
Abstract
Introduction: Cluster headache is characterized by severe attacks of unilateral pain, but many patients experience symptoms more commonly associated with migraine such as persistent pain.
Patients and methods: We evaluated cluster headache patients using a questionnaire and chart review to determine clinical characteristics.
Results: Twenty-four of 50 subjects reported interictal pain outside of their acute attacks. Sixteen reported persistent pain more than half the time while in cycle. Unlike acute attacks, this pain was generally mild.
Conclusions: Subjects with persistent interictal pain were more likely to have chronic cluster, allodynia, and suboptimal response to sumatriptan, suggesting that interictal pain in cluster headache may predict a more severe disease process.
Introduction
Cluster headache is a primary headache disorder characterised by unilateral headache with autonomic symptoms lasting 15–180 min if untreated (1). Patients with cluster headache generally present for evaluation of severe headache, and many experience phenomena common in other headache disorders such as migraine. Cluster headache patients may experience symptoms such as aura (2), nausea, or photophobia and phonophobia (3) that may cause diagnostic confusion or delay diagnosis (4). Cluster headache patients may have allodynia between (5) or during (6) acute attacks. A recent study suggests many chronic cluster headache patients suffer from pain between acute cluster attacks (7) suggesting an overlap with chronic migraine. This case series describes the phenomenon of interictal pain in cluster headache, and discusses if the presence of interictal pain suggests a more severe disease process.
Patients and methods
This study was approved by the Institutional Review Board of Thomas Jefferson University. We studied adults (age >18 years) from the Jefferson Headache Center with either episodic or chronic cluster headache, as defined by International Classification of Headache Disorders (ICHD-2) criteria (1). To avoid recall bias, we excluded all patients with episodic cluster headache not currently in cycle. Patients with highly atypical features, proven secondary cause of headache, frequent opiate use, or an unclear diagnosis were excluded. We used a prospective questionnaire at the time of an office visit to establish diagnosis and disease duration, obtain demographic information and preventative medications, and determine pain intensity during and between attacks. We confirmed medications and obtained height and weight from patient records. We asked patients, if known, for their perceived response to acute treatments (including subcutaneous sumatriptan, oxygen and corticosteroids) giving them a forced choice of a treatment ‘helping a lot’, ‘helping a little’, or ‘not at all’. We screened for the presence of interictal pain during their cluster cycles. If present, we asked patients, again with a forced choice, to state if the pain was: (i) all the time; (ii) more than half the time; (iii) less than half the time; (iv) short and brief (less than 10 min); or (v) jabs of pain lasting seconds between attacks. We asked patients to describe, in their own words, this pain between attacks. Patients rated this pain severity using an 11-point pain scale (0–10, where 10 is the most severe). We screened patients for the presence of allodynia during and outside of attacks using a validated questionnaire (8). We determined the presence of brush allodynia outside of attacks using a clinical method used previously in migraine, with results similar to quantitative sensory thresholds (9). This involved folding a 4 × 4 inch gauze pad in half and brushing it lightly over the patient’s skin 10 times at a rate of 2/s on each side of the forehead (V1).
For comparison, we divided patients into groups of those with interictal pain more than half the time, and those with no pain or pain less than half the time. We considered this first group to have persistent pain outside of attacks. After collecting the data with the questionnaire, we calculated data including sex, mean and median age, and body mass index (BMI). We used descriptive statistics to perform statistical analysis and Fisher’s-exact test to determine differences between groups.
Results
Fifty subjects participated in this study including 39 (78%) men and 11 women (22%). The mean age was 46.5 years (median, 47 years; range, 21–67 years). Thirty-eight patients met ICHD-2 criteria for ECH and 12 for CCH. All patients had more than one autonomic symptom during acute attacks and the majority (36/50; 72%) reported agitation or restlessness. Seven subjects reported a personal history of migraine, and seven reported experiencing other headache types including tension-type and sleep apnoea headaches. The majority (43/50; 86%) of patients were on one or more medications for cluster headache prophylaxis including verapamil (37/50; 74%), topiramate (11/50; 22%), divalproate (6/50; 12%), melatonin (4/50; 8%) and lithium (1/50; 2%). The mean duration of cluster headache (time since first ever attack) was 17.4 years (median, 15 years; range, 0–47 years). Thirty-eight subjects (76%) reported disease duration of 10 years or more.
Twenty-seven of 50 subjects (54%) reported having interictal pain. Of these, the majority (16/27; 59%) had pain more than half the time, with 10 subjects reporting some degree of pain all the time. Ten subjects reported interictal pain less than half of the time, with two subjects reporting jabs of pain lasting only seconds, and another two noting brief pain for less than 10 min.
Unlike cluster headache attacks, this pain in between attacks was generally mild. Sixteen subjects rated their pain between attacks as 1–3 in severity on the 11-point pain scale, seven between 4–6, and three between 7–10. Patient descriptions of this interictal pain included: ‘my head feels cloudy, eyes swell and is sore to touch’, ‘dull, like a woodpecker on the temple’, ‘little twinges of pain over the right temple and feeling in a daze’, ‘bad neck pain and pain left over from my head that lingers’, and ‘mild pain and tenderness over right temple’. In most cases, this pain was ipsilateral to cluster headache attacks (24/26; 92%). Unlike during their cluster headache attacks, three patients reported neck pain was more prominent than head pain interictally. Subjects denied significant autonomic symptoms during periods of between attacks other than congestion.
Disease features and response to acute treatment
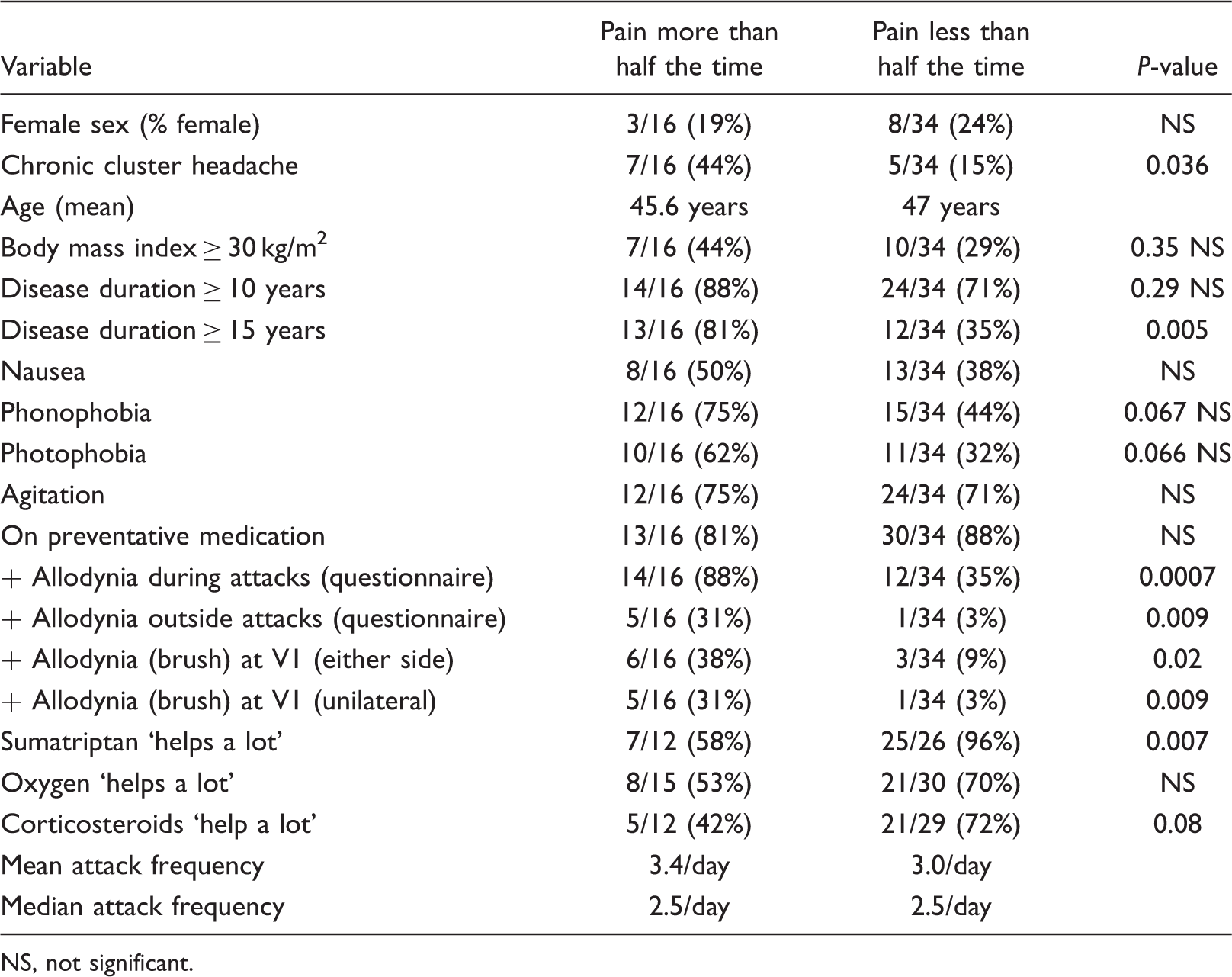
NS, not significant.
Of subjects that had used sumatriptan injections, subjects with persistent pain were less likely to agree that the treatment ‘helps a lot’. There was a trend towards decreased effectiveness of steroids (Table 1). Subjects with allodynia by questionnaire but without persistent interictal pain usually reported that sumatriptan ‘helps a lot’ (8/9) unlike those with persistent pain and allodynia (4/10).
Discussion
Pain that persists between attacks in cluster headache was common in this study. These subjects with cluster headache and persistent interictal pain were more likely to have other markers of increased disease severity such as chronic cluster headache, suboptimal response to sumatriptan, cutaneous allodynia during and outside of attacks, and disease duration of 15 years or more. The correlation between persistent pain and these clinical features suggests that interictal pain may predict disease severity. Factors influencing successful response to acute treatment in cluster headache are poorly understood, although a previous study suggested advanced age, nausea and restlessness were negative predictors of response (10). There was a trend towards increased photophobia and phonophobia, but otherwise this study does not support the concept that cluster headache patients with interictal pain have more migraine features.
This study suggests physicians treating cluster headache need to ask about the presence of interictal pain. Cluster headache patients usually present for evaluation of their severe headaches, not the ‘annoying’ pain that occurs outside of attacks.
The majority of patients with interictal pain reported only mild or moderate pain during episodes which was different than their typical cluster headache attacks. Most patient descriptions of interictal pain were not specific for cluster headache, except that the pain was usually unilateral. One possibility is that frequent headache attacks may lead to more frequent interictal pain (11). The concept of pain memory from repeated noxious stimuli has been postulated as a mechanism for persistent pain in patients with hemicrania continua (12). Pain memory may help explain pain between attacks in cluster headache and why both chronic cluster headache subjects and those with a long history of attacks were more susceptible to interictal pain in this study.
Allodynia in this study was less common than in migraine studies using similar methods or quantitative sensory testing, but was more common in the persistent pain group. We tested for dynamic mechanical allodynia between attacks but the 8-item questionnaire screened for symptoms of thermal and static mechanical allodynia during and outside of attacks. In this study, cluster headache patients with allodynia usually still experienced relief with acute treatment, especially if they did not experience persistent pain. There are increasing reports and studies of allodynia in cluster headache (13,14), which suggest central sensitization occurs, but another study using quantitative sensory testing did not confirm this (15). In pain conditions, repeated attacks of pain may lead to activation of microglia and production of prostaglandins by cyclooxygenase-2 resulting in allodynia (16). Larger studies are needed to clarify the prevalence and significance of allodynia in cluster headache, or at least if it exists in a minority of patients. For refractory cluster headache patients with interictal pain or allodynia, it may be worth using cyclooxygenase-2 inhibitors (17) or preventatives that inhibit allodynia, such as gabapentin (18,19), for optimal results.
Study limitations
This study was limited due to the fact that the great majority of subjects were on prophylactic medication. Preventatives may influence allodynia and can influence disease severity and attack frequency. Verapamil, the most commonly used preventative, commonly causes headache as a side effect. Recent studies suggest that frequent abortive use in cluster headache can cause deterioration and constant headache (20). Medication overuse could explain some of our findings and we did not specifically exclude subjects with possible triptan overuse. Although all patients had attacks which met criteria for cluster headache, constant unilateral headache with autonomic features suggests hemicrania continua. The majority of patients with persistent pain did not receive a sufficient course of indomethacin to rule out hemicrania continua and it is unclear if pain between attacks in cluster headache would respond to indomethacin.