
Abstract
The aim of this study was to investigate the prevalence and characteristics of typical aura without headache (TAWH) in Japan. We distributed a self-report questionnaire comprising seven items. Of 1914 cases, the number of patients who provided valid answers was 1063. They included 1063 out-patients with 81 of these patients positive in the ID migraine screener Japanese version. TAWH was diagnosed in 35 patients (3.2%), aged 23–87 years, and included 12 males and 23 females. The age of patients with TAWH showed a biphasic distribution (20–39 years and 60–69 years), similar to the age distribution of all patients. Migraine with aura was diagnosed in 67 patients (6.3%) and showed a monophasic age distribution (40–49 years). These data suggest that TAWH is not a rare headache type in clinics especially in a setting of general ophthalmology clinics, and some patients of migraine with aura may transform to TAWH with ageing.
Introduction
Migraine is one of the most common neurological disorders and is observed in about 8.4% of the population in Japan (1). Migraine attacks are characterised by unilateral, throbbing and moderate-to-severe headache lasting 4–72 h, typically accompanied by nausea and photo- and phonophobia (2). In approximately 20% of patients, the migraine can also be preceded by transient neurological symptoms (aura) that usually develop gradually over >5 min and last for <60 min. Auras are most frequently visual (>90%), but may also involve other sensory symptoms (pins and needles, numbness), hemiparesis or speech deficits (2). To date, the trigger mechanisms of migraine aura/cortical spreading depression (CSD) and the question of whether or not CSD is a prerequisite for developing migraine headache remain controversial (3).
Typical aura without headache (TAWH) is diagnosed according to the operational diagnostic criteria of The International Classification of Headache Disorders (ICHD)-II (2). The reported prevalence of TAWH is 0.2–6.5% (4,5). However, the prevalence and characteristics of Japanese patients with TAWH are not known. In their study of 53 patients diagnosed as migraine with aura (MWA) followed-up for 16 years, Erikson et al. (6) reported seven (13%) patients who had TAWH. Patients with TAWH often visit an ophthalmology clinic since they only develop visual symptoms without any headache. Therefore, to determine the prevalence of TAWH in Japan, this study was performed in ophthalmology clinics and a university hospital. We investigated the prevalence and characteristics of TAWH and MWA with a special focus on the age distribution.
Subjects and methods
Diagnostic criteria for typical aura without headache according to ICHD-II

The chi-squared test with 5% level of significance and 95% confidence limit was used.
Results
Although 1914 subjects were included in the study, 851 patients were excluded due to incomplete answers in the questionnaire. The final analysis was based on data from 1063 (55.5%) subjects (Figure 1). Of the 1063 subjects, 348 were males (33%) and 715 were females (67%; Figure 2). The mean ± SD age of the subjects who completed the questionnaires was 51.3 ± 18.9 years (males, 53.4 ± 18.6 years; females, 50 ± 18.8 years; median, 54 years; range, 6–95 years). The ID migraine screener Japanese version was positive in 81 subjects. Visual or/and sensory aura as the prodromal symptom was reported by 356 of the 982 screening negative cases. We excluded 53 subjects who suffered from cerebrovascular disease, history of weakness and headache with aura. Of the 303 (28.5%) subjects, 172 (16.2%) experienced visual aura, 60 (5.6%) visual and sensory auras, and 71 (6.7%) sensory aura. Finally, of the 1063 subjects who completed the study, only 35 (3.2%) were diagnosed with TAWH according to ICHD-II criteria (Figure 1).
Flow diagram of selection of patients who visited the ophthalmology out-patient clinics. Of all 1063 subjects who completed the study, only 35 (3.2%) were diagnosed with TAWH. Age distribution of 1063 patients who visited the ophthalmology out-patient clinics and answered questionnaires. Of the 1063 subjects, 348 were males (33%) and 715 were females (67%). The mean ± SD age of the subjects who completed the questionnaires was 51.3 ± 18.9 years (males, 53.4 ± 18.6 years; females, 50 ± 18.8 years).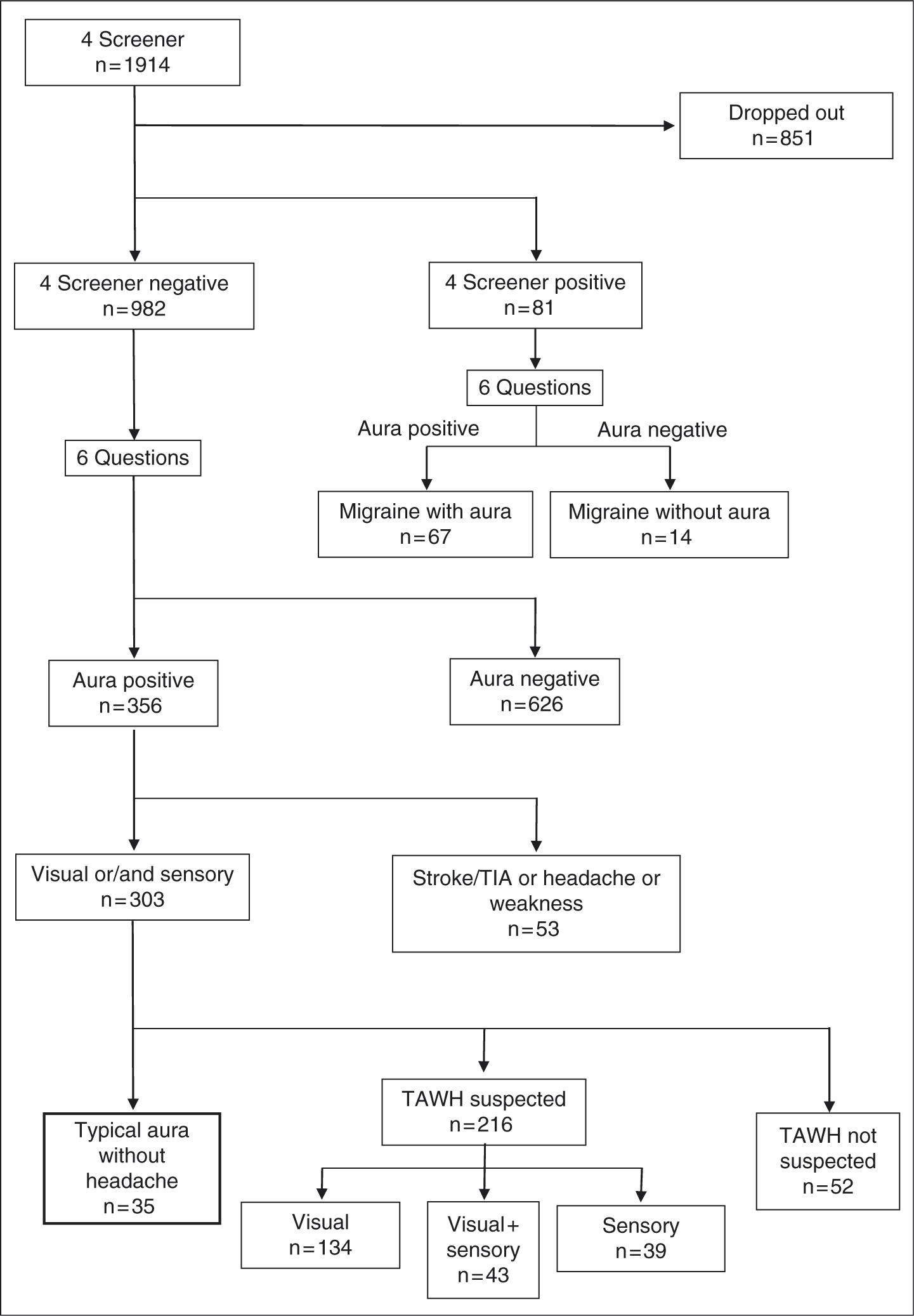

The 35 patients comprised 12 males and 23 females (Figure 3A), with a male:female ratio of 1:1.9, and a median age of 47 years (range, 23–87 years). Among the 35 patients with attacks of TAWH, 11 had visual aura only, 9 had sensory aura only, and 15 patients had both visual and sensory aura. Sixty-seven patients (9 males and 58 females) had MWA (6.3%; Figure 3B), with a male:female ratio of 1:6.4, and median age of 42 years (range, 22–89 years). Furthermore, 14 patients (all females) had migraine without aura (MWOA; 1.3%), with a median age of 37 years (range, 25–53 years). The median age of patients of the MWA and TAWH was the fourth decade (42 years and 47 years). Although the age of patients with TAWH showed a biphasic distribution, similar to the age distribution of all patients (the second to third and sixth decades), that of MWA showed a monophasic distribution at third-fourth decade.
Visual and sensory auras were the most frequent symptoms (43%) in patients with TAWH (n = 35), followed by visual aura (31%) and sensory aura (26%). Furthermore, visual and sensory auras were the most frequent symptoms (48%) in MWA (n = 67), followed by visual aura (34%) and sensory aura (18%). The frequency of visual and sensory auras in TAWH was not different from those in MWA.
Discussion
This is the first epidemiological study of TAWH according to ICHD-II in Japan. The prevalence of TAWH in this study was 3.2%, indicating a high prevalence compared with that reported previously in neurology clinics of 0.2% (4,9). To determine the reason for the high prevalence in our study, we analysed the sex and age distribution in the two studies. The Danish studies (4,9) were conducted in 4000 patients aged 40 years, and included 3000 males and 1000 females (M:F ratio, 3:1). The results of our study indicated more females are affected with TAWH than those reported in the above two studies (4,9). Furthermore, the age distribution was different in the two studies. In our study, the 1063 patients comprised 348 males and 715 females with M:F ratio of 1:2, and a median age of 54 years (range, 6–95 years). The prevalence of MWA was 6.3%, with 0.8% males and 5.5% females, while that of TAWH was 3.2% with 1.1% males and 2.1% females. The high prevalence of TAWH in our study compared with the previous report (4) may be related to the relatively younger age of patients in that study (40 years) compared with the present investigation. Furthermore, Amos and Fleming (10) reported that TAWH is a type of migraine that seems to be reported more frequently in ophthalmology than in neurology or general medical practice. Their other report in ophthalmology (5) described that, of the 1000 primary eye care patients surveyed, 6.5% had experienced visual sensations consistent with TAWH.
In our study, the male:female ratio was in favour of females in MWA and TAWH, and the median age of MWA and TAWH was 40–49 years in both groups. Our data suggest a two-level age distribution of patients with TAWH (20–39 years and 60–69 years; Figure 3A), similar to the age distribution of all patients, compared with the narrow age distribution of MWA (30–49 years; Figure 3B). Our results are similar to those of another survey study of ophthalmology clinics (5).
(A) Age distribution of patients with typical aura without headache. The median age of patients of the typical aura without headache was the fourth decade. The age of patients showed a biphasic distribution; the second to third and sixth decades, similar to the age distribution of all patients. (B) Age distribution of patients with migraine and aura. The median age of patients of the migraine and aura was the fourth decade. The age of patients showed a monophasic distribution at third-fourth decade.
Hedges (11) reported 7 of 43 patients (12%) with TAWH between 5–30 years of age; 18 of 43 patients (42%) between 30–50 years; and 18 of 43 patients (42%) between 50–80 years of age. The age of patients with TAWH reported in our and Hedges’ studies seems to cover a broad span.
Eriksen et al. (6) reported the results of a 16-year follow-up study designed to assess the long-term outcome of MWA. At follow-up, attacks had ceased (no MWA for 2 years) in 19 (36%) of 53 patients. Similarly, Colongo et al. (12) conducted a 10–20 year follow-up study that assessed the long-term outcome of MWA. They identified eight patients (11%) among 81 who switched from MWA to TAWH. Mattsson et al. (13) reported that the life-time prevalence of migraine headache in 728 female was 31.5% whereas the 1-year prevalence was 18.0%. The estimated decline in the prevalence of active migraine headache in their study was 50% per decade, suggesting that the decline in the prevalence of active migraine headache with age was due to a decrease in pain intensity. Although the prevalence of visual aura was 3.8% and this rate did not change with age, the intensity of the headache decreased slightly with age (40–49 years, 4.21%; 50–59 years, 4.2%; 60–74 years, 3.1%) and the disability identified by the Visual Analogue Scale showed a clear decline with age (40–49 years, 6.5; 50–59 years, 5.0; 60–74 years, 2.0). The present study showed a decline in the prevalence of active migraine headache with age but not in the prevalence of active migraine visual aura. In addition, the headache intensity decreased after 50 years of age, whereas visual aura does not seem to decrease even in advanced age. Unfortunately, our study design did not include follow-up investigation; however, the results suggested that MWA might shift to TAWH with ageing.
Study limitations
Our study has many limitations. First, it has been suggested that the diagnosis of MWA is difficult (14). For example, photophobia can be easily mistaken for a migraine aura. For this reason, only interviews by physicians with experience in headache diagnosis can be considered valid in nosographic studies of MWA (15–17). In this regard, Russell and Olesen (17) suggested that participants must be interviewed by a physician. Our study was not designed to include such interviews and the diagnosis was based on the response to questionnaires. Second, to determine the prevalence of TAWH in Japan, this study was conducted in several ophthalmology clinics and a university hospital. In Japan, the national health insurance system provides free access for all patients with disturbance of visual acuity to all clinics, including ophthalmology clinics and also university hospital clinics. Third, Di Piero and colleagues (18) indicated that one striking feature of migraine is the difference between the estimated migraine prevalence and the actual number of migraineurs consulting their general practitioners. Taking this issue into consideration, our sampling method using ID migraine plus six other questions may have been somewhat biased.
Conclusions
The prevalence of TAWH is considered common in ophthalmology and our results suggest that TAWH seems to increase with ageing, emphasising the need for programmes that can deal with this issue in the future.