
Abstract
Headache is an underestimated burden on general health and social functioning. Accompanying symptoms of headache episodes might influence this impact. In a survey in a headache population in Luxembourg on the social and emotional impact of headaches, accompanying symptoms of headache episodes were evaluated. In 1909 participants with episodic (<15 days per month) headaches (77.1% women), visual symptoms (52.4%) and dizziness (51.1%) were frequent accompanying symptoms of headache episodes. Visual symptoms and dizziness were each independently associated with migraine in both genders and independently associated with greater headache-related disability (scored on the Migraine Disability Scale [MIDAS]), more severe depression, and higher disability as measured by the disease-independent World Health Organization Disability Assessment Schedule (WHODAS). We found that dizziness is a frequent accompanying symptom of headache, particularly in migraine. The presence of dizziness was found to have an exacerbating impact on disability and depression associated with headaches. The effect of dizziness was comparable in magnitude and independent from the presence of visual symptoms.
Introduction
Most headaches are so-called primary headaches and considered a benign medical condition. Nevertheless, headache is often a chronic recurrent condition with a negative impact on social and professional functioning (1,2)
Headache (3) and dizziness (4) both have a high prevalence. While in the International Classification of Headache Disorders (ICHD) accompanying symptoms such as photo- and phonophobia, and also visual disturbances in migraine with aura, play a major role, this is not the case for non-specific disturbances of balance, most commonly called ‘dizziness’. Dizziness is a term used to describe a sensation of disturbed orientation in space, whereas vertigo describes an illusion of movement without specific localizing value of a disturbance in the vestibular system (5). The term dizziness is often used in a broad sense of the word by both patients and medical professionals, and can include feelings of vertigo (6).
In a community study in a working-age population from general practice lists in the UK, the prevalence of dizziness was 20%, more commonly in women; about one-half of these patients had handicapping dizziness with an impact on working ability and an association with anxiety (7). In the German National Telephone Health Interview Survey 2003 (GNT-HIS) (4), lifetime prevalence of moderate-to-severe dizziness or vertigo was found in 29.5% of the adult population.
Many investigators (8,9) have described a relationship between vertigo and migraine. Whereas sensory hypersensitivity to visual and auditory stimuli (photophobia and phonophobia) are part of the diagnostic criteria for migraine, vestibular hypersensitivity to movement is not considered at all. In the second edition of the ICHD (2004) (10), vertigo is only part of two diagnostic entities: basilar-type migraine (1.2.6), where vertigo is accepted as an aura symptom only if at least one of eight other listed symptoms is also present, and benign paroxysmal vertigo of childhood (1.3.3).
Hypotheses on the underlying pathophysiology of vertigo in basilar and vestibular migraine are a functional vestibular tone imbalance by asymmetric activation or deactivation of vestibular neuronal activity at brain-stem level (11,12) and possibly cortical spreading depression involving the vestibular cortex (13).
The data analyzed in this paper are part of an epidemiological study investigating the impact of headache and accompanying symptoms on professional and social functioning. Based on clinical experience, the authors hypothesized that disturbances of balance associated with headaches might in fact be prevalent and play a pronounced role in headache-associated disability. To approach this question in the subpopulation of episodic headache sufferers, the frequency and functional impact of dizziness in association with headache were evaluated. Visual symptoms were incorporated into the analysis to compare the prevalence and impact of dizziness with another widely accepted symptom associated with migraine.
Methods
A validated, self-administered questionnaire–based investigation (BURMIG) was conducted in a headache population of Luxembourg during 2005; the questionnaire and the data on its validation are published elsewhere (14). Because of the multicultural composition of the population, it was available in four languages (German, French, English and Portuguese). The BURMIG study was a two-phase cross-sectional survey of prevalence and impact of headache. The first phase was a prevalence study for headaches with a population-generated sample of 6500 people, with 3520 questionnaires returned. Of these, 2242 were headache sufferers, 728 of whom agreed to fill in the impact questionnaire in the second phase. An additional headache population was recruited in hospitals, pharmacies and surgeries, volunteering to participate. The two recruitment methods allowed comparing the characteristics of the second population with the population-based sample.
The questionnaire contained 41 items on professional and social life, affect, stigma, use of medication, use of health care resources, coping strategies and perceived needs for improving the current situation. It contained questionnaire blocks validated in the four languages used: (1) WHODAS II, a tool to assess disability independently from the underlying disease, which exists in different versions (for the purpose of this study, the 12-question version was chosen (15); (2) the MIDAS questionnaire, which is targeted to assess disability related to headache (16); (3) the PHQ9 (Patient Health Questionnaire), assessing depression (17); and (4) Migraine ID, for identification of migraine as opposed to other headaches (18).
One block of questions asked about associated symptoms before, during and after the headache episodes: dizziness, but also mood changes, speech difficulty, unusual hunger, visual disturbances (blurred or altered vision), swollen limbs and other symtoms.
To ask about symptoms arising from the vestibular system in a wider sense, the following terms were used: in English “feeling dizzy”, in German, “Benommenheit/Schwindel”, in French, “sensation de vertige”, in Portuguese, “tonturas”.
Statistical methods
Descriptive statistics consisted of frequency counts and percentages or means and standard deviations. Mean comparisons were done by means of ANOVA (ANalysis Of VAriation), with the groups as the independent factor. In the case of a significant Kolmogorov-Smirnov test for normal data, a logarithmic transformation was used; otherwise, a non-parametric Mann-Withney test was performed. Homogeneity of variance was assessed with the Bartlett test. Welch-adjusted ANOVA was carried out if variances were unequal. Pairwise comparison of the mean values between groups’ modalities were further investigated with the Ryan-Einot-Gabriel-Welsch multiple-range test when the homogeneity of variance was verified; otherwise, the Tuckey post-hoc test was used.
Binary or ordinal factors were first analyzed with a Chi-square test for comparisons between groups. Cochran-Mantel-Haenszel stratified analysis was performed in order to evaluate influences of visual disturbances and vertigo, differentiating between different headache groups, in terms of relative risks and 95% confidence intervals. Adjusted estimates were obtained using a logistics model or a proportional odds-ratio model, controlling for the type of headache.
A p value of <.05 was considered statistically significant. All tests were two-tailed. Statistical analyses were carried out with the statistical package SAS, version 9.3.1 (SAS Institute, Cary, NC, USA).
Results
A total of 2117 questionnaires from headache sufferers were returned (728 from the population-based prevalence study on headaches, the remainder from the volunteers recruited in hospitals, pharmacies and surgeries). A sample of 1909 of non-chronic headache sufferers (<15 headache days per month according to IHS criteria) was used for this analysis, as in chronic headaches the question of a temporal relationship between episodes of headache and other symptoms, such as dizziness, cannot be established.
Of the respondents, 77% were women. Among the respondents, 56.9% of males and 71.7% of females fulfilled the criteria for the diagnosis of migraine according to the Migraine ID (18).
No significant differences were found between the two recruitment groups in terms of age. In the volunteer population, women, chronic and high-frequency headache sufferers as well as migraine sufferers were more frequent than in the headache population–based group.
Among accompanying symptoms of headache episodes, visual symptoms (52.4%) were slightly more prevalent than dizziness (51.1%); the prevalence of dizziness did not differ according to type of recruitment in stratified analysis.
Prevalence of migraine- and headache-associated dizziness

The relative risk (RR) for a male migraine sufferer compared to that of a non-migrainous headache sufferer to have headache-related dizziness was 1.51 (95% confidence interval [CI]: 1.31–1.75); in the female population, RR = 1.63 (95% CI: 1.47–1.82). Dizziness was significantly linked to migraine in both genders after controlling for the recruitment method.
Regarding the two sensory symptoms, 33.5% had both dizziness and visual symptoms, and 30.7% had neither, possibly representing distinct populations. Visual symptoms were also significantly linked to migraine (RR = 1.77; CI: 1.62–1.92).
The link between migraine and dizziness remained significant after adjusting for visual symptoms (p < .0001 in Cochran-Mantel-Haenszel statistics).
The frequency of dizziness was similar across age groups.
The temporal association of dizziness and visual symptoms with the headache episodes was similar, mostly occurring during the headache episodes. A minority had the symptoms only before their headache (dizziness 5%, visual 7.5%).
The presence of dizziness with headaches was associated with higher disability as measured by MIDAS (stratified analysis χ2 test p < .001), independently from gender and headache type (Figure 1).
Effect of dizziness assessed by the Migraine Disability Assessment questionnaire (MIDAS). Presence of dizziness makes disability significantly worse (χ2 test p < .001), independently of gender and headache type (stratified analysis).
According to the PHQ9, which assesses depression, dizziness is associated with more severe depression (stratified analysis χ2 test p < .001), independently from gender and headache type (Figure 2).
PHQ9 (depression) scores. Presence of dizziness makes depression significantly worse (χ2 test p < .001), independently of gender and headache type (stratified analysis).
WHODAS showed an association of dizziness with increased functional impairment, independently from headache type and gender (Cochran-Mantel-Haenszel statistics p < .001) (Figure 3).
Effect of headache accompanying dizziness on the World Health Organization’s disease-independent Disability Assessment Schedule (WHODAS).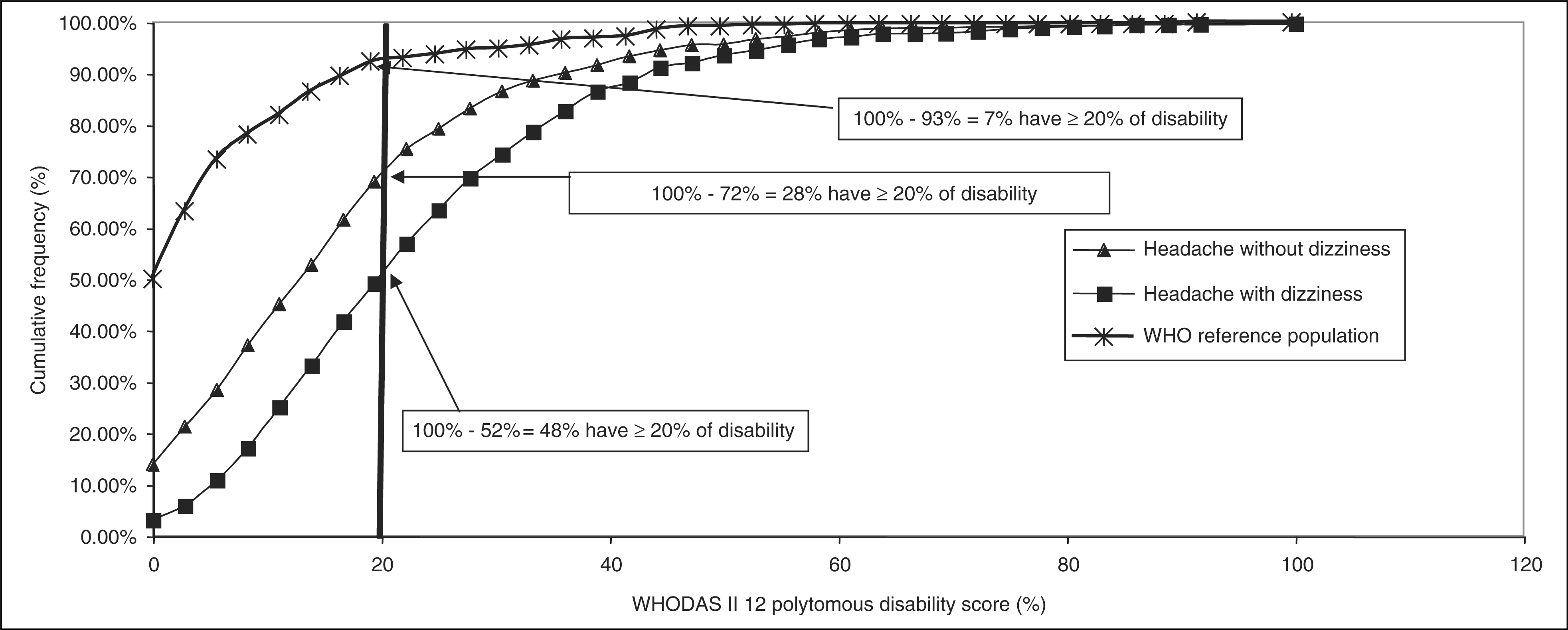
Dizziness and migraine were associated with a higher frequency of episodic headaches. In a linear model, no interaction between frequency, headache type and presence of dizziness was found, meaning that all factors have an independent negative effect on WHODAS, MIDAS and PHQ9.
A similar analysis on the impact of visual symptoms showed that they were also significantly linked to migraine and had significant negative impact on MIDAS, WHODAS and PHQ9 scores, and the effect was still present after controlling for migraine and dizziness.
Headache sufferers with dizziness more frequently used rescue medications, independently of headache type, and had tried a greater number of preventive medications. They more frequently indicated that they did not have their headache ‘under control’, and a higher proportion had had brain imaging (computed tomography [CT] scans or magnetic resonance imaging [MRI]; 45.1% vs. 29.8%).
Discussion
The data presented here are derived from a study conducted in Luxembourg designed to assess the impact on social and professional functioning in adult headache sufferers, focusing on the contribution of accompanying symptoms, particularly dizziness. Two types of recruitment methods were used. A first group was recruited from a general population–based prevalence study on headaches, and a second group consisted of headache sufferers responding to an appeal in hospitals, pharmacies and surgeries to take part in the impact study. Although the second group had more women and a higher proportion of frequent headaches and migraine, the prevalence of dizziness was not statistically different between the two groups; this aspect can therefore be considered representative of an unselected headache population.
A sample of 1909 non-chronic headache sufferers (<15 days per month according to IHS criteria) was used for this analysis, as in chronic headaches the question of a temporal relationship between episodes of headache and other symptoms, such as dizziness, cannot be established.
Although studies have shown that dizziness is, with a proportion of 23%–29.5%, a highly prevalent symptom in the general population (4,5,19), the proportion of participants experiencing dizziness associated with their headache episodes is higher than expected based on those studies. The analysis revealed that dizziness in our sample is a common accompanying symptom of episodic headaches, affecting 51.1% of participants, which is in the same order of magnitude as visual symptoms. Dizziness was significantly linked to migraine after controlling for gender, headache frequency, presence of visual symptoms and type of recruitment.
The strong association of dizziness with migraine found in this study is in line with previous studies (9)
Dizziness can be caused by several pathophysiological mechanisms, including dysfunction of the vestibular system, but also by cardiovascular problems, intoxication, side effects of drugs, hyperventilation, anxiety, depression and other mechanisms (6).
The high proportion of dizziness in temporal association with headache episodes is unlikely to be explained solely by coincidence of independent vestibular and non-vestibular disorders or side effects of acute headache medication.
Sensory hypersensitivity is common during migraine attacks, and the presence of photo- and phonophobia is part of the diagnostic criteria for migraine according to the ICHD-II (10). ‘Dizziness’, at least in some patients, could be due to a similar disturbance in another sensory modality (vestibular sensations), with a hypersensitivity to movement (‘kinephobia’). Another proportion of dizziness is likely to correspond to ‘vestibular migraine’ (11,20–22), but the high prevalence in non-migraine headaches suggests the presence of a variety of factors. From the present data, it is not possible to differentiate among various possible contributing factors to the dizziness.
This study shows that dizziness associated with headaches has a negative impact on functioning in professional and social life and is associated with low mood. The impact of dizziness remains significant after controlling for headache type and frequency, gender and presence of visual symptoms, suggesting that it is an independent factor for negative impact, and should therefore be further studied. The impact of dizziness is also reflected by a greater number of brain scans done and prophylactic medications tried and by the more frequently perceived ‘lack of control’ of the headaches.
Our results are compatible with previously published data on the impact of vestibular migraine on quality of life and depression measures in a population of migraineurs (23).
Migraine is known to be comorbid with anxiety and depression (24–26) and vertigo with anxiety and panic disorders (27–29). As vertigo is associated with migraine (9), it is possible that vestibular symptoms are part of the link between migraine and its psychiatric comorbidity, in particular, anxiety, as proposed by others (30).
Vestibular symptoms have so far not been acknowledged as being part of the spectrum of common migrainous symptoms, as opposed to symptoms involving other sensory modalities: vision (typical aura, photophobia), hearing (phonophobia), smell (osmophobia) and touch (allodynia). One reason for the paucity of data on dizziness and vertigo associated with headaches could be the lack of internationally accepted definitions for vestibular sensations (7). Only recently, tools for studies have been developed to better distinguish vestibular from non-vestibular dizziness (4,31).
Our study is limited by the fact that the questionnaire did not quantify the intensity of dizziness and its functional impact. Therefore, correlations to the severity and duration of headache could not be calculated.
Our data suggest that non-specific disturbances of balance might be commonly associated with headache episodes and may in fact be a regular accompanying symptom of headaches, comparable in magnitude to visual disturbances and having a negative functional impact. More population-based research is needed to confirm our data, and also to evaluate the different underlying pathophysiological mechanisms.