
Abstract
Delirium is the most common in-hospital complication affecting older adults with acute hip fractures. Current evidence demonstrates inconsistent associations between anaesthetic type for acute hip fracture surgery and postoperative delirium. Using the Australian and New Zealand Hip Fracture Registry database, we conducted a retrospective cohort study of patients aged 50 years and over who underwent acute hip fracture surgery between 2015 and 2020. The incidence of delirium in patients who received general anaesthesia alone or combined with a regional technique, versus those who received spinal or regional anaesthesia was assessed. Multivariable multilevel logistic regression was used to test associations between anaesthetic type and delirium controlling for known confounders. Finally, given hospital variation in preference for anaesthetic type, an instrumental variable analysis was performed to include the effect of both known and unknown confounding. Of 35,252 patients, 25,682 (72.9%) patients received general anaesthesia, and 9570 (27.2%) patients received spinal or regional anaesthesia for their hip fracture surgery. A higher proportion of patients who received general anaesthesia developed delirium than those who received spinal or regional anaesthesia (40.6% vs. 35.7%, odds ratio (OR) 1.23, 95% confidence intervals (CI) 1.18 to 1.30, P < 0.0001). After adjusting for known confounders, general anaesthesia patients were at slightly increased odds of developing delirium (OR 1.14, 95% CI 1.04 to 1.25, P = 0.0052). However, the instrumental variable analysis found no statistically significant difference between groups (OR 1.03, 95% CI 0.99 to 1.07, P = 0.141). Therefore, while a weak association was found between general anaesthesia exposure and postoperative delirium, an instrumental variable analysis to compensate for unmeasured confounding showed no causal association between general anaesthesia and postoperative delirium.
Keywords
Introduction
Proximal femoral fractures are a common yet deleterious consequence of falls. They are most likely to occur in community dwelling older adults who have multiple medical comorbidities contributing to their degree of clinical frailty. 1 Despite ongoing work to improve hip fracture care through clinical care standards, 30-day mortality is reported at 8% with a one-year mortality of 22%. 2 There is also a significant association with functional decline, with almost 50% of hip fracture patients experiencing a sustained deterioration in the performance of activities of daily living and mobility, which has important implications on quality of life and the need for residential aged care. 3
Many older adults experience complications during their hospital stay including delirium, sepsis, cardiovascular events and venous thromboembolism. 4 Delirium is a complex clinical syndrome characterised by impaired attention, consciousness and cognition that develops over a short period of time and fluctuates throughout the day. 5 It is well established that risk factors for delirium include age greater than 80 years, living in a residential aged care facility, and a pre-existing diagnosis of dementia. 6 Older patients undergoing orthopaedic surgery are also three times more likely to experience delirium compared with those undergoing non-orthopaedic surgery. 6 Due to the significant adverse outcomes associated with delirium as well as limited evidence for effective delirium treatment, there has been a shift in focus towards delirium prevention strategies. 7
In line with such efforts, the potential influence of anaesthetic modality on the incidence of postoperative delirium has become a topic of interest in recent literature. In Australia and New Zealand, 98% of patients with hip fractures undergo surgery and thus will require anaesthesia, which is broadly categorised into general (GA) or regional/spinal anaesthesia (non-GA). 1 Seventy-one percent of New Zealand patients and 75% of Australian patients undergo a GA alone or in combination with a regional technique for their acute hip fracture surgery. 1 Smith et al. 6 conducted a systematic review and meta-analysis of 6704 patients undergoing hip fracture surgery, which encompassed 32 studies and a total of 2090 patients with delirium. They identified there was nearly a two times greater risk of developing delirium if the patient was aged over 80 years, or lived in a residential care facility pre-admission, and nearly six times the risk of developing delirium if they had a premorbid diagnosis of dementia. Interestingly, they found no statistically significant difference between anaesthetic type, nor with a number of intraoperative variables (medication use; use of sedation; anaesthetic type and duration; intraoperative blood pressure; intraoperative blood loss), and the incidence of postoperative delirium (POD). 6 Wu and colleagues’ meta-analysis of 104,572 patients identified conflicting associations between anaesthetic type and POD. 8 Once two studies were excluded to resolve heterogeneity, they found that general anaesthesia has a significant effect on rates of POD, possibly due to the use of propofol and its interruption of neuronal processes. However, some studies also suggested that regional anaesthesia potentially increases the rates of delirium, possibly due to lower systolic blood pressure, oxygen saturations or depth of sedation. This hypothesis was challenged by the recently published regional anaesthesia versus general anaesthesia (RAGA) trial, a multicentre randomised controlled trial (RCT) that compared regional anaesthesia with general anaesthesia for acute hip fracture surgery with respect to the development of POD. Interestingly, it concluded that regional anaesthesia without sedation did not significantly decrease the rates of POD in older patients undergoing neck of femur (NOF) surgery. 9
This study is a retrospective cohort analysis that aimed to examine the association between anaesthetic type and the incidence of postoperative delirium in patients undergoing acute hip fracture surgery. We analysed the existing Australian and New Zealand Hip Fracture Registry (ANZHFR) data between 2015 and 2020, which included patients over the age of 50 years who underwent hip fracture surgery. We hypothesised that patients who underwent a GA for hip fracture surgery would experience a higher incidence of POD than those who did not undergo a GA for this procedure. The primary outcome of interest was in-hospital acute delirium. We also performed an instrumental variable (IV) analysis in order to examine potential causal associations between GA exposure for acute hip fracture surgery and the development of POD. Delirium is a complex, multifactorial entity which is well suited to evaluation by IV analysis as this technique removes both known and unknown confounding such that causation can be established, and it makes use of institutional variation in the exposure of interest. 10
Methods
Data source
The data for this project were obtained from the ANZHFR database, which collected data from 117 Australian and New Zealand hospitals involved in the initial and/or operative management of fractured NOF patients. Information entered into the database included de-identified patient demographic data and information pertaining to seven quality improvement criteria—namely, care at presentation, pain management, orthogeriatric model of care, timing of surgery, mobilisation and weightbearing, minimising risk of another fracture and transition from healthcare. Registry data were linked to the National Death Index to provide date of death. Ethical approval was obtained through the University of New South Wales Human Research Ethics Committee (HC220406).
Study population
We identified patients aged 50 years and over who were admitted to an Australian or New Zealand hospital with a hip fracture and received operative management of their fracture between 1 January 2015 and 31 December 2020 inclusive. Patients who were assessed for delirium during the acute hospital admission and had a known anaesthetic type were included in the analysis. Patients who were treated non-operatively (n = 2012), or for whom anaesthetic type was unclear or unknown (n = 1106) were excluded. Surgical intervention was by sliding hip screw, cannulated screws, intramedullary nail, hemiarthroplasty or total hip arthroplasty (cemented or uncemented).
Anaesthetic type was coded as either GA, GA and spinal or regional anaesthesia or spinal or regional anaesthesia only. It was not known from registry data which patients may have received sedation as sedation was not one of the coded inputs into the registry. That is, it is possible that some patients who were exposed to deep sedation without an artificial airway may have been coded as having a GA, GA and spinal/regional anaesthetic, other anaesthetic type or unknown anaesthetic type. Therefore, to categorise patients according to anaesthetic type, any patient who was coded as exposed to a GA either as part of either spinal/regional anaesthesia or GA alone were included in the GA group, and the remaining patients were included in the non-GA group.
Patients were screened for their baseline cognition following admission to hospital. This assessment took place as part of a preoperative cognitive assessment using a validated tool such as the abbreviated mental test score (AMTS), standardised mini-mental state examination (SMMSE), modified mini mental state exam (3MS), general practitioner’s assessment of cognition (GPCOG), the rapid clinical test for delirium (4AT), the Rowland universal dementia assessment scale (RUDAS) and the Kimberley indigenous cognitive assessment (KICA). 12 This assessment determined if that patient had normal cognition, impaired cognition or known dementia prior to admission, and served as a preoperative cognitive baseline.
Patients were then assessed for the presence of delirium in the week following surgery for their hip fracture. Delirium is defined as an acute disturbance in consciousness, attention, cognition and/or perception, and may have been characterised by agitation and restlessness (hyperactive delirium), quiet and withdrawn behaviour (hypoactive delirium) or features of both (mixed delirium). 12 Delirium was assessed by a validated tool such as the confusion assessment method (CAM), confusion assessment method for intensive care unit (CAM-ICU), the 3-minute delirium assessment tool based on the CAM algorithm (3D-CAM) or the 4AT. Only patients who underwent delirium screening were included in the final analysis. Those who were not assessed or in whom the delirium assessment was not known were not included. The demographic, covariate and outcome variables of interest are listed in Table 1.
Characteristics of hip fracture patients who were assessed for delirium, by anaesthetic type, Australia and New Zealand 2015–2020.
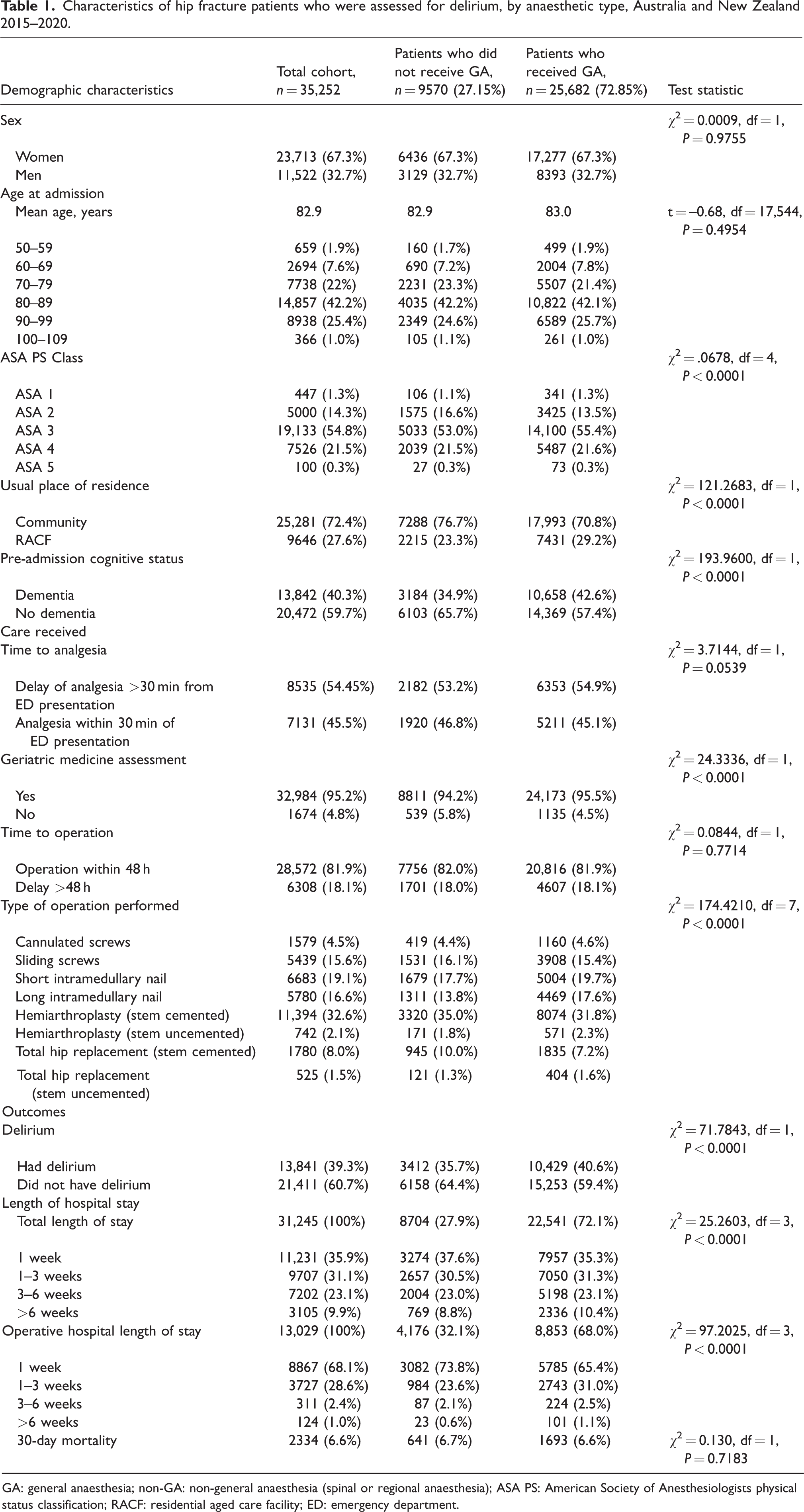
GA: general anaesthesia; non-GA: non-general anaesthesia (spinal or regional anaesthesia); ASA PS: American Society of Anesthesiologists physical status classification; RACF: residential aged care facility; ED: emergency department.
Statistical analysis
Descriptive statistics were used to describe the demographic characteristics of the hip fracture cohort, and were reported by anaesthetic type. Chi-squared tests were used to test group differences in categorical variables, and t-test for continuous variables. Logistic regression was used to determine whether there was a difference in the rate of acute in-hospital delirium (the primary outcome) between patients who received GA versus those who did not. Multivariable multilevel logistic regression was used to test the association between type of anaesthesia and delirium controlling for known confounders including age, sex, American Society of Anesthesiologists physical status (ASA PS) score, type of surgery, residential aged care and cognition. To adjust for the potential effect of clustering by hospital, hospital was used as a random effect in the models. Finally, IV analysis was performed using POD as the outcome. IV analysis is a method of determining causal associations without the need to adjust for confounders, as patient assignment to a particular hospital is random and assumes that patients did not present to hospitals based on the preference of that hospital in using GA or not. 13 IV analysis allows causal inferences to be made from observational data by controlling for unmeasured confounding. Its success in so doing relies on the selection of an appropriate instrumental variable, a characteristic that allows a patient to be exposed to the treatment of interest without having any bearing on the outcome itself, because it is itself not influenced by the same confounders that influence treatment and outcome. 11 Our study considered the natural randomness of patient assignment to a particular hospital as a suitable instrumental variable to assess causality between treatment (anaesthetic type) and outcome (incidence of POD). The variation in anaesthetic type preferred by each institution provides the treatment variation that allows this analysis. Hospital-level variation in preference for anaesthetic type was determined, and each hospital assigned a preference value equal to the proportion of all cases in which general anaesthesia is used. As the first stage test for weak instrument demonstrated that the association between hospital preference and the use of GA was strong (i.e. F statistic >105, 14 whereby our F statistic was 2927), hospital preference for anaesthetic type was used as the instrument in the IV analysis. Analyses were performed using the Statistical Analysis System (version 9.4; SAS Institute, Cary, NC, USA) and the instrumental variable analysis was performed using the applied econometrics package in R (version 4.1.1, R Environment for Statistical Computing, Auckland, New Zealand).
Power calculation
We aimed to detect a difference in the rate of delirium between hip fracture patients who had GA compared with those who did not undergo GA for their procedure. Using data reported from the 2021 ANZHFR Annual Report, 27% of hip fracture patients overall developed POD and 71% of patients who underwent surgery received GA. 15 Based on these figures, to detect a 2% difference in delirium between the groups, with 90% power and α = 0.05, 24,797 individuals are required (17,586 GA group, 7211 non-GA group). With a total of 35,252 eligible patients (25,682 in the GA group and 9570 in the regional/spinal anaesthesia group), our study was adequately powered.
Results
Demographics
A total of 74,203 patients were included in the ANZHFR data between 2015 and 2020. Of these, 70,879 (95.5%) patients were aged over 50 years and underwent operative intervention with a known anaesthetic type. A total of 35,252 patients had a documented assessment for delirium within one week postoperatively (Figure 1). Over two-thirds of these patients underwent GA (25,682; 72.8%), either as a lone anaesthetic or in combination with a regional or spinal technique. The remaining 9570 patients (27.2%) received non-GA. The distribution of demographics was comparable between study groups across most variables (Table 1). The majority of patients were women (23,713; 67.3%), and had an average age of 82.9 years. Forty percent of patients had known preoperative cognitive impairment, and 27% of patients were living in a residential aged care facility prior to admission.
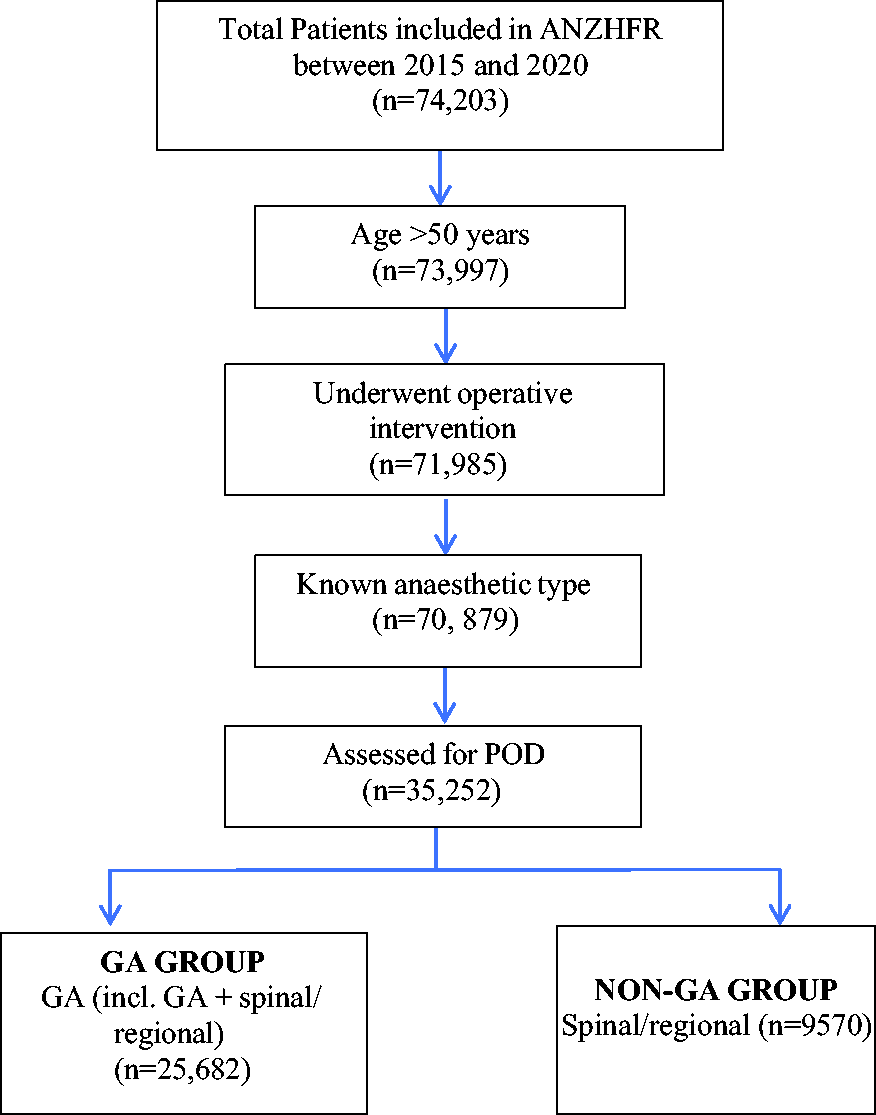
Inclusion of patients from Australian and New Zealand Hip Fracture Registry (ANZHFR) data. POD: postoperative delirium; GA: general anaesthesia; non-GA: non–general anaesthesia; n: number of patients.
The unadjusted univariate analysis demonstrated 23% increased odds of POD following GA exposure, with an incidence of 40.6% in the GA group compared with 35.7% in the non-GA group (odds ratio (OR) 1.23, 95% confidence interval (CI) 1.18 to 1.30, P < 0.0001). However, when adjusted for known confounders, the magnitude of this association reduced to a 14% increased odds of POD post GA exposure (OR 1.14, 95% CI 1.04 to 1.25, P = 0.005; Figure 2). The association with the type of anaesthesia was small when compared with other variables in the model. In particular, having a preoperative diagnosis of dementia was associated with 5.25 times increased odds of developing POD, and ASA PS 4 and 5 patients were at 2.5 times and 2.9 times increased odds of developing POD, respectively. Finally, we performed an IV analysis in order to remove the effect of unknown confounding and draw causal inference from our dataset. The IV analysis demonstrated that the association between GA and the development of POD was not statistically significant, and as such, GA exposure is not causally associated with POD development (OR 1.03, 95% CI 0.99 to 1.07, P = 0.14; Figure 3).
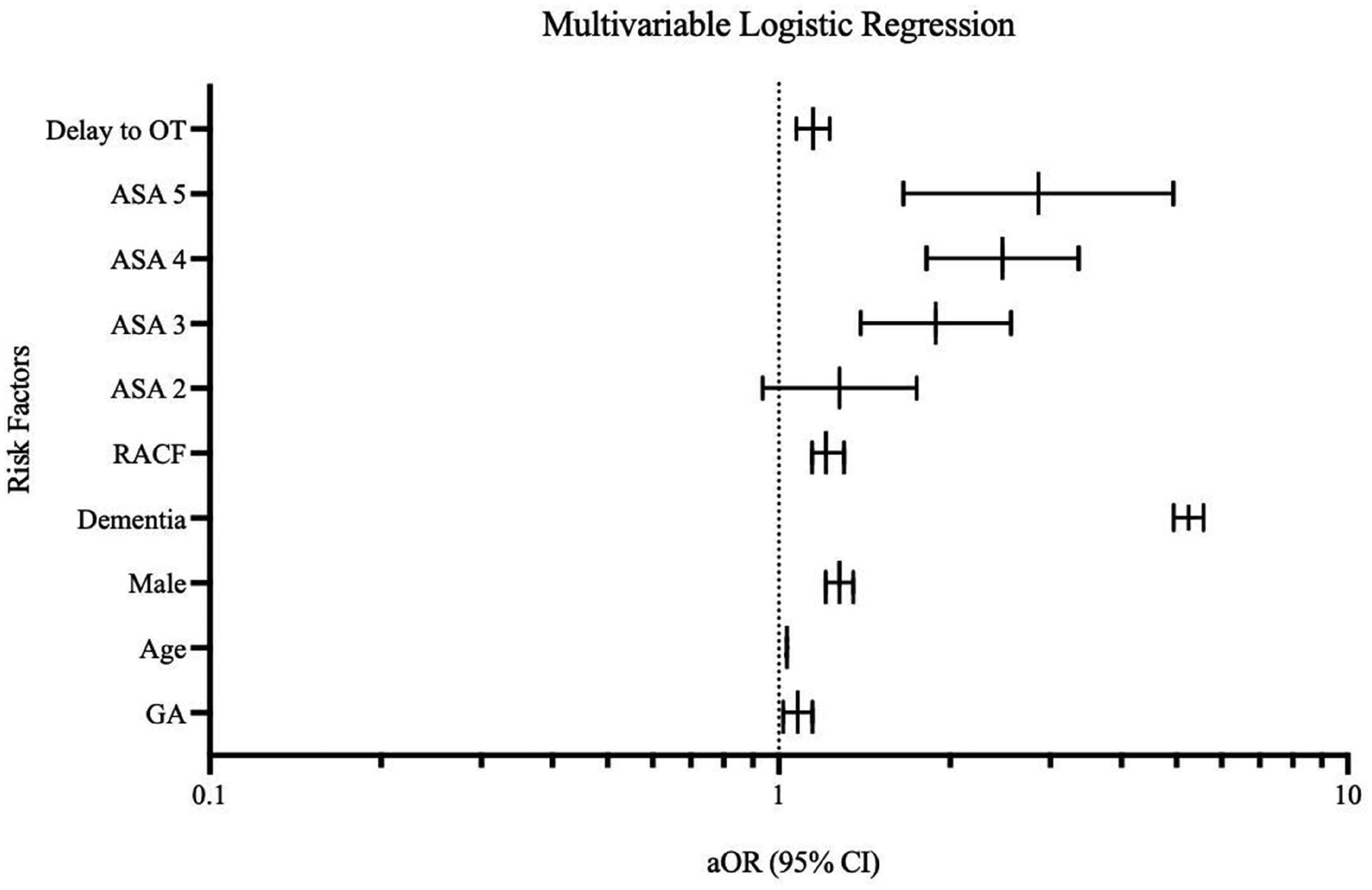
Multivariable logistic regression. OT: operating theatre; ASA: American Society of Anesthesiologists physical status classification; RACF: residential aged care facility; GA: general anaesthesia; aOR: adjusted odds ratio; CI: confidence interval.
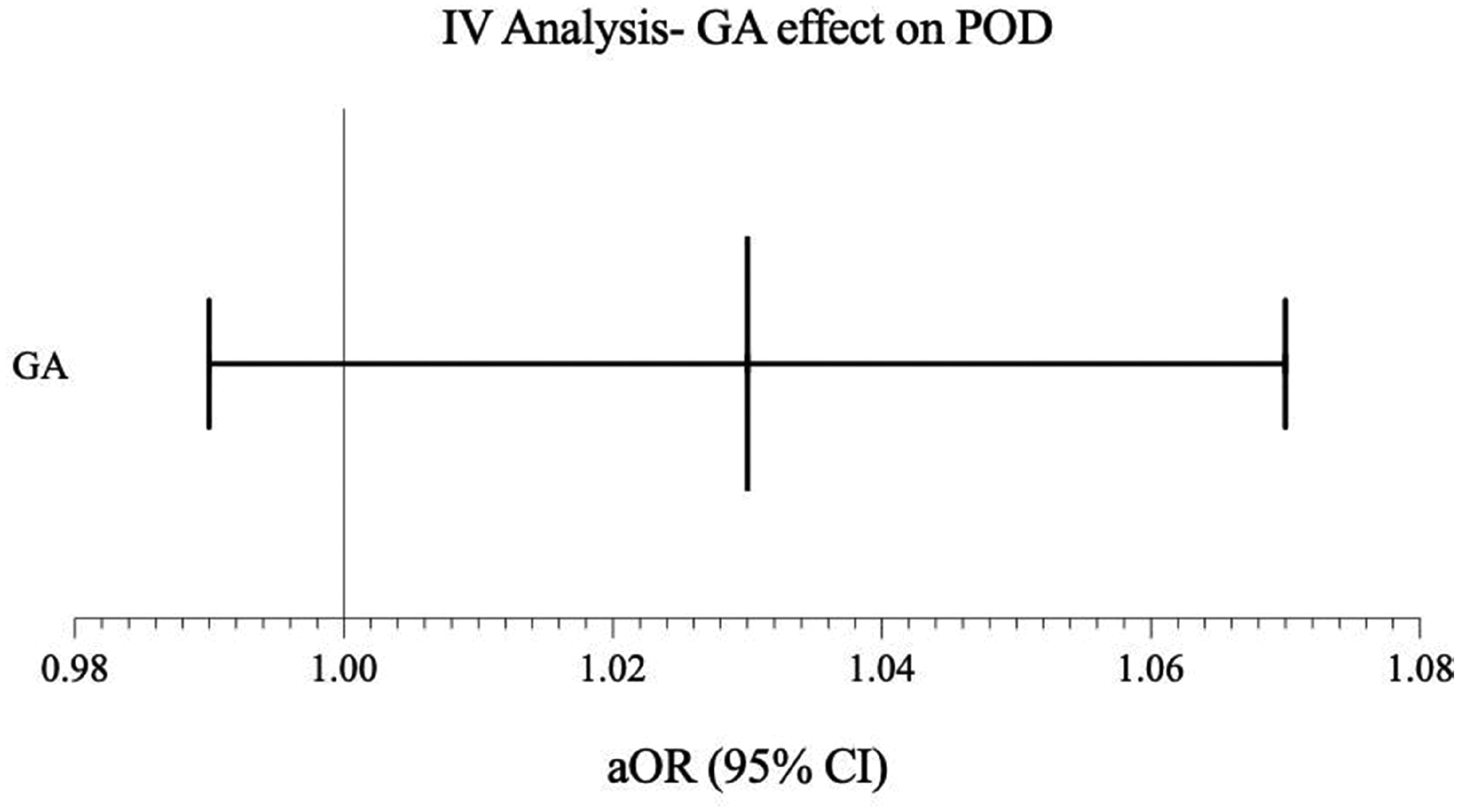
Instrumental variable (IV)analysis. GA: general anaesthesia; POD: postoperative delirium; aOR: adjusted odds ratio; CI: confidence interval.
Discussion
This study aimed to investigate the association between anaesthetic type (GA vs. non-GA) and POD in older patients undergoing acute hip fracture surgery. We included a large number of patients (>35,000) from 93 hospitals across Australia and New Zealand over a 5-year period. Our large sample size ensured that our study was adequately powered with respect to the primary outcome. Patients included in this study were from rural, regional and metropolitan hospitals across the two countries, which increases the external validity of our results. The data were uniformly collected against registry-specified data criteria, which improved consistency across all contributing hospitals. Relevant risk factors were explored and their effect minimised with relevant multivariate regression and novel IV analysis.
Our unadjusted univariate analysis demonstrated that an association exists between undergoing GA for fractured NOF surgery and POD. The strength of this association was minimised when relevant risk factors were explored by way of a multivariable logistic regression. Namely, we found that the largest drivers of this association were dementia, and an ASA PS score of 4 or 5 as surrogates for complex comorbidity. This finding is consistent with current literature that identifies dementia, increased ASA score and complex comorbidities as important risk factors associated with POD.6,9 Our IV analysis is a novel approach to overcoming the effect of unknown confounders in an observational study. The selection of hospital preference for anaesthetic type was a strong instrument, and subsequent use of this instrument in the IV analysis demonstrated that GA does not cause POD. Overall, our findings are consistent with those of the recently published randomised superiority REGAIN multicentre trial, which found a similar incidence in the rates of POD between 1600 patients who underwent either spinal anaesthesia or general anaesthesia for hip fracture surgery. 16
One limitation of our study is the lack of temporal sequencing with respect to the timing of delirium assessments, as this was not standardised across sites. Ideally, it would have been helpful for patients to undergo delirium assessments pre and postoperatively with the same validated tool, acting as their own control for the development of delirium. This is consistent with the delirium clinical care standard, which identified that 10–18% of patients aged over 65 years are already experiencing delirium at the time of presentation and up to 8% develop delirium during admission, thus more than one assessment may be necessary to identify all patients with delirium. 17 We attempted to account for this by including the preoperative cognitive assessment to serve as a preoperative cognitive baseline (rather than a preoperative delirium assessment, as this was not known), and performing a subgroup analysis on these patients which demonstrated that there was no difference in the incidence of POD between this subgroup and our overall study cohort.
Furthermore, it was unclear from the coded inputs into the registry which patients may have received sedation as part of their anaesthetic. An attempt was made to account for this by including any patient who was known to have been exposed to anything defined as GA in the GA group (in case this captured some patients who had deep sedation). However, it is possible that some non-GA patients may have been exposed to sedative drugs, thereby introducing misclassification bias. It is also unclear if GA patients were exposed to intravenous agents, inhalational anaesthetics or a combination of the two, or if benzodiazepines, ketamine or opioids were utilised. The literature surrounding the potential contribution of ketamine towards POD rates is also inconsistent with some studies suggesting exposure increases the risk of POD, and others contesting its role as a causative agent and instead supporting its use as a preventive measure against the development of postoperative cognitive dysfunction.18,19 Finally, the depth of anaesthesia and potentially associated periods of hypotension were not known from registry data. Intraoperative hypotension is particularly important to account for as current international consensus guidelines support the avoidance of intraoperative hypotension in order to improve patient outcomes in patients undergoing NOF surgery. 20
In summary, our study suggests that while adjusted regression analyses may show an association between undergoing general anaesthesia for acute hip fracture surgery and developing delirium postoperatively, this association is likely to be due to residual confounding from unmeasured confounders as the causal association between these variables was not statistically significant. Clinicians should be reassured that anaesthetic modality for acute hip fracture surgery is unlikely to contribute significantly to the burden of POD, which is instead largely driven by non-modifiable comorbidities.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank Elizabeth Armstrong, Jamie Hallen, Karen Lee, Narelle Payne, Niamh Ramsay and James Wright of the ANZHFR, as well as staff at contributing hospitals.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AT was sponsored by the University of Queensland Mayne Academy of Critical Care to present this research at a conference. The remaining author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.