Sociodemographic characteristics were evaluated, including age, gender, race, marital status, education and smoking, as previously described (9).
Mental disorders
DSM-IV disorders were assessed with the World Health Organization’s Composite International Diagnostic Interview (CIDI), version 3.0, a fully structured, lay-administered, diagnostic interview. A previous clinical reappraisal study using the DSM-IV Axis I Disorders, Research Version, Non-patient Edition of the Structured Clinical Interview for DSM-IV (SCID) found generally good concordance with CIDI diagnoses (11). Major depressive disorder (MDD), GAD, PTSD and drug and alcohol abuse were assessed. Organic exclusions were applied. Additionally, DSM-IV diagnostic hierarchy rules were applied in making diagnoses where available, (ie. GAD, MDD and alcohol abuse). A diagnostic hierarchy rule is a criterion in the DSM-IV that states if a patient fulfills two disorders of which one is the better explanation than the other, then the primary disorder or best-fitting diagnosis is given diagnostic hierarchy over the other. In the NCS-R database, if a participant fulfilled criteria for a disorder that was best attributable to another disorder, only the primary disorder was coded. For example, if a participant fulfilled criteria for GAD but also fulfilled criteria for PTSD, the primary disorder was coded as PTSD. Similarly, if a participant had MDD from a chronic medical illness this would not be included as primary MDD. This hierarchy was applied for MDD, GAD and alcohol abuse and dependence (those psychiatric disorders for which a primary designation is available,) and for which existed no other explanation for these disorders. Finally, a “lifetime” designation is used for those who met criteria at any point in their life, while a “12-month” designation is used for those who met criteria within the past year.
Post-traumatic stress disorder
As part of the PTSD protocol, participants were asked about lifetime exposure to 27 specific traumas. Participants were also given the opportunity to report other nonlisted traumas. Individual trauma items were summed for a total number of lifetime traumas experienced. PTSD was then assessed for those endorsing at least one traumatic event. Participants who endorsed more than one were assessed for their worst event and a randomly selected event. Participants who met diagnostic criteria for either their worst/only event or random event were diagnosed with PTSD, and asked their age at onset and the age of the most recent event evoking PTSD symptoms.
Headache diagnoses
Participants were asked whether they ever experienced “frequent or severe headaches”. Those who answered affirmatively were asked if such headaches occurred in the prior 12 months. Participants reporting frequent or severe headaches in the past but not within the prior 12 months were classified as having “nonactive headache” and excluded.
Participants responding affirmatively to having frequent or severe headaches in the prior 12 months were asked more detailed questions. Specifically, headache duration, location, severity, quality, frequency, presence of nausea, photophobia or phonophobia were evaluated (Appendix 1). Additionally, the number of days of headache per year and the age of first onset of frequent or severe headaches were evaluated. Aggravation of pain by activity was not assessed. Headache diagnoses were then classified according to the International Classification of Headache Disorders, second edition (ICHD-II), with one modification: those who fulfilled ICHD-II criteria for migraine based on an affirmative response to the presence of “photophobia or phonophobia” were designated as “modified” definitive migraine (12). Finally, those participants fulfilling migraine criteria who reported headaches on fewer than 15 days of the month were classified as episodic migraineurs, while those reporting headaches on 15 or more days of the month were defined as CDH sufferers. Thus, the following four groups were included: (i) those with no headache, (ii) those with episodic nonmigraine headache, (iii) those with EM and (iv) those with CDH.
Analysis
Statistical analyses were performed using PASW version 17. Differences in continuous variables were tested using analysis of variation (ANOVA) or t-tests. Fisher’s exact or Chi-square approximation tests were used for categorical variable comparisons where appropriate. Associations between headache and mood disorders or drug and alcohol abuse were assessed using logistic regression models. Variables were included as possible confounders if p < .1 in univariate analyses. Backward elimination was used in logistic regression analyses for inclusion of variables; variables were included in the model if p < .05 or removal changed the magnitude of the primary association by more than 15%. Interactions between headache type and all demographic characteristics were assessed and considered statistically significant if p < .05; of these, only gender was significant, and is included here.
Results
Participants
A total of 5,692 participants had complete information in regard to both headache and PTSD, of which 595 participants who did not have headache in prior 12 months but who reported a previous history of frequent or severe headaches at some point in their life, and 34 participants who only fulfilled probable migraine criteria were eliminated from further analysis. Thus, 5,064 participants were included.
Demographics
Demographic characteristics of NCS-R respondents by headache subtype

NCS-R = National Comorbidity Survey Replication. SD = standard deviation. USD = US dollars.
aComparison to no-headache group. bComparison to nonmigraine episodic headache group. cComparison to episodic migraine group.
Headache
Of included participants, 86.7% (4393/5064) had no headache history in the prior 12 months or their lifetime; 13.3% (671/5064) had frequent or severe headaches in the prior 12 months; 5.0% (251/5064) fulfilled ICHD-II criteria for EM, (74.9% definitive migraine, 25.1% modified-definitive migraine,) and 3.0% (151/5064) fulfilled CDH criteria. A total of 34 participants who only fulfilled criteria for probable migraine were eliminated from further analysis.
Depression and anxiety
Prevalence rates and adjusted ORs of PTSD, mood disorders and drug and alcohol abuse by headache subtype
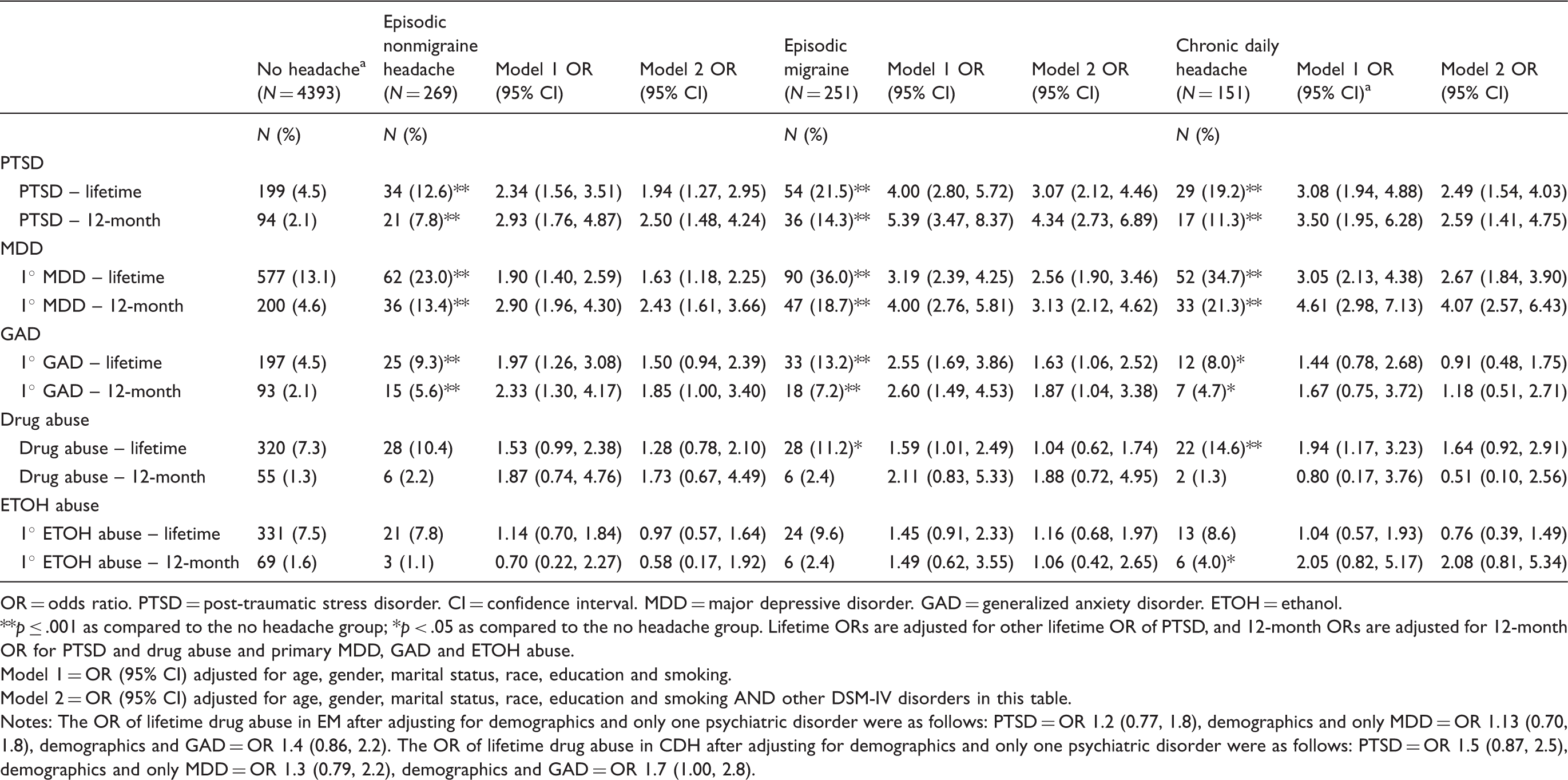
OR = odds ratio. PTSD = post-traumatic stress disorder. CI = confidence interval. MDD = major depressive disorder. GAD = generalized anxiety disorder. ETOH = ethanol.
**p ≤ .001 as compared to the no headache group; *p < .05 as compared to the no headache group. Lifetime ORs are adjusted for other lifetime OR of PTSD, and 12-month ORs are adjusted for 12-month OR for PTSD and drug abuse and primary MDD, GAD and ETOH abuse.
Model 1 = OR (95% CI) adjusted for age, gender, marital status, race, education and smoking.
Model 2 = OR (95% CI) adjusted for age, gender, marital status, race, education and smoking AND other DSM-IV disorders in this table.
Notes: The OR of lifetime drug abuse in EM after adjusting for demographics and only one psychiatric disorder were as follows: PTSD = OR 1.2 (0.77, 1.8), demographics and only MDD = OR 1.13 (0.70, 1.8), demographics and GAD = OR 1.4 (0.86, 2.2). The OR of lifetime drug abuse in CDH after adjusting for demographics and only one psychiatric disorder were as follows: PTSD = OR 1.5 (0.87, 2.5), demographics and only MDD = OR 1.3 (0.79, 2.2), demographics and GAD = OR 1.7 (1.00, 2.8).
The crude prevalence of GAD was greater in those with EM and CDH compared to those without headache (Table 2). However, after adjustments, the lifetime and 12-month odds ratio (OR) of GAD were significantly increased only in those with EM (Table 2).
Traumatic life events
Of all participants, irrespective of PTSD status, the mean number of traumatic life events (TLEs) was greater in those with EM or CDH compared to those with no headache. EM participants reported a mean of 4.6 ± 3.6 TLEs and CDH sufferers 4.2 ± 3.3, compared to 2.6 ± 2.5 by those without headache, p < .001 for both. Among those without PTSD, EM and CDH participants reported more TLEs (EM 4.2 ± 3.4 TLE; CDH sufferers 3.7 ± 3.0 TLEs,) compared to those without headache (2.5 ± 2.4 TLEs), p < .001 for both. Among those with PTSD, although those with CDH reported a greater number of TLEs (6.5 ± 3.6) as compared to those with no headache (5.3 ± 3.4), p = .05, there was no significant difference in the mean number of TLEs reported by EM participants (6.0 ± 4.1) compared to those without headache, p = .5.
Post-traumatic stress disorder
Prevalence and odds ratio in EM and CDH
Of all participants, 7.7% (389/5064) fulfilled PTSD criteria. Of those with a lifetime history of PTSD, 52.2% also fulfilled PTSD criteria in the prior 12 months. The crude lifetime prevalence of PTSD was greater in those with EM (21.5%) and CDH (19.2%) compared to those without headache, (4.5%; p < .001; Table 2). Similarly, the 12-month prevalence of PTSD was greater in those with EM and CDH as compared to those with out headache (Table 2). After adjusting for demographics, the lifetime and 12-month odds ratio of PTSD were four- to fivefold greater in those with EM (life: OR 4.00; CI: 2.80, 5.72; 12-month OR 5.39; CI: 3.47, 8.37) and over threefold greater in those with CDH (life: OR 3.08; CI: 1.94, 4.88; 12-month: OR 3.50; CI: 1.95, 6.28) compared to those without headache; and remained significant after adjusting for drug abuse, MDD, GAD and alcohol abuse (Table 2).
Gender differences
Gender-specific prevalences, ORs and 95% CIs for the association between migraine, CDH and PTSD

OR = odds ratio. CI = confidence interval. CDH = chronic daily headache. PTSD = post-traumatic stress disorder. MDD = major depressive disorder. GAD = generalized anxiety disorder. ETOH = ethanol.
**p < .001 as compared to those with no headache. *p = .006 as compared to those with no headache.
Model 1 = OR (95% CI) adjusted for age, marital status, race, education and smoking.
Model 2 = OR (95% CI) adjusted for age, marital status, race, education and smoking AND other DSM-IV primary diagnosis, lifetime.
Note: In addition to demographics, model 2 lifetime ORs are adjusted for other lifetime ORs of primary MDD, GAD, ETOH abuse and lifetime OR of any drug abuse, while 12-month ORs are adjusted for 12-month ORs of primary MDD, GAD, ETOH abuse and 12-month OR of any drug abuse.
Sensitivity and specificity of a DSM-IV diagnosis of MDD and GAD to predict PTSD
The sensitivity and specificity of a DSM-IV MDD diagnosis identifying DSM-IV PTSD in EM and CDH participants was poor, suggesting that identification of depression in migraineurs is not sufficient to capture those with PTSD. The overall sensitivity of a DSM-IV MDD diagnosis being associated with a DSM-IV PTSD diagnosis was 42% in EM participants and 50% in CDH participants, while the specificity was 65% in EM participants and 69% in CDH participants. The positive predictive value (PPV) of a DSM-IV MDD diagnosis to capture PTSD was 24.4% for EM participants and 26.9% for CDH participants.
Although the specificity of any DSM-IV diagnosis of GAD being able to identify DSM-IV criteria PTSD was good (80.7% EM; 89.3% CDH), the sensitivity was fair to poor (64.8% EM; 34.5% CDH); and the PPV of a DSM-IV GAD diagnosis to capture PTSD was poor (33% for EM; 43.5% for CDH participants).
Temporal relationship between PTSD and headache
Of those with EM and PTSD, 69.2% (36/52) reported PTSD before the onset of severe or frequent headache. Similarly, of those with CDH and PTSD, 71.4% (20/28) reported PTSD prior to developing severe or frequent headaches.
There were no significant differences in (i) the mean age at onset of PTSD, (ii) the mean years since the onset of PTSD, or (iii) the mean age of the most recent event evoking PTSD symptoms in those with no headache compared to those with EM or CDH. However, the mean number of years since the last episode evoking PTSD was greater in those with no headaches (9.6 years ± 12.5) compared to EM participants (4 years ± 8.4, p < .001) and CDH participants (5.6 years ± 8.8, p = .04).
Drug and alcohol abuse
The crude lifetime prevalence of drug abuse was greater in EM participants (11.2%) compared to those without headache (7.3%, p = .02) as well as in CDH participants (14.6%) compared to those without headache (7.3%, p < .001). Additionally, the crude 12-month prevalence of alcohol abuse was increased in those with CDH (4%) as compared to those without headache (1.6%, p = .04).
The ORs of alcohol abuse (either over a lifetime or 12-month period), were not different in EM or CDH participants compared to those without headache, after adjusting for demographics only (Table 2). In contrast, after adjusting for demographics only the ORs of a lifetime history of drug abuse were increased in EM (OR 1.59; CI: 1.01, 2.49) and CDH (OR 1.94; CI: 1.17, 3.23) participants; however, after adjusting for demographics and psychiatric disorders, all significance was lost. Additionally, we evaluated the ORs of drug abuse in EM and CDH participants after adjusting for demographics and each mood disorder individually. Specifically, in those with EM, the lifetime OR for drug abuse was no longer significant after adjusting for demographics and either PTSD alone (OR 1.24; CI: 0.77, 1.98) or MDD alone (OR 1.34; CI: 0.85, 2.12), but remained significant after adjusting for demographics and only GAD (OR 1.68; CI: 1.08, 2.62). Similarly, the lifetime OR for drug abuse in CDH patients was no longer significant after adjusting for demographics and PTSD alone (OR 1.59; CI: 0.94, 2.69) or MDD alone (OR 1.66; CI: 0.99, 2.77), but remained significant when demographics and GAD alone were adjusted for (OR 2.19; CI: 1.33, 3.61)
Discussion
Several mood disorders have been shown to be associated with migraine (13,14). More recently, an association between PTSD and migraine has been increasingly recognized (1,2,15). In this study we found a one-year-period prevalence rate of PTSD of 14.3% in participants with EM compared to 2.1% in those with no headache, and a lifetime prevalence rate of 21.5% in participants with EM compared to 4.5% in those with no headache (2). We also found increased prevalence rates of PTSD in those with CDH (1 year: 11.3%; lifetime: 19.2%).
We also report three other important new findings. First, our results suggest that the association between PTSD and migraine is comparable if not stronger than the association between migraine and either primary MDD or GAD; furthermore, identification of depression and/or anxiety is not sufficient to identify those with PTSD. Second, our current study is the first to evaluate the gender-specific OR of PTSD in migraineurs. Although increased in both genders, we found a stronger association for PTSD in men than in women with EM, with more than a sixfold increase in OR of PTSD in men with migraine as compared to an approximately threefold increase in women with migraine. To our knowledge, this is the first mental disorder to be reported as having greater prevalence in male than in female migraineurs. Thus our data suggest that migraineurs, and in particular male migraineurs, should be screened for PTSD. And in those migraineurs who do have PTSD, treatment of the PTSD should be strongly considered, as treatment of PTSD alone has been shown to positively influence both pain and disability in chronic pain patients (2).
The third important finding from our study pertains to the association between alcohol and drug abuse and migraine. Similar to previous studies, no association between migraine and alcohol abuse was found (16). Further, in our current study we found that any association between drug abuse and migraine could be attributable to either PTSD or depression but not GAD.
How PTSD is related to migraine pathophysiology is not known. It has been well described that migraineurs manifest an increased sensitivity to internal biological stressors (ie. stress, sleep changes,) as well as to external environmental stressors (ie. dietary triggers). PTSD could reflect this increased reactivity of migraineurs to extreme stressors.
Additionally, biologically, low levels of serotonin and dysfunction of the autonomic system have been linked to both PTSD and migraine (17–19). Furthermore, several studies have suggested a dysfunction in the hypothalamic-pituitary-adrenal (HPA) axis for both disorders, with the majority of studies suggesting that elevated levels of cortisol are present in those with recent traumatic exposure and who are at greatest risk of developing PTSD, while low levels are present in those who have already developed PTSD (20–23). Studies have also suggested that migraineurs may have baseline elevated cortisol levels (24,25); and others have shown an abnormal HPA response to activation (26,27). Taken together, these data suggest that migraineurs could have a greater biological risk for developing PTSD as well as an abnormal HPA response when activated. Further evaluation of this hypothesis is warranted.
It is unclear why the association with migraine and PTSD is stronger in men than women in our current study. However, several sex-related differences of the HPA axis may play a role. First, a general trend suggests a greater acute HPA response in adult men, with a greater corticotropin-releasing hormone (CRH)-stimulated adrenocorticotropic hormone (ACTH) and exercise-stimulated cortisol response in men compared to women (27,28). Second, a functional MRI (fMRI) study demonstrated gender differences in cerebral blood flow (CBF) in response to psychological stress in regions of the brain that also modulate pain (28). Others have suggested that the greater HPA axis activation in men may leave them more vulnerable to some stressors, whereas the female stress response may be more “buffered” due to a greater production of estrogen and oxytocin, which may counter the effect of cortisol (28–30). These data, together with our current findings, suggest that further research with attention to the gender differences in migraineurs with PTSD is warranted.
The NCS-R has several strengths. First, this study permitted assessment of the association between migraine and PTSD in a large, population-based sample, not subject to the biases inherent in clinical samples and one providing sufficient power to investigate the extent to which the association between migraine and PTSD was attributed to comorbid mood disorder and alcohol and drug abuse.
Second, both the headache and mental disorders were determined based on standardized diagnostic criteria. Third, the NCS-R allows the differentiation of a primary psychiatric disorder from secondary psychiatric disorders. For example, whereas other studies evaluating GAD often broadly include all participants with GAD from any cause (which can result in the diagnosis being given even if the GAD was secondary to PTSD or in response to the presence of a fatal illness), the NCS-R allows for a distinction of primary versus secondary disorders.
Several limitations of the current study should be considered when interpreting our results. First, headache diagnoses were only collected for those with headaches during the previous year. By contrast, mental disorders were characterized for both lifetime and one-year periods. Second, one of the ICHD criteria was not included; however, it is likely its exclusion did not significantly impact our findings as it resulted in a loss of only 25 participants. Third, the prevalence of migraine is lower in the NCS-R than expected in the general population; this may be due to differences in survey methodology and sampling strategies as noted previously (1). However, the major reason for this disparity is likely related to the headache screener question which was based on persons having “frequent or severe” headaches and which likely eliminated those with having less severe or infrequent headaches that nevertheless would fulfill migraine criteria from being included. Finally, although the headache questions are based on the ICHD-II criteria the NCS-R headache questions have not been validated for migraine as compared to a physician diagnosis of ICHD-II migraine.
Statistical analysis
Statistical analysis of data was performed by Andrea L. Rosso.
Footnotes
Acknowledgements
The National Comorbidity Survey Replication (NCS-R) is supported by the US National Institute of Mental Health (NIMH; U01-MH60220) with supplemental support from the National Institute of Drug Abuse, the Substance Abuse and Mental Health Services Administration, the Robert Wood Johnson Foundation (Grant #044780) and the John W. Alden Trust. Collaborating NCS-R investigators include Kathleen Merikangas (co-principal investigator, NIMH). The views and opinions expressed in this report are those of the authors and should not be construed to represent the views of any of the sponsoring organizations, agencies or the US government. Dr. Peterlin had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Dr. Peterlin has been a consultant for OrthoMcNeil and Pfizer, is on the speakers' bureaus for GlaxoSmithKline (GSK), Endo and Merck, has grant support from GSK, has an intellectual property patent for the use of adiponectin-modulating drugs for migraine and is an associate editor for the journal Headache. Dr. Sheftell has served on advisory boards for GSK, Merck, MAP, NuPath, Optinose, and Novartis, is on the speaker’s bureaus for Merck and GSK, has received grant support from Pfizer and has an intellectual property patent for montelukast and leukotriene modifiers for migraine and neuroinflammatory disorders. He is an associate editor for the journal Headache Currents. Dr. Mossey is an associate editor for the journal Pain Medicine. A. Rosso, Dr. Libon and Dr. Merikangas have no conflicts of interest or disclosures.
Comparison of NCS-R Headache Questionnaire to ICHD-II criteria (Primary differences between the two are noted in italics.)
| ICHD-II criteria | NCS-R questionnaire |
|---|---|
| A. At least 5 attacks fulfilling criteria B–D | About how many days out of 365 did you have a headache in the past 12 months? |
| B. Headache attacks lasting between from 4–72 hours | About how many minutes or hours do your headaches usually last? |
| C. Headache has at least two of the following characteristics | |
| 1. Unilateral location | Is the headache pain ever on only one side of your head? |
| Do you ever have pain behind one eye during your headaches? | |
| 2. Pulsating quality | Does the pain ever throb or come in pulses during your headaches? |
| 3. Moderate or severe pain intensity | On a scale from 0 to 10, where 0 is “no pain” and 10 is “pain as bad as you can imagine”, what number best describes your headache pain |
| 4. Aggravation by or causing avoidance of routine physical activity | This was not asked on the NCS-R questionnaire. |
| D. During headache at least one of the following: | |
| 1. Nausea and/or vomiting | Are your headaches ever accompanied by nausea or vomiting? |
| 2. Photophobia and phonophobia | Are your headaches ever accompanied by increased sensitivity to light or sound? |

NCS-R = National Comorbidity Survey Replication. ICD-II = International Classification of Headache Disorders, Second Edition.