
Abstract
Australian teachers and school employees report high levels of stress-related mental health problems. Previous theory and research show that workplace training in strategies to manage stress can improve organisational productivity as well as employee wellbeing. Theory suggests that self-compassion strategies may produce better outcomes, than standard cognitive behavioural training interventions, due to activation of self-soothing. This pilot randomised controlled trial evaluated whether inclusion of a brief compassion-focussed therapy (CFT) training workshop was more effective in reducing stress-related mental health problems of school employees, than the standard professional development (PD) workshop that incorporated cognitive behavioural therapy and mindfulness strategies. School employees (103) were recruited and randomly allocated to either the standard PD alone or to also participate in a brief CFT workshop. There were very large reductions in burnout and clinically significant improvements in mental health problems under both conditions. The results provide preliminary evidence that CFT-enhanced training improves secondary traumatic stress and compassion satisfaction; further research needs to be conducted with a larger sample. These results may also be relevant to other occupations with a high emotional load.
Keywords
1. Introduction
Mental health claims due to psychosocial risks at work are a growing area of concern. Safe Work Australia (2023) reported a substantial increase in mental health claims over the last decade with both the median time lost from work, and compensation payouts, around four times that of other injuries. Australian teachers are particularly at risk. In a comparison of injuries over industry type, education and training had the highest overload from job demands and the highest emotional demands, with burnout and psychological strain higher among educational workers than in other industries (Jimmieson et al., 2016). In addition to having a heavy workload, teachers, principals and other school employees often deal with a heavy burden of potentially traumatic and emotionally challenging work, including managing students with behavioural and emotional problems, dealing with angry parents and supporting grief responses to stressful events of children and families (Maxwell and Riley, 2017; Rajendran et al., 2020). Human Resources Managers supporting Australian schools regularly identify employees who are at-risk for taking stress-related leave (Jimmieson et al., 2016).
This high level of teacher stress is not unique to Australia; teacher stress is a global issue that predicts turnover intent (Ryan et al., 2017). Work stress predicts increased risk of mental illnesses including depression and anxiety (Milner et al., 2018), the leading causes of sick leave and long-term work disability in most developed countries (Joyce et al., 2016). Leave from stress-related mental health problems such as anxiety, depression and trauma places a heavy burden on employers, with the cost of untreated mental health problems in Australia alone estimated at $10.9 billion annually (Beyond Blue, 2015).
Over the last 30 years, many organisations have implemented interventions aimed at reducing work-related employee stress and stress-related mental illness. There are three broad types of interventions: primary, secondary and tertiary. Primary prevention programmes aim to remove organisational sources of stress, including known psychosocial stressors such as workload and low job control (Murphy and Sauter, 2003). Secondary and tertiary interventions focus on individuals impacted by work stress. Secondary programmes, which are the focus of this study, attempt to reduce the severity of stress symptoms before they lead to serious health and mental health problems (Murphy and Sauter, 2003), whereas tertiary interventions target those who have already developed mental illness (Joyce et al., 2016). Several meta-analyses have examined the effectiveness of these interventions for individuals randomly allocated to an intervention condition, compared to those who do not receive treatment, or are on a waitlist control. In general, these meta-analyses have reported medium effect sizes for the impact of primary and secondary workplace interventions on stress (Richardson and Rothstein, 2008). Larger effect sizes have been reported for cognitive behavioural interventions, that aim to modify thoughts and behaviours contributing to stress; however, effect sizes were smaller when these interventions also included other components like time management strategies (Bhui et al., 2012; Lau and Mak, 2017; Richardson and Rothstein, 2008). Mindfulness is attentiveness to the present moment with curiosity, openness and acceptance (Bishop et al., 2004); interventions using mindfulness training also reported a medium effect size for stress (Bartlett et al., 2019). In all meta-analyses, there was substantial diversity in length of programmes and sessions, ranging from a single session to many hours over weeks and months. However, time investment was found not to moderate effectiveness (Richardson and Rothstein, 2008). Although research incorporating organisational outcomes (such as absenteeism and work quality) is limited, evidence suggests that interventions that enhance emotional coping skills of employees can improve service delivery as well as employee wellbeing (e.g. Clarke and Hill, 2012). So, in general, research suggests employee stress reduction programmes are of benefit to organisations as well as employees.
Building on this strong foundation, recent research suggests that the inclusion of compassion-focussed approaches may help improve the impact of cognitive behavioural and mindfulness-based interventions (Jazaieri et al., 2014; Kirby and Gilbert, 2017). Compassion can be defined as, ‘the sensitivity to suffering in self and others, with a commitment to try and alleviate and prevent it’ (Gilbert, 2014: p. 19). Previous research has found that compassion is helpful for improving emotion regulation (Finlay-Jones et al., 2015), improving motivation (Breines and Chen, 2012) and improving feelings of connectedness (Neff, 2009). A meta-analysis of compassion-focussed interventions, including 21 randomised controlled studies involving 1200 adults, found significant moderate effects for reducing depression, anxiety, stress and significantly improved wellbeing and compassion compared to waitlist controls (Kirby et al., 2017b). However, these results were from clinical and community populations, rather than individuals recruited in workplace settings.
Meta-analytic research has also found that self-compassion in particular is beneficial for mental health and wellbeing (MacBeth and Gumley, 2012). According to Gilbert (2014), when someone is mindful of the present moment, compassion can inform actions to help alleviate suffering of self and/or others. Relevant to helping employees manage their own stress, there is substantial evidence that self-compassion (acting as one’s own source of comfort) contributes uniquely to positive functioning in times of stress (Dodson and Heng, 2020). Self-compassion may also help employees improve the support they give to customers: for instance, a qualitative study found that teachers who were high in self-compassion reported more capacity to provide emotional support to challenging students (Jennings, 2015). Research has found that self-compassion helps reduce the adverse effect of work-family conflict on psychological wellbeing (Rafique et al., 2018). In addition, Babenko et al. (2019) found that self-compassion was associated with increased job engagement and decreased emotional exhaustion for workers. The aim of this project is to evaluate whether inclusion of a brief compassion-focussed therapy (CFT) training workshop is more effective in reducing stress and related mental health problems of school employees, compared with a brief standard professional development workshop incorporating cognitive behavioural and mindfulness strategies.
Several systematic reviews have examined the impact of self-compassion-focussed workplace training interventions on employee outcomes for wellbeing, stress and stress-related mental health problems but noted methodological limitations of current research. Dodson and Heng (2020) found that self-compassion training led to decreased stress and burnout, based on a small number of interventions studies, most of which lacked a control group. Similarly, Kotera and Van Gordon (2021) concluded that self-compassion training can improve self-compassion and other work-related outcomes of employees including stress, burnout, wellbeing and resilience but noted methodological limitations of existing studies. Interventions studied ranged from 1 to 60 hours. Although one pre-post study reported improvements in self-compassion-based on an online session of only 1 hour (Rao and Kemper, 2017), Kotero and Van Gordon noted there was more robust evidence for longer interventions, and that overall, more randomised controlled trials (RCTs) involving active control groups were needed. The current study addresses this call.
We selected CFT (Matos et al., 2022), a brief compassion-based intervention specifically aimed at helping individuals with self-criticism and emotional distress through development of self-compassion (Gilbert, 2014). In CFT, there is a central focus placed on the motives of competition versus compassion. A competitive focus leads to social comparisons that increase the likelihood of submissive or aggressive behaviours, which is found to be relevant in understanding depression, anxiety and other clinical disorders (Wetherall et al., 2019). Alternatively, compassion, which is focussed on alleviating distress, can facilitate self-reassurance and encouragement, which may protect against depression and anxiety (Petrocchi et al., 2019). The aim of CFT is to shift people from competitiveness to a compassionate focus, through self-reassurance, validation and encouragement.
A defining feature of CFT is its model of affect regulation. The model, depicted in Figure 1, is referred to as the ‘three affect regulation systems of emotion’ and is informed by affective neuroscience research into the evolutionary functions of emotion (Depue and Morrone-Strupinsky, 2005; LeDoux, 1998; Panksepp, 1998). These three emotion regulation systems interact and include: (a) the threat/self-protect system, (b) the drive/reward system and (c) the affiliative/soothing system. The threat system detects and responds to physical and social dangers to enable protection. It is responsible for the physiological fight/flight response (sympathetic system) when faced with a threat so is the most dominant emotion regulation system, when activated (Gilbert, 2014). An example of a potential threat to a classroom teacher would be disruptive behaviour of students. The drive system is concerned with seeking and obtaining resources and achieving desired goals (Gilbert, 2014), which can activate positive emotions of excitement, pleasure and happiness. An example of a drive for a classroom teacher would be achieving student understanding of the maths lesson. The function of the third soothing/affiliative system is to enable recovery, rest and digestion, associated with feelings of calm, contentment and peace. According to Gilbert’s model, the soothing system is linked to the parasympathetic nervous system which slows down the autonomic nervous system, that is associated with feelings of stress. For an individual teacher, this may mean implementing self-soothing when disruptive behaviours of students threaten to derail the maths lesson.
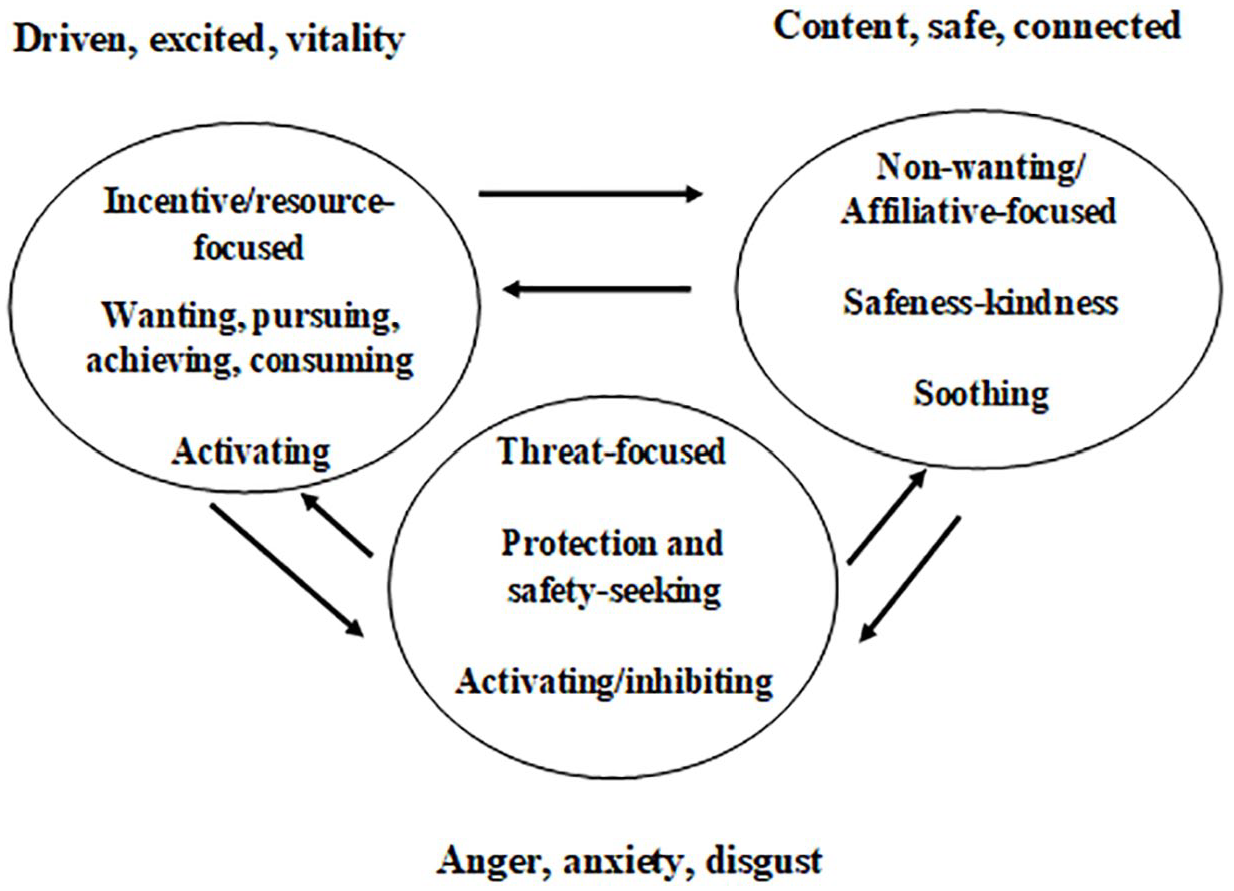
The interaction between the three major emotion-regulation systems. From Gilbert, The Compassionate Mind (2009), reprinted with permission from Constable & Robinson Ltd.
How these systems operate is contextual. For instance, in a crisis, such as dealing with high-level aggression, it may be more important to have a dominant threat-drive system as opposed to a dominant calm and peaceful orientation; this may help gain the attention of the class so as to follow a direction, such as the lock-down procedure. The theory postulates that, if one is compassionately motivated, there is greater balance between these systems. Conversely, if one is competitively motivated, there is an overreliance on the threat-drive systems, which is theorised to be a vulnerability factor for stress and mental health difficulties (Gilbert, 2014). These systems can be triggered by external factors (e.g. immediate physical threat) or internal factors (e.g. judgements we make). A balance of these three affect regulation systems is required to obtain successful emotion regulation. The aim of CFT therefore is to cultivate the compassionate motive to bring about a greater balance of these three systems.
To date, systematic reviews examining effectiveness of treating stress-related mental illness have concluded that CFT shows promise as an intervention for depression (Craig et al., 2020; Leaviss and Uttley, 2015). Recent research has begun to examine the effectiveness of CFT in reducing employee stress in workplaces, including schools. A pilot study in the United Kingdom found that CFT was reported as helpful for reducing self-criticism and increasing self-compassion of teachers and support employees (Maratos et al., 2019); however, this study did not use an RCT design. The intervention itself was time-consuming, lasting six sessions. Lighter touch 2-hour CFT seminars have been found to be effective at reducing self-criticism and improving self-compassion in clinical and community settings. For example, an RCT of a brief 2-hour module of CFT with a general community sample of 93 participants found that, compared with a wait-list control group, participants in the intervention group had significantly reduced self-criticism, depressive symptoms and improved wellbeing (Matos et al., 2017). The current study examines whether this brief CFT intervention enhances mental health outcomes of school employees, compared to the standard stress management workshop alone.
1.1. Study aims
This study aimed to evaluate whether the addition of a 2-hour CFT workshop was more effective than a standard professional development programme alone in reducing stress and stress-related mental health problems of school employees in a region on the East coast of Australia. We predicted that, compared to the active control group that received only the standard programme, that the CFT group would have greater reductions in stress, anxiety, depressive symptoms, traumatic stress and burnout, and greater improvements in compassion satisfaction, self-compassion and resilience.
2. Method
2.1. Procedure
The project used an RCT design. Interventions were delivered in-person. Eligible participants were employees of the state Department of Education, (either in a school or in a regional role supporting schools), who enrolled in one of two standard professional development workshops aimed at reducing stress and improving wellbeing: ‘Managing Stress, Anxiety and Depression’ for all schools and regional office staff and ‘Looking after Yourselves in the Frontline’ targeting at school administrative staff. These one-off workshops were offered in-person from 8:30 to 11:30 a.m. including a 20-minute morning tea break. Employees from schools across the region travelled to a central school to attend the workshop in the school library in groups of approximately 30 employees.
When employees enrolled in either of the above workshops they were asked if they would like information about participation in the trial of CFT. Employees who expressed interest were sent information and directed to an online site where they could complete consent forms and the initial online assessment. Employees who completed the initial online assessment were randomly allocated to either standard professional development (Standard PD) or standard PD plus CFT (CFT Enhanced PD) conditions. Employees who were allocated to CFT Enhanced PD were offered CFT in-person from 1:00 to 3:00 on the same day as their participation in Standard PD, following a short lunch break. Employees from both conditions were asked to complete a second online assessment 2 weeks later. In practice the mean (SD) time that the second assessment was completed was 55.2 (27.1) days after the initial assessment. Employees who had been allocated to the Standard PD condition were invited to a subsequent CFT workshop (from 1:00 to 3:00) on any date that suited them after they had completed the second assessment.
2.2. Control condition: Standard PD
Both Standard PD courses offered to employees in the region included cognitive behavioural and mindfulness strategies aimed at managing stress and stress-related mental health problems. Staff were also provided information about strategies to enhance protective factors against stress and associated mental health problems, such as engaging in regular exercise and maintaining social connections. Both courses also included tips on managing workload, as this is a frequent stressor raised by school employees. The ‘Looking after Yourselves in the Frontline’ workshop included a short (30-minute) focus on managing stressful situations with emotional customers (e.g. angry parents). The ‘Managing Stress, Anxiety and Depression’ workshop spent more time on risk and protective factors and strategies for managing anxiety and depression. Both workshops prompted employees to develop a personal wellbeing plan which included proactive strategies to maintain and improve their general ongoing resilience and wellbeing, and strategies to manage emotions in the moment. In summary, both interventions would have been categorised as having multiple components (Lau and Mak, 2017; Richardson and Rothstein, 2008).
2.3. CFT-enhanced intervention condition: Standard PD plus CFT
The CFT seminar was a single 2-hour session designed to cultivate compassion, especially self-compassion. The intervention included psychoeducation about compassion according to the CFT approach (Gilbert, 2014; Matos et al., 2017). The CFT seminar included seven specific practices that were completed within the seminar: 1) body posture, 2) friendly voice tone and facial expression, 3) soothing rhythm breathing, 4) mindfulness, 5) cultivating the compassionate self, 6) compassion for others and 7) self-compassion. For instance, the exercise on compassion for self, asked participants to generate compassionate wishes towards themselves, for example, ‘may I be free from suffering’, and direct this wish to oneself using a warm and friendly inner voice tone. Participants were provided with a workbook that described the exercises, and were sent an email with a weblink to the recorded guided audio tracks that were used in the CFT seminar so they could continue to practice the exercises. All tracks used in the intervention are available on the Open Science Framework: https://osf.io/vpuhs/.
2.4. Participants
Our initial aim was to complete a full RCT; towards this, we had aimed to recruit 150 participants. However, our data collection was interrupted by COVID-19, which resulted in the redesign of the Standard PD course so it could be delivered through an online platform; thus, collection of data for the current study ceased. In total, 103 employees (94 female) had been recruited before this interruption, 83 of whom were enrolled in one of 11 ‘Managing Stress, Anxiety and Depression’ workshops offered between Term 3 2018 and Term 1 2020, and 17 of whom were enrolled in one of three ‘Looking after Yourselves in the Frontline’ workshop in this time period (and three employees who could not be identified from workshop records as they used a non-departmental email to sign into Redcap). The 103 employees were randomised to either the Standard PD (n = 50) or the CFT Enhanced PD (n = 53). Of these, 76 (73.7%) employees commenced the post-assessment, and 73 (70.9%) employees continued this post-assessment to completion. A simulation study found that, for continuous variables, a sample size of 70 is usually sufficient for pilot RCTs to estimate parameters of a full RCT (Teare et al., 2014). Hence, the sample from the current study was considered sufficient to calculate effect sizes and the parameters required for a full RCT to test for statistically significant differences between the two intervention conditions.
2.5. Measures
The Professional Quality of Life Scale (ProQOL; Stamm, 2005) is the most commonly used measure of negative and positive affect associated with helping others who experience suffering and trauma. There are 30 items which respondents rate on a 5-point scale from ‘1’ (never) to ‘5’ (very often). There are three subscales including compassion satisfaction (e.g. ‘I get satisfaction from being able to help people’), burnout (e.g. ‘I feel worn out because of my work as a helper’) and secondary traumatic stress (or compassion fatigue, e.g. ‘As a result of my helping I have intrusive, frightening thoughts’). The internal reliability of all three subscales was acceptable with Cronbach’s alphas for compassion satisfaction (.87, .91), burnout (.77, .79) and secondary traumatic stress (.80, .89) at the pre-assessment and post-assessment, respectively.
The Depression Anxiety Stress Scale (DASS-21) is a well-established 21-item measure of depression, anxiety and stress. Items ask respondents to indicate the frequency of experiences on a four-point scale from ‘0’ (not at all) to ‘3’ (most of the time). The DASS-21 subscales have Cronbach’s alphas of .94 for depression, .87 for anxiety and .91 for stress (Antony et al., 1998; Lovibond and Lovibond and Lovibond, 1995). Internal reliability was acceptable in the current study with Cronbach’s alphas for depression (.94, .96), anxiety (.85, .90) and stress (.92, .93) at pre- and post-assessments, respectively.
The Brief Resilience Scale is a six-item scale of individual resilience in the face of adversity. Respondents rate their level of agreement to statements (e.g. ‘I tend to bounce back quickly after hard time’) on a five-point scale from ‘strongly disagree’ to ‘strongly agree’. Internal reliability was acceptable with a Cronbach’s alpha of .92 for both timepoints.
The Fears of Compassion Scale – Self (FCS; Gilbert et al., 2011) assesses fears of compassion towards the self on a five-point Likert-type scale from ‘0’ (don’t agree at all) to ‘4’ (completely agree). It has 15-items with an example item being ‘I feel that I don’t deserve to be kind and forgiving to myself’. Scores are summed with higher scores indicating higher fears of compassion. Fears of self-compassion are negatively associated with positive self-compassion (Gilbert et al., 2011). Internal reliability was good with Cronbach’s alphas of .95 for pre- and post-assessments.
2.6. Analyses
Basic data screening and a missing data analysis were conducted through Statistical Package for Social Sciences (SPSS). This revealed that 33.63% of the total values were missing, including data missing due to attrition (i.e. 30 participants). As Little’s test showed that data were missing completely at random, χ2 (2840) = 1615.49, p > .999, we conducted data imputation through Expectation Maximisation (SPSS). Expectation Maximisation is an example of a ‘principled’ method of imputing missing values in that it uses observed data and statistical assumptions to estimate the population parameters (Dong and Peng, 2013). Simulation studies have found that the pattern of missingness is more important than the proportion of missingness per se (Madley-Dowd et al., 2019). For data missing ‘completely at random’ (or even ‘at random’), imputing data produces less bias in treatment effect and higher power than either the case-complete approach (list-wise or case-wise deletion) or last-observation carried forward (Baron et al., 2008; Dong and Peng, 2013; Madley-Dowd et al., 2019). Furthermore, Expectation Maximisation performs as well, if not better, than other methods of imputation for data sets with 20–60% of data missing at random or completely at random (Dong and Peng, 2013).
We analysed intervention effects through a series of repeated measures mixed design Analyses of Variance (ANOVAs) with time as the within-subject variable and experimental condition as the between-subjects variable, again through SPSS, which also provides information about effect size. As recommended by Jacobson and Truax (1991), we tested the clinical meaningfulness of change for measures with established norms; this included the sub-scales from the DASS and ProQOL scales. Clinical cut-offs for the DASS were scores outside the normal range (i.e. mild upwards) for each sub-scale (Lovibond and Lovibond and Lovibond, 1995). Clinical cut-offs for the ProQOL scales were designated as more than 1 SD beyond the mean scores, using statistical information provided in the manual (Stamm, 2005). We examined changes over time in the proportion of clinically elevated cases within and between conditions using the McNemar test through SPSS (Lund Research, 2018). We compared differences between conditions in the proportion of cases that changed from clinically elevated to the normal range between pre- and post-assessments, by chi-square tests through SPSS, using exact 2-sided tests.
Sample sizes required to test differences between conditions in a full RCT were calculated through G-Power, using an alpha level of .05 and a power level of .8, and imputing parameters from ANOVAs (partial eta squared and correlations between repeated measures of each variable).
3. Results
3.1. Preliminary analyses
We checked the effectiveness of randomisation by comparing the two groups on all pre-assessment and demographic variables using between-subjects ANOVAs and chi-square for categorical variables. There were no differences between conditions on demographics of age or gender. There were no differences between groups on the number of days between the two assessments (F (1, 74) = .037, p = .849). There were no differences between groups on pre-assessment measures of compassion satisfaction (F (1, 101) = .176, p = .676), burnout (F (1, 101) = .498, p = .482), secondary traumatic stress (F (1, 101) = 1.07, p = .303) or fears of compassion (F (1, 101) = .471, p = .494). However, there were difference between groups in pre-assessment scores of depression (F (1, 101) = 5.07, p = .027), anxiety (F (1, 101) = 5.41, p = .022) and stress (F (1, 74) = 7.37, p = .008) with higher scores in the control condition (Standard PD) than the enhanced intervention condition (CFT). Similarly, the Standard PD control condition had lower scores for Resilience at pre-assessment than the CFT intervention condition (F (1, 101) = 4.98, p = .028).
We tested differences at pre-assessment for those employees who completed the post-assessment compared to those who did not. There were no differences between these groups on demographics of age (F (1, 99) = .290, p = .592) or gender (F (1, 99) = .1.19, p = .279), or pre-assessment measures of burnout (F (1, 99) = .225, p = .636), secondary traumatic stress (F (1, 99) = .925, p = .338), depression (F (1, 99) = .243, p = .623), anxiety (F (1, 101) = .129, p = .720) and stress (F (1, 99) = 1.31, p = .256. However, there were marginally significant differences between the groups for Compassion Satisfaction (F (1, 99) = 3.75, p = .056) and Fears of Compassion (F (1, 99) = 3.79, p = .055) with dropouts having both marginally higher Compassion Satisfaction and marginally higher Fears of Compassion at pre-assessment.
3.2. Comparison of effects of interventions
Table 1 reports means and SDs for each group at each timepoint, and comparisons over time in each condition, across the whole sample and comparisons between conditions over time. There was a significant reduction in Burnout over time across both conditions (p < .001), consistent with a very large effect size; this is graphed in Figure 2. There were also significant reductions in depression (p = .035) and secondary traumatic stress (p = .027).
Effects of interventions on staff mental health.

STSS = secondary traumatic stress symptoms.
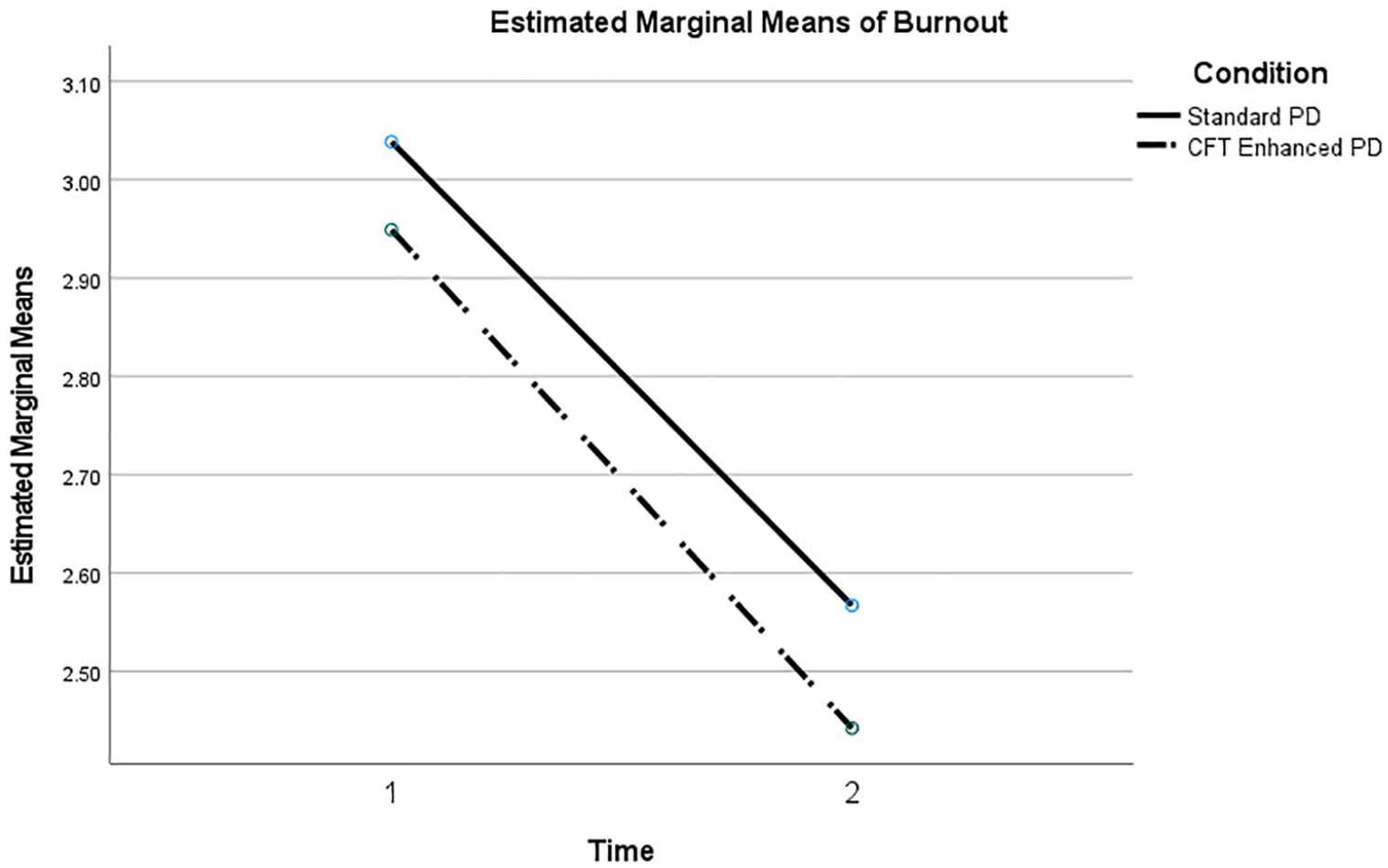
Change in burnout across conditions over time.
In addition to the large reduction in burnout (p < .001), the Standard PD alone was associated with a marginally significant reduction in depression (p = .054) and marginally significant increase in Resilience (p = .072). Apart from the large reduction in burnout (p < .001), the CFT Enhanced PD was associated with a significant reduction in secondary traumatic stress (p = .027) and marginally significant increase in compassion satisfaction (p = .067), but the improvements in depression (p = .281) and resilience (p = .799) were not significant. Figures 3 and 4 graph the interaction between the conditions over time for secondary traumatic stress and compassion satisfaction, respectively. The analyses of Time X Condition in Table 1 show a non-significant trend towards greater improvement in compassion satisfaction (p = .099) for the CFT Enhanced PD. No other interactions between condition and time were significant with the current sample size.
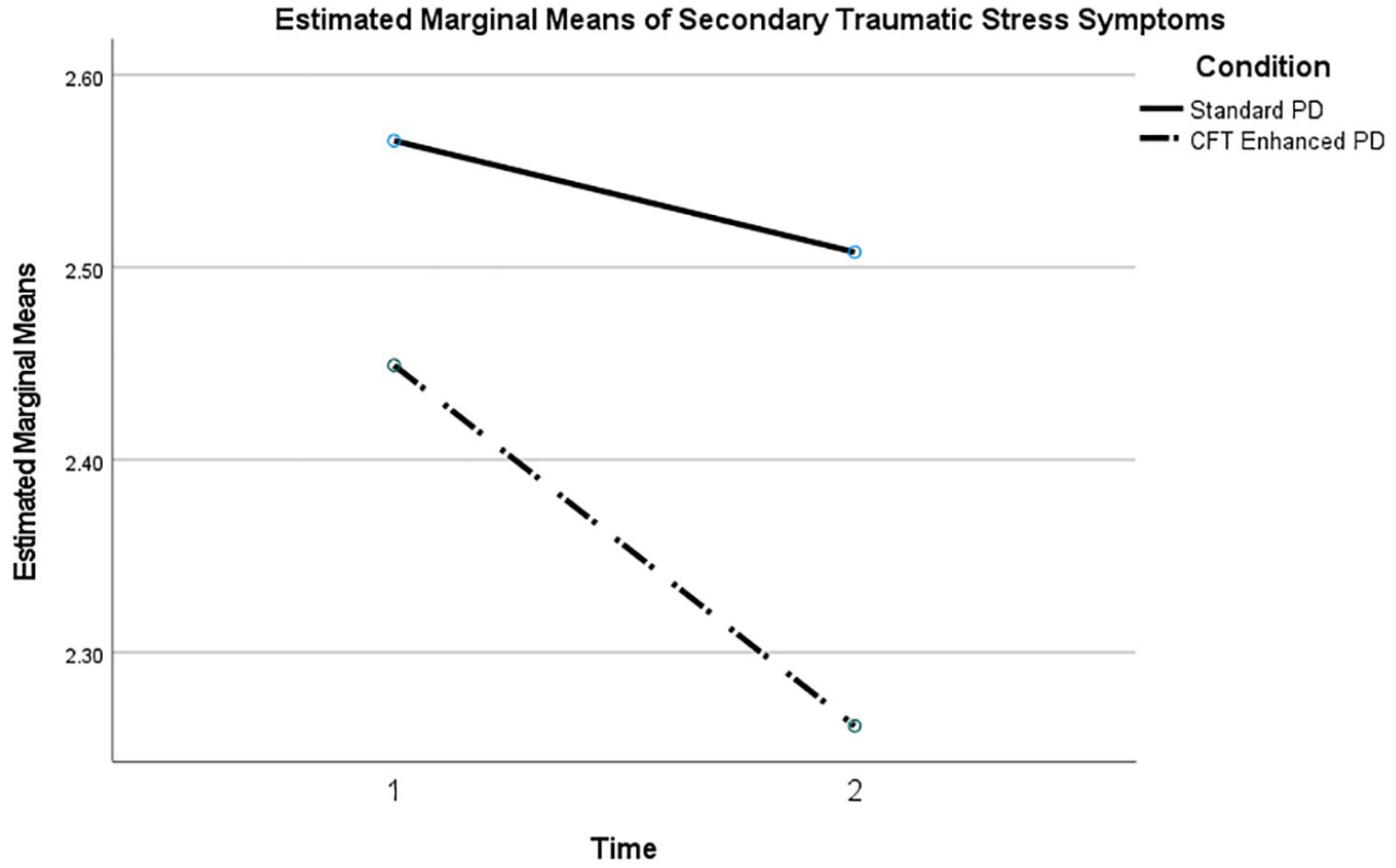
Change in secondary traumatic stress across conditions over time.
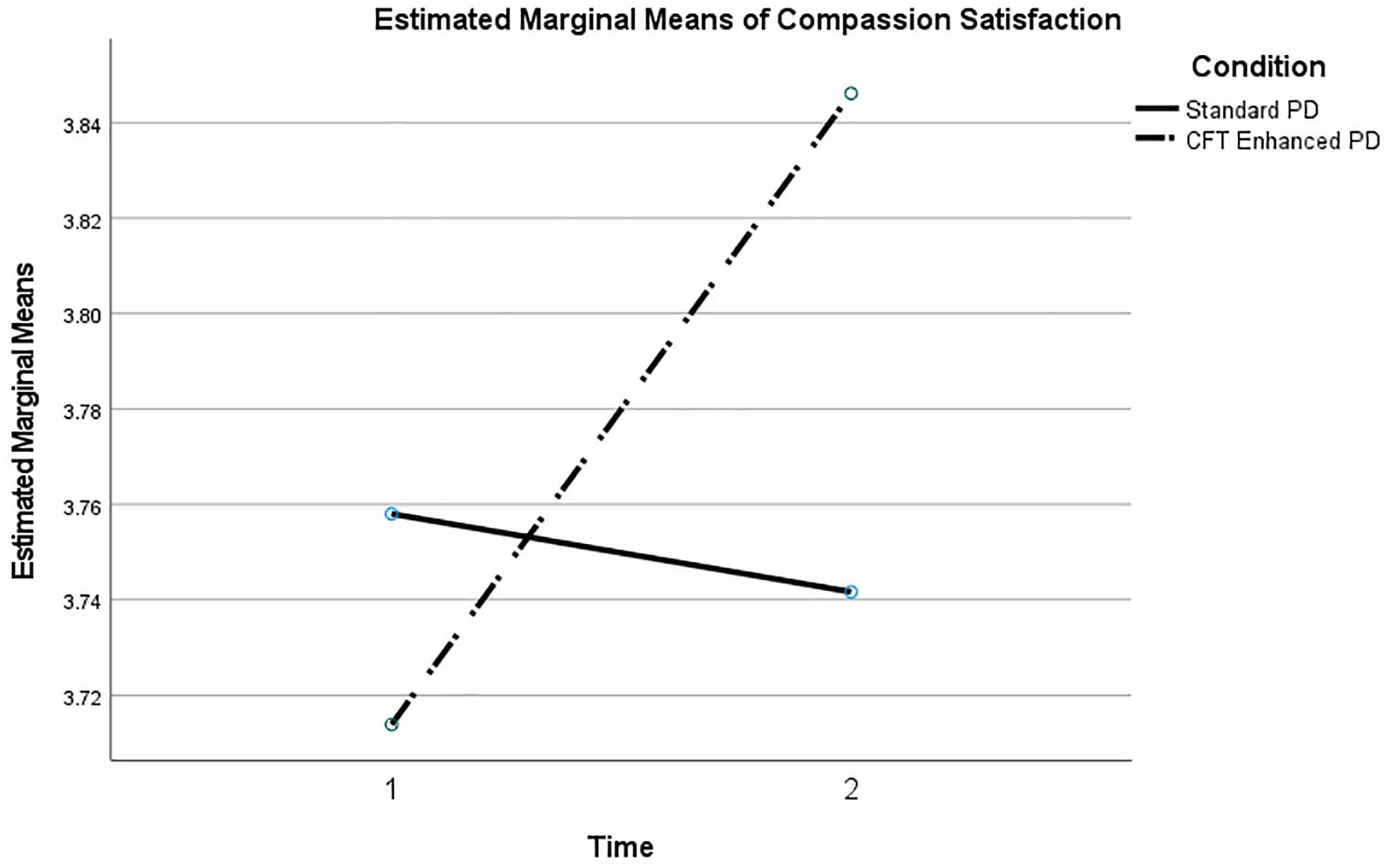
Change in compassion satisfaction across conditions over time.
3.3. Test of clinical significance of change
Table 2 reports on the clinical significance of change through comparison of subscales to established norms. The proportion of cases in the clinical range was high on many measures, notably for secondary traumatic stress (with 88.3% of the total sample in the clinical range at pre-assessment) and Burnout (with 62.1% of the total sample in the clinical range at pre-assessment). This suggests that many employees recruited to the trial were experiencing mental health problems. For the Standard PD group, a significant proportion of cases had moved out of the clinically evaluated range at post-assessment for burnout (p = .001), stress (p = .004) and depression (p = .011). For the CFT Enhanced Group, a significant proportion of cases had moved out of the clinically evaluated range for burnout (p = .001), anxiety (p = .020) and secondary traumatic stress (p = .035); there was a trend towards significance for cases moving out of the clinical range for depression (p = .073) and stress (p = .105). There were no significant differences between the two conditions for the proportion of cases moving out of the clinical range for any of the variables, although there was a non-significant trend (p = .096) for more cases moving out of the clinical range for stress for the Standard PD compared to CFT Enhanced PD.
Clinical significance of change.

STSS = secondary traumatic stress symptoms.
Exact 2-sided.
Includes cell counts of less than 1 so the result may not be reliable.
3.4. Calculation of sample sizes required for definitive RCT
Table 3 shows power analyses to determine sample sizes required for the power of .80 and .90. This shows that a sample size of 200–250 is likely to be sufficient to demonstrate significant improvements in compassion satisfaction, secondary traumatic stress, fears of compassion and resilience. On other variables like burnout and depression, the differences in effect sizes between conditions were very small, meaning that the sample size required to find a significant difference would be very large (n > 1500).
Power analysis to calculate required sample size for definitive RCT.

STSS = secondary traumatic stress symptoms.
4. Discussion
The aim of this study was to evaluate whether inclusion of a brief CFT training workshop improved the effectiveness of a Standard PD workshop in reducing stress-related mental health problems of school employees. Based on previous research, and theory about the soothing effect of self-compassion, we predicted that inclusion of a brief session on CFT, following Standard PD, would produce greater improvements in mental health outcomes, than the Standard PD alone. We initially planned to conduct a full RCT with an estimated sample size of 150 participants. However, our data collection was interrupted by COVID-19, at which stage 103 participants had been randomised to an intervention condition, of which 76 commenced (and 73 finished) a post-assessment. Although this sample was less than what we estimated would be required for a full RCT, it was sufficient for a pilot study to reliably estimate parameters required of a full RCT (Teare et al., 2014).
There were several main findings of note. First, the sample recruited included a high proportion of employees who scored in the clinical range for various mental health problems. Second, there was a substantial improvement in short-term mental health outcomes across both conditions, including a reduction in burnout, consistent with a very large effect size, and significant clinical improvements across both conditions. Third, the results of clinically significant improvements suggested that, if the trial had been properly powered by a larger sample size, the CFT Enhanced PD would have produced significantly better results than the Standard PD on some outcomes of secondary traumatic stress and anxiety. Fourth, however, contrary to predictions, results also suggested that the Standard PD alone produced better outcomes on variables including stress, depression and resilience. Fifth, results suggested that a sample size of 200–250 would provide sufficient power for a full RCT. Each of these main findings is discussed in turn below.
The first noteworthy finding of this study was that a high proportion of participating employees scored in the clinically elevated ranges for standardised measures of mental illness, most notably for secondary traumatic stress and burnout for which 88.3% and 62.1% of participants, respectively, scored in the clinically elevated range. High levels of burnout and increased risk of secondary traumatic stress have previously been documented in Australian teachers (García-Carmona et al., 2019; Ormiston et al., 2022). However, the most likely explanation for the high levels of stress in the current trial is that PD workshops encouraged self-selection of employees experiencing problems managing stress and stress-related mental health problems, meaning that those experiencing more stress were more likely to enrol in the study. If the trial had included all employees in one or more schools, we would expect that a lower proportion of employees’ scores would have fallen in the clinical range. Moreover, as some employees remained in the clinical range at post-assessment, perhaps longer interventions, over more sessions, would be helpful for those employees experiencing ongoing clinical levels of stress and stress-related mental health problems.
Another finding was the substantial short-term reductions in some mental health outcomes across both conditions over the period of monitoring. In particular there was a very large reduction in burnout. Burnout is emotional exhaustion resulting from excessive job demands and chronic stress (Rajendran et al., 2020). In addition to negatively impacting individual employees, it has serious impacts on the organisation, with burnout predicting turnover intent of teachers (Rajendran et al., 2020). Previous research shows that workplace cognitive behavioural and mindfulness interventions for teachers produce significant but small reductions in burnout, with smaller effect sizes for shorter interventions (Iancu et al., 2018). The Standard PD included components about workload management. Previous research has found that being overwhelmed by one’s workload was strongly linked to burnout (Hotchkiss and Lesher, 2018). Perhaps workload management is more important for preventing burnout than other stress-related conditions. However, these results must be interpreted with caution: the current study monitored short-term effects only and did not have a comparison condition for Standard PD. Although, the strong short-term reductions for burnout in the current trial are promising, future research should investigate whether these improvements persist. Ideally, the effectiveness of the Standard PD could be evaluated using an RCT design. However, it would be difficult, and ethically questionable, to withhold Standard PD from employees who request it. Perhaps, quasi-experimental designs could compare outcomes with matched employees who do not attend the Standard PD programme.
Although the sample study was underpowered to find significant differences between two active treatment conditions, there were some differences between conditions on tests of significance of clinical improvements. Unlike the Standard PD alone, the CFT Enhanced PD produced significant reductions in cases that were initially in the clinically elevated range for secondary traumatic stress and for anxiety. The primary aim of CFT is to de-shame the individual when it comes to experiencing distress because of external contextual stressors (e.g. disruptive student behaviour), by using its evolutionary-informed three-affect regulation model of emotion regulation (Gilbert, 2014). The threat system is typically triggered by external threats and linked to anxiety and traumatic stress. Learning how to apply compassion-based practices, to increase the soothing system, could have led to the significant reductions in traumatic stress and anxiety. The significant reduction in clinical change for anxiety of school employees is new; past research with school employees in Portugal and the UK reported anxiety scores within the normal range (Matos et al., 2022). The large proportion of individuals with elevated clinical symptoms in our sample could explain this difference. This study adds to a growing body of research suggesting that self-compassion training may improve work-related wellbeing, including with school-based employees (Maratos et al., 2019); it also addresses some of the methodological limitations of previous research by using a randomised design (Dodson and Heng, 2020; Kotera and Van Gordon, 2021).
Contrary to predictions, statistical trends suggested that Standard PD alone was more effective than when combined with CFT PD on some outcomes. Specifically, tests of the significance of clinical improvement showed that a significant proportion of cases in the Standard PD group moved out of the clinical range for stress and depression, but this was not the case for the CFT group. Also, although there were no statistically significant interactions between condition and improvement on any variable on General Mixed Model tests, Table 3 shows that the second greatest difference between conditions was in resilience, favouring Standard PD. These results are contrary to previous research that shows that CFT is helpful in reducing stress and depression compared with wait-list controls (Kirby et al., 2017b), and also to the theory described earlier. However, there are other plausible explanations for these results. First, as previously noted, randomisation resulted in some statistically significant differences between the two groups at pre-assessment, including for depression (p = .022), stress (p = .008) and resilience (p = .028), with the Standard PD having the poorer mental health score for all these variables. These differences are also apparent for the proportion of participants clinically elevated at pre-assessment in the Standard PD group (48%; 56%) compared with the CFT Enhanced Group (26.4%; 26.4%) for depression and stress, respectively. It may be that it was easier to reduce stress and depression and improve resilience for individuals who had very poor scores to begin with than to improve scores that were closer to the mean.
Another possible explanation for the apparently stronger results for the Standard PD than the CFT Enhanced condition on some measures may be in the way the PD was delivered. For the CFT Enhanced condition, the CFT PD was offered after lunch on the same day as the Standard PD. As a result, there may have been too much information presented in too short a timeframe, impacting the employees’ engagement, mastery of skills and capacity to implement strategies for both the Standard PD and CFT Enhanced, which may have limited the outcomes achieved. This may also explain why short wellbeing interventions have been found to have similar impacts to more intensive interventions (Richardson and Rothstein, 2008); perhaps the limiting factor is that employees only can implement a small number of strategies in a time period.
Also, contrary to predictions, there were reductions of similar size in burnout, stress and depression, across both conditions. Another recent RCT compared outcomes over 3 months for a compassion intervention (6 weeks X 2 hours) against an active control intervention (physical exercise); like the current study, stress and mental ill-health decreased in both groups similarly, but self-compassion only increased in the intervention group (Andersson et al., 2022). Perhaps, general wellbeing interventions are effective in reducing stress, depression and burnout and the self-soothing quality of self-compassion, encouraged by CFT, is more effective for traumatic stress.
We also propose that improvement across both conditions could be interpreted in terms of compassion-focussed theory. All employees self-selected for participation in the Standard PD and the trial; perhaps, we attracted employees who had noticed they were stressed and were taking action to alleviate it, that is, self-care. All participating employees required approval from their line managers to take time out during school hours to participate in the workshops. This approval may have been impactful, as it may have been interpreted as managers’ supporting the employees’ self-care, and may have ensured that employees in our sample had managers that supported self-care. Previous research suggests that employees may need to feel supported by others in order to be self-compassionate (Dodson and Heng, 2020). Future management research could investigate this hypothesis that perceived managerial support impacts effectiveness of stress management and self-care interventions for employees.
Following a reduced sample size, due to interruptions in face-to-face training through COVID-19, the main aim of this modified study was to calculate the sample size required for a definitive RCT testing whether including of brief CFT training enhances mental health outcomes of school employees beyond Standard PD. This study has determined that CFT is likely to produce significantly greater improvements than the Standard PD on outcomes of traumatic secondary stress, fears of compassion and compassion satisfaction with a sufficiently powered study, and that the sample size required to achieve this power would be between 200 and 250 participants.
The findings of this study have substantial practical implications for managers of school employees. First, this study provides further evidence that some Australian school staff are under a high level of stress and at risk of burnout and emotional exhaustion from vicarious trauma. It is essential that they be offered high-quality PD and access to evidence-based therapy. There was already substantial evidence that primary and secondary workplace stress management training interventions, particularly those that include cognitive behavioural and mindfulness strategies, reduce stress and stress-related mental health problems (Bartlett et al., 2019; Bhui et al., 2012; Lau and Mak, 2017; Richardson and Rothstein, 2008). The current study adds to the small amount of previous evidence that brief interventions can produce substantial improvements, at least in the short-term. It also suggests that including CFT in training may help beyond standard approaches, especially with secondary traumatic stress, which is an important risk factor for teacher mental health (Ormiston et al., 2022). CFT may also be helpful for other professions experiencing high emotional load in their roles, such as managers (Jimmieson et al., 2016).
This study has made other contributions to the field of management. It raised the theory of ‘strategy overload’ as the reason why more intensive interventions may be no more effective than shorter ones (Bhui et al., 2012; Lau and Mak, 2017; Richardson and Rothstein, 2008). Another direction for further research raised by this study was the question of whether approval from the line manager for an employee to take time off work to attend wellbeing training may, in itself, be protective of employee wellbeing by permitting and encouraging self-care. Further research could examine these hypothesised mechanisms directly.
Despite substantial short-term improvements in stress-related symptoms of some staff, a substantial proportion of employees recruited for this study remained in the clinical range for burnout and secondary traumatic stress at post-intervention. This points to important considerations for the sustainability of the workforce. It may be that higher levels of workplace wellbeing support over longer periods are needed for some staff. To prevent staff attrition from stress-related mental illness, it is also important to address primary organisational sources of stress through systemic change. Previous studies have found that teacher burnout is associated with high demands of non-teaching-related workload, including administrative load (Lawrence et al., 2019), and emotional exhaustion from balancing work and family demands (Rajendron et al., 2020). Future organisational research could investigate how to improve the sustainability of teaching roles, perhaps by reducing non-teaching-related responsibilities or providing extra time for such work.
Teachers and other school employees in Australia have always played an essential role in supporting their students and communities through challenges and disruptions. This has never been more so than in recent times with significant increases in student mental health issues and anxiety about educational attainment, future job prospects and the impact on their family. Layered on top of this, are family units that are continuing to struggle with serious financial, housing, employment and health pressures and environmental disasters from climate change. The importance of a stable, consistent and high-quality education workforce has never been more important for Australian families. With frontline educational employees spending so much of their time interacting with people and supporting others with stressful situations, some risk of secondary traumatic stress, as well as burnout, may be inherent to these roles.
The current study suggests that brief PD that addresses risk and protective factors may be impactful in reducing burnout and that inclusion of brief CFT training may enhance outcomes of secondary traumatic stress, fear of compassion and compassion satisfaction. The aim of CFT is to cultivate compassion and, although not measured here, greater levels of compassion and lower fears of compassion are significantly associated with better physiological health, as measured by parasympathetic activity (Di Bello et al., 2020; Kirby et al., 2017a). Another RCT found that CFT reduced parasympathetic activity of school employees (Matos et al., 2022); thus, a benefit of CFT could be that it increases the ability of school employees to physiologically regulate the threat experienced in school contexts. Thus, CFT not only aims to reduce threat (e.g. traumatic stress and anxiety) but also improve a sense of safety that is reflected physiologically in improved parasympathetic regulation. In addition, CFT significantly increases satisfaction with professional life (Matos et al., 2022), which suggests CFT increases the value and meaning school employees derive in their professional work. A fully powered RCT is likely to provide definitive evidence of this, particularly if it includes additional physiological measures that can assess for parasympathetic regulation (e.g. heart rate variability).
The results of this study are best interpreted in the context of its strengths and limitations. Strengths included that the intervention took place in the workplace, used an RCT design and an active control group. However, there were several limitations. First, it may be that having the two workshops on the same day for the CFT group reduced opportunities for employees to implement strategies from both workshops, which may have resulted in less impact than the interventions may have had, if delivered on separate days. Furthermore, the CFT group had 2 hours more input than the Standard PD group; although this does not in itself explain the outcomes well, making contact time the same for both conditions would prevent this potential confound. Second, randomisation was not totally successful in making the two groups comparable; initial differences between groups on stress, depression and resilience may account for better performance of the control group on these outcome measures; this would be especially true if CFT is more effective for employees who have higher levels of stress and depression. Third, the sample was mainly female; although this is representative of Australian school employees, the results may not necessarily be true for males or gender diverse employees. Fourth, this study measured outcomes over just a few months. Further research could track outcomes over a longer period of time to find out if improvements are sustainable. Fifth, like most psychological intervention studies we relied on self-report measures. Assessing objective measures like parasympathetic activity (e.g. heart rate variability) would enhance the methodological rigour of the research. Fifth, research has found that the more one practices CFT exercises, the greater the benefit (Kim et al., 2020). We did not measure how often school employees listened to the recorded practices we made available during the study period. It is possible a dosage effect was present, and that employees who listened to the CFT practices more frequently benefitted more; we suggest future research measures and tests dosage as a possible moderator.
In summary, the current study functioned as a pilot for examining whether inclusion of brief compassion-focussed training enhanced outcomes of a Standard PD workshop in reducing stress-related mental health problems. This paves the way for a full trial. Our results suggest a sample of 200–250 employees would produce sufficient power to demonstrate significant differences between conditions in reducing secondary traumatic stress and improving resilience. This further study could address limitations in the current study, including by addressing the difference in timing between conditions; this could be done by holding the CFT workshop on a separate date, and offering extended time on Standard CFT material to the control group. This would increase opportunities for mastery of skill and implementation of practices for both programmes.