
Abstract
Reversible cerebral vasoconstriction is a rare and poorly understood syndrome, without clear diagnostic criteria. It has been described in association with multiple disorders, but has only been reported rarely in the setting of carotid artery dissection and, to our knowledge, never before in association with renal artery stenosis.
Keywords
Case report
A 44-year-old woman was referred for investigation of headache, confusion, left hemiparesis and visual disturbance. She had developed predominantly occipital headache 3–4 weeks previously, which was thunderclap in onset and had subsequently fluctuated in severity. She had also been diagnosed with hypertension at this time, which remained poorly controlled despite treatment with atenolol and lercanidipine. She had visited a chiropractor after developing the headache and undergone neck manipulation, without improvement. At 2–3 weeks post headache onset, she became confused and several days later developed left-sided visual loss and left leg weakness. The patient was a tobacco and marijuana smoker but denied amphetamine use in the last 20 years. A computed tomography (CT) head scan was normal and lumbar puncture revealed normal cerebrospinal fluid (CSF) opening pressure, biochemistry and cell counts.
On arrival, blood pressure was 191/99 mmHg. Neurological examination revealed left homonymous inferior quadrantanopia, pyramidal weakness of the left arm and leg, extensor left plantar and features of both dominant and non-dominant parietal dysfunction (dyscalculia, left–right disorientation, finger agnosia and constructional apraxia).
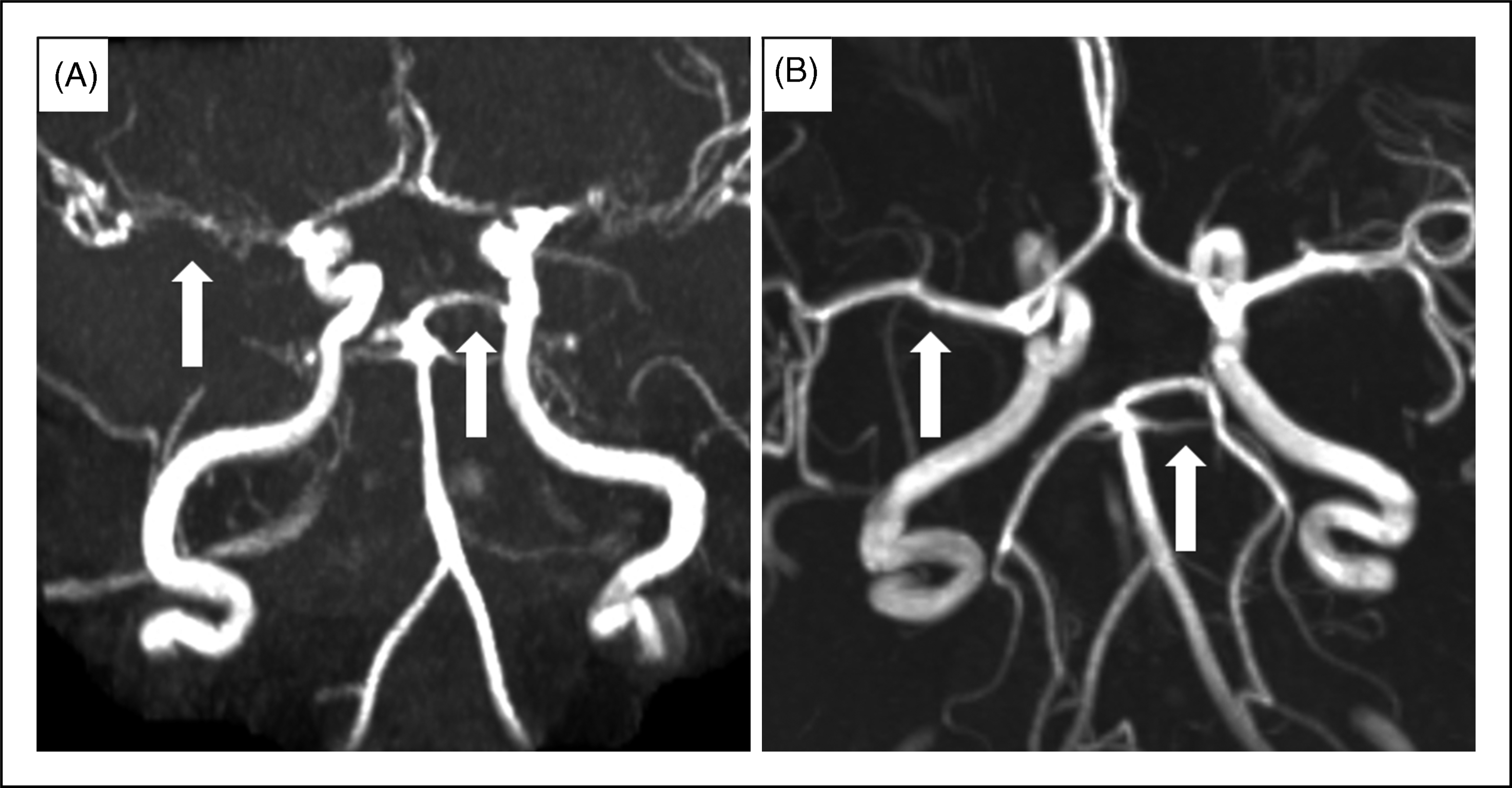
Magnetic resonance imaging (MRI) of the brain showed bilateral cortical and subcortical areas of restricted diffusion in watershed regions, particularly involving the posterosuperior parietal lobes and corresponding to abnormalities on fluid-attenuated inversion recovery (FLAIR). There was no evidence of subarachnoid haemorrhage. Magnetic resonance angiography (MRA) showed left internal carotid artery dissection extending from first and second cervical vertebrae to the base of the skull, and proximal narrowing of the anterior, middle and posterior cerebral arteries bilaterally (Figures 1 and 2A).
(A) Diffusion-weighted image showing restricted diffusion in parietal lobes. (B) T1 fat saturation image showing dissection of left internal carotid artery. (A)Magnetic resonanceangiography (MRA) showing proximal narrowing of the anterior, middle and posterior cerebral arteries bilaterally. (B) MRA circle of Willis at 3 months post-symptom onset showing normal calibre intracranial vessels.
She was commenced on intravenous heparin and methylprednisolone and blood pressure was maintained below 160 mmHg systolic with atenolol, lercanidipine and perindopril. She deteriorated over the next 48 h, with severe headache, akinetic mutism, bilateral hypertonia, hyper-reflexia and extensor plantars. EEG showed diffuse slowing consistent with an encephalopathic process and CT brain scan excluded cerebral haemorrhage.
The deterioration in her condition was attributed to progressive cerebral ischaemia secondary to severe vasoconstriction of multiple cerebral arteries. She was commenced on intravenous nimodipine and, within 24 h of starting treatment, had resolution of headache, normalisation of tone in upper limbs and improvement in spontaneous speech and movement. Over the next 3 months, there was gradual, but complete, resolution of neurological symptoms and signs. During this time, she was managed with anticoagulation and lercanidipine, with good control of blood pressure, and steroids were slowly weaned.
Repeat MRI and MRA brain at 3 months post-symptom onset showed normal calibre intracranial vessels (Figure 2B). Screening for causes of secondary hypertension with renal CT angiography (CTA) identified a tight, non-atherosclerotic stenosis of the mid to distal segment of the right renal artery, with an area of post-stenotic dilatation distal to this and abrupt truncation of the middle renal artery.
Discussion
We discuss the case of a 44-year-old woman who presented with headache and progressive neurological deterioration, with MRA showing severe vasoconstriction of multiple cerebral arteries. There was complete clinical and radiological resolution, which is consistent with reversible cerebral vasoconstriction syndrome (RCVS).
There are no established definitive diagnostic criteria for RCVS, but a recent review (1) proposed the following critical elements for diagnosis:
Transfemoral angiography or indirect CTA or MRA documenting multifocal segmental cerebral artery vasoconstriction. No evidence for aneurysmal subarachnoid haemorrhage. Normal or near-normal cerebrospinal fluid analysis (protein level <80 mg%, leukocytes < 10 mm3, normal glucose level). Severe, acute headaches, with or without additional neurological signs or symptoms. Reversibility of angiographic abnormalities within 12 weeks after onset.
The largest case series to date, carried out by Ducros et al., (2) involved 67 patients and used different diagnostic criteria to identify patients:
Unusual, recent, severe headaches of progressive or sudden onset, with or without focal neurological deficit and/or seizure. Cerebral vasoconstriction assessed by MRA or conventional angiography, with at least two narrowings per artery on two different cerebral arteries. Disappearance of arterial abnormalities in less than 3 months.
The lack of consensus regarding diagnostic criteria relates, in part, to poor understanding of the pathophysiology of this condition, as well as the heterogeneous range of disorders which have been described in association with it. These disorders include pregnancy, pre-eclampsia, head injury, unruptured cerebral aneurysm, bronchial carcinoid, phaeochromocytoma, hypercalcaemia, porphyria, reversible posterior leukoencephalopathy, carotid endarterectomy and vasoactive drug use (1). The series of Ducros et al., (2) demonstrated that more than 50% of patients had a history of previous use of these substances, including cannabis, cocaine, amphetamines, nasal decongestants, selective serotonin re-uptake inhibitors and nicotine patches.
The patient described in this case report had multiple potential contributing factors to RCVS, including marijuana use, internal carotid artery dissection, hypertension and renal artery stenosis. There have been two reported cases of internal carotid artery dissection and RCVS (3,4). The first was a 31-year-old woman who developed post-partum RCVS complicated by seizures and was found to have left internal carotid artery dissection (3). This was assumed to be incidental. Arnold et al. (4) subsequently reported the case of a 35-year-old woman with post-partum RCVS, in association with dissection of left internal carotid and right vertebral arteries. Additionally, they described a 27-year-old woman with post-partum RCVS, reversible posterior leukoencephalopathy and right vertebral artery dissection. Four previous cases of RCVS in association with vertebral artery dissection had been identified in the series of Ducros et al., (2) where the possibility of a causal relationship between cervicocephalic artery dissection and RCVS was first raised. Our case provides further evidence for an aetiological link.
RCVS is thought to be related to disturbance in regulation of cerebral vascular tone (5). Given these reported cases and also that ipsilateral RCVS has been reported in the setting of carotid endarterectomy (6), it is more likely that carotid dissection preceded cerebral vasoconstriction in our patient’s case than vice versa – despite her chiropractic treatment subsequent to headache onset (a known precipitant of cervicocephalic dissection) (7). It has been postulated that excessive sympathetic activity or an abnormal vascular response to circulating catecholamines underlies RCVS (8). The association in our patient of RCVS and renal artery stenosis, a known cause of increased sympathetic activity (9), further supports this hypothesis.
Atherosclerotic disease is unlikely as the cause of renal artery stenosis in our patient, given her age, few cardiovascular risk factors prior to developing hypertension, and the location of the stenosis, which usually involves the ostium and proximal main renal artery in atherosclerosis (10). Fibromuscular dysplasia is a non-atherosclerotic, non-inflammatory vascular disease of unknown cause, which most frequently affects the renal (60–75% of cases) and carotid or vertebral (25–30% of cases) arteries (11). Renal angiography most commonly shows beading of the renal artery, with involvement in middle to distal portions, but less frequently can be a focal stenosis (10).
Fibromuscular dysplasia also tends to affect the middle and distal portions of the carotid and vertebral arteries at the level of the first and second cervical vertebrae, and CTA typically shows beading, but can demonstrate focal concentric stenoses or aneurysms (12). Up to 15% of patients with spontaneous dissection of the vertebral and carotid arteries have angiographic changes of fibromuscular dysplasia (13). Our patient did not have typical beading on MRA; the location of her internal carotid artery dissection was consistent with fibromuscular dysplasia, although most idiopathic carotid artery dissections also occur in this location (14). An underlying disorder of large arteries is suggested by co-incident, dual, non-atherosclerotic lesions. Therefore, although not proven, a parsimonious explanation for her condition could be fibromuscular dysplasia affecting renal and carotid arteries, and that dissection of her carotid artery and stenosis of her renal artery acted synergistically to produce RCVS (Figure 3). Alternatively, the arterial lesions may have both been due to inherited connective tissue abnormalities or, less likely, be co-incidental.
Possible causes of reversible cerebral vasoconstriction syndrome (RCVS).
Treatment for RCVS is aimed at vasospasm and usually consists of calcium channel blockers and high-dose glucocorticoids, although given the reversible nature of RCVS, the benefit of this therapy on outcome has not been clearly established (2,15,16). If vasoactive substances are thought to have played a role, patients are advised to avoid these in future. As with the case described above, RCVS tends to have a good clinical outcome, with death and relapse rare occurrences (1,2,17).
Most other causes of severe headache and neurological deficit, such as subarachnoid haemorrhage, may be differentiated early on with neuro-imaging and lumbar puncture. Cerebral vasculitis remains an important differential diagnosis to consider, especially as its prognosis is much poorer than RCVS and patients require long-term immunosuppression. This condition tends to present with a more insidious onset than RCVS and has high rates of abnormal CSF findings, but can be difficult to distinguish from RCVS on initial angiography (18). The reversibility of vasoconstriction over days to weeks has been suggested as the best feature to distinguish RCVS from cerebral vasculitis (1).
Conclusions
Reversible cerebral vasoconstriction syndrome remains a diagnostic challenge but, nonetheless, should be considered in patients presenting with severe headache and neurological deficits. The case described above not only demonstrates the multifactorial nature of this condition, but describes a new association with renal artery stenosis and strengthens the proposed aetiological link with cervicocephalic arterial dissection.