
Abstract
Medical emergency team (MET) activations were designed to improve patient safety and outcomes by providing timely and specialised care to patients experiencing clinical deterioration. The primary objective of this study was to describe the association between MET events in the early (24-h) postoperative period and in-hospital mortality as well as length of stay. A retrospective data linkage study was performed of prospectively collected data from patient administrative data and the MET database at Launceston General Hospital located in Tasmania, Australia. Over five years, 109,116 operating room cases fulfilled the inclusion criteria, of which 85,235 were the first operating room case in a unique admission episode after exclusions. A MET event within the first 24 h after surgery was associated with an increased median length of stay from 0.16 to 4.00 days with a median difference of 2.96 days (95% confidence interval (CI) 2.86 to 3.08) and more than doubled the hazard of mortality for each day a patient remained in hospital after completion of surgery (hazard ratio 2.3, 95% CI 1.9 to 2.8). Emergency surgical patients were at higher risk. Of recorded MET triggers, cardiac arrest was the most strongly associated event with in-hospital mortality. Notably, staff concern as a trigger for MET activation was associated with a hazard nearly as great as chest pain. Other MET triggers that reached statistical significance were bleeding, respiratory rate more than 36/min, peripheral oxygen saturations less than 84% and systolic blood pressure less than 80 mmHg. Despite being frequent, MET events should be regarded as a serious marker of an adverse patient journey that may warrant higher resource allocation.
Keywords
Introduction
Lee and colleagues first developed and reported on medical emergency team (MET) activation in Sydney’s Liverpool Hospital in 1995.1 Since then, the use and effectiveness of the MET has been described in the literature for its association with reduction in mortality of hospitalised patients 2 and has now become widespread and mandated by the Australian Commission on Safety and Quality in Health Care (ACSQHC). MET activation was designed to improve patient safety and outcomes by providing timely and specialised care to patients experiencing clinical deterioration. Trigger events for MET activation are characterised by a breach of a specific and/or group of clinical thresholds that indicate an acute deterioration in a patient’s physiological or mental state. Tasmanian hospitals utilise charts from the Observation and Response Chart project piloted by the ACSQHC. 3 These charts outline predetermined thresholds for various physiological parameters, prompting escalation of review in the event of a threshold breach, with the highest tiers being MET team activation or, in extreme cases, a ‘code blue’ call response. The criteria in use at our hospital are listed in Appendix 1.
While the MET system has been associated with reduced in-hospital mortality and cardiopulmonary arrest, 4 a systematic review and meta-analysis conducted by Maharaj et al 5 identified that only limited studies are available regarding the outcomes after MET trigger events that occur early in a patient’s postoperative journey. A search of current available literature suggests that postoperative patients who trigger MET events are a vulnerable population, and there is an association between MET activations at any point during hospital admission and high rates of morbidity and in-hospital mortality, 6 with a high associated cost. Weingarten et al described how 78.5% of early postsurgical MET events that occurred within 24 h of surgery 7 were a surrogate marker for early clinical deterioration outside of a pre-designated critical care admission, and focused their study on the perioperative and intraoperative aetiology of such events.
To build on this, we conducted a retrospective observational study to describe the impact of MET events that occur within the first 24-h postoperative period in the general surgical population of a regional referral centre. The aim of our study was to address the hypothesis that patients triggering a MET event within the 24-h period following surgery have higher in-hospital mortality rates and longer length of stay (LOS) compared with those who do not. We were interested to identify a higher-risk group that may benefit from escalated clinical care, and assess the associated impact this event may have on their postoperative journey.
Methods
Study design
A retrospective observational data linkage study was performed on prospectively collected data from the Launceston General Hospital (LGH). Ethics approval was obtained from The University of Tasmania Human Research Ethics Committee (HREC) H0028325 (H-92967) and the need to obtain consent from individual patients was waived.
Setting and participants
Launceston General Hospital is a public 386-bed hospital in northern Tasmania with approximately 15,000 separations per year. It has a surgical case-mix of general, orthopaedic, colorectal, upper gastrointestinal, urology, plastics, and ear, nose and throat specialties, with a regional referral role. Cardiothoracic, neurosurgical and burns cases are transferred out, and paediatric cases are selectively managed locally or transferred. The hospital also provides regional referral medical specialties and a Day Procedure Unit (DPU). The DPU acts as an endoscopy suite and a short-stay ward where interventional cardiology, gastrointestinal and respiratory endoscopic procedures are undertaken. These can include elective day case oesophago-gastro-duodenoscopy as well as ward patients admitted for investigation of emergency gastrointestinal bleeding.
Data collected prospectively between 1 January 2016 and 31 December 2022 were retrospectively analysed using live clinical databases. We included all cases where an admission episode occurred in the main operating room complex and DPU for both emergency and elective procedures. The first operating room episode per unique admission was included in the analysis, and all MET events within 24 h of surgery completion in this episode were measured. Patients with more than one admission were analysed by the first operating room episode in each admission. Individuals were excluded if they were under the age of 18 years, allocated to or attended the operating room with no procedure completed, undergoing cardiac angiography, organ procurement or electroconvulsive therapy. Patients who were admitted to the intensive care unit (ICU) directly from the operating room (planned or unplanned) were included in the analysis; however, this group do not trigger MET events.
An arbitrary time period of 24 h from the end of surgery was chosen as a clinically relevant window where MET events are likely to be related to the surgical episode and as a definable point of time where future services could be targeted.
Data collection
Inpatient data were collected from the LGH MET Call Database and Tasmanian Health Service patient administration data. The LGH has been routinely collecting MET and code blue calls data since 2014. We collected information via patient unique record identifiers, hospital location descriptors and time of call. Other details included were operating room area, trigger of the MET event, and patient age. Outcome measures were calculated LOS since time of surgery and in-hospital mortality within the same admission. LOS since end-time of surgery was chosen as a unifying definable physiologic event applicable to all patients. Data linkage was performed by collating data from a range of different databases and importing them into a table in a Microsoft SQL server. After linkage was completed, data were de-identified, coded with unique serial numbers and exported for analysis.
Details of MET activations
MET activations are triggered by defined breaches of predefined criteria as previously discussed and listed in Appendix 1. The LGH ICU is funded to roster the MET service with one of the 29 registered nurses who have advanced life support training and have been orientated to the role. This nurse is allocated at the beginning of their shift to the external support role to attend MET calls. An ICU registrar and medical registrar are also allocated to the team and a junior doctor from the identified home team attends. Upon activation, MET calls are logged into the MET database by switchboard staff. Immediately following management of the MET event, senior ward staff who have been directly involved in the event log into the database and select the recorded event to enter patient details and a clinical summary. This record is then locked and is unable to be edited. Later, senior ward staff from the location of the call complete a quality assurance evaluation and add follow-up data. The data are recorded and stored for future auditing and reviews.
Statistical analysis
Statistical analysis and figure creation was performed in R version 4.2.213 with dependent packages.8 –13 Median LOS between groups was compared with Wilcoxon rank sum tests. Odds ratio (OR) for overall in-hospital mortality was calculated with Fisher’s exact test. Hazard ratios were calculated from time-to-event analysis using a mixed methods Cox regression model (also known as a shared frailty model) with fixed effects for variables of interest and a random effects model for quantifying variation of outcome between individual patients and allowing for repeated measures of the same patient undergoing more than one operating room episode within different hospital admissions. The model outcome was admission mortality; patients discharged alive were censored from further analysis at time of discharge as is standard for time-to-event analysis. Records with missing data were ignored. Statistical model generation was performed on an Intel i9-13900K desktop processor with 64 gigabytes of RAM. Limitations of computational power from the size of the dataset prevented development of a nested random effects model for multiple operating room episodes within unique admissions per patient. Two models were used: the first used the number of MET events within the first 24 h postoperatively while the second used the recorded MET triggers of events. Selected factors were compared visually by Kaplan–Meier curves. For clarity, figures were limited to 60 days since time of first surgery.
Results
Participants and sample description
During the study period there were 109,116 operating room cases that fulfilled the inclusion criteria of which 85,235 were the first case in a unique admission episode and, of these, 20,200 were excluded from analysis (Figure 1). The median age at time of operating room episode was 59 years, with 28.9% aged 70 years or older. Of operating room episodes, 47.7% were for male patients. The most common admitting services were gastroenterology (27.9%) and general surgery (14.1%). The majority of admissions were elective (76.6%) and almost two-thirds of procedures were carried out in the main operating room complex. The patient characteristics at operating room presentation are included in Table 1. During this time period there was a total of 12,376 MET calls for adult patients across the hospital; 503 of these (4.06%) did not have details recorded about the call or patient and so could not be included in the data linkage. Seven hundred and ninety-eight events (681 MET calls, 117 code blue calls) occurred within the first 24 h after surgery. Additional extracts from the hospital database over the full five years have been included in online Supplementary material Table 1.
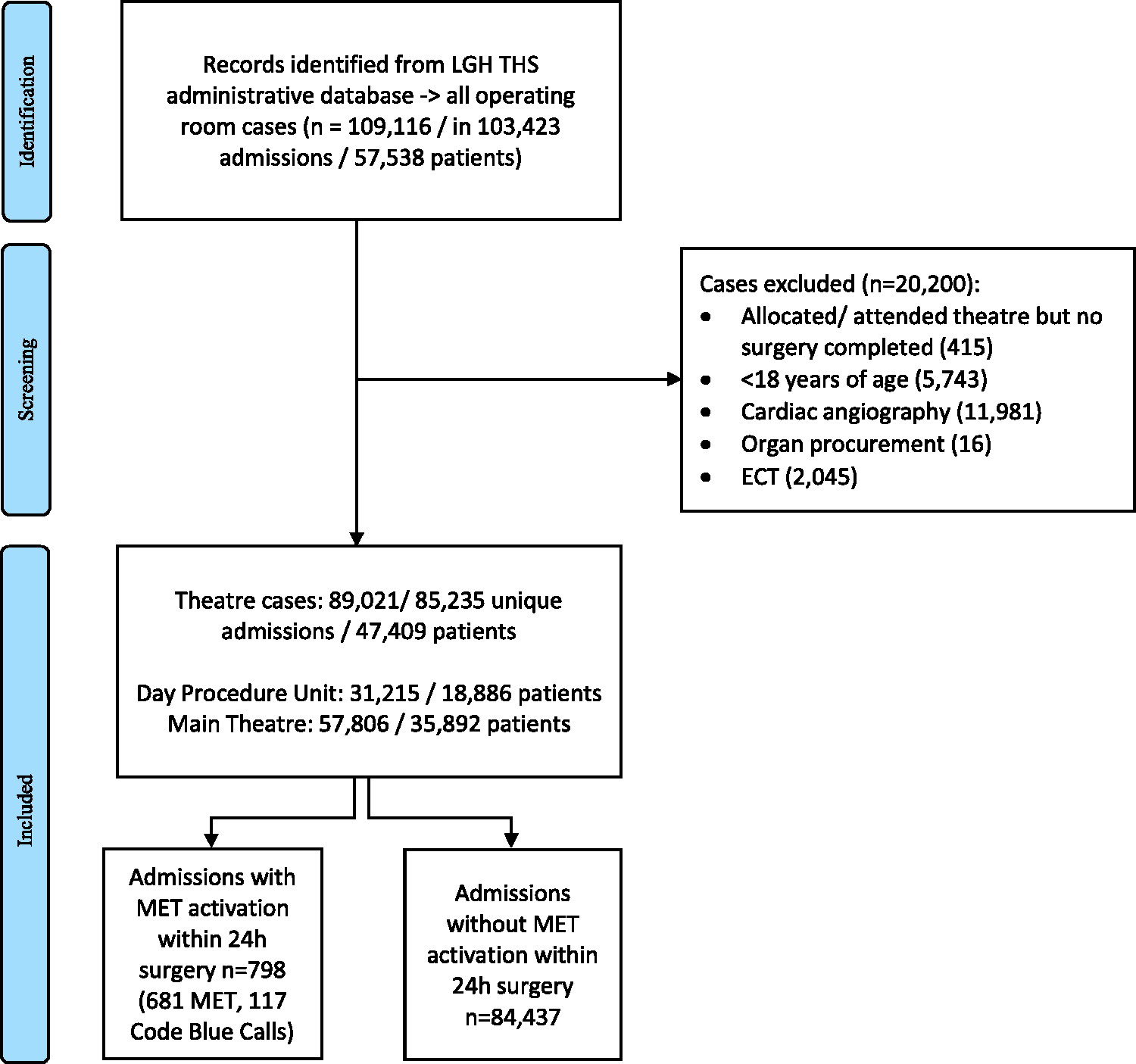
Study flow diagram. LGH: Launceston General Hospital; THS: Tasmanian Health Service; MET: medical emergency team; ECT: electroconvulsive therapy
Patient characteristics at operating room presentation, elective versus emergency.
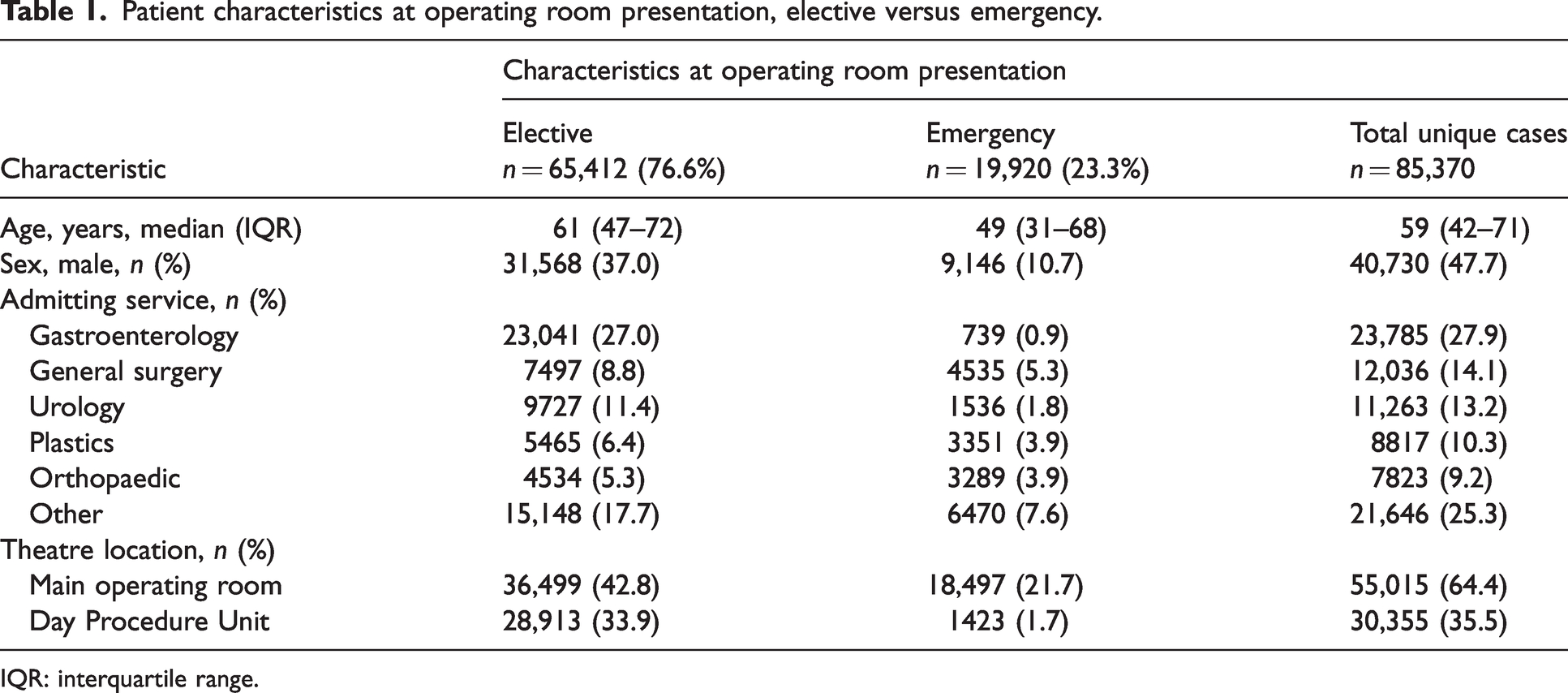
IQR: interquartile range.
Overall mortality
Three hundred and nine in-hospital deaths occurred during this time period; of these, 88 deaths within the first five days following surgery and a total of 249 within 30 days. There were 85 deaths in elective patients and 224 in emergency patients (0.13% vs. 1.12%, OR 8.74, 95% confidence interval (CI) 6.77 to 11.36, P < 0.0001) with mean ages of 73.25 (standard deviation (SD) 11.17) years and 73.29 (SD 13.61) years respectively. Of the 85 deaths in the elective group, six had a MET call in the first 24 h after surgery, compared with 24 of the 224 deaths in emergency patients.
LOS
For elective cases in the main operating room, the impact associated with a MET event was a median increase in LOS from end of surgery to discharge from 0.24 days to 4.90 days; similarly, emergency cases in the main operating room had an associated increase in median LOS from end of surgery to discharge of 1.62 days to 7.02 days. Comprehensive comparisons for the associated impact of a MET event are presented in Table 2.
Median length of hospital stay (days) from completion time of surgery to discharge by MET event in the first 24 h after surgery.
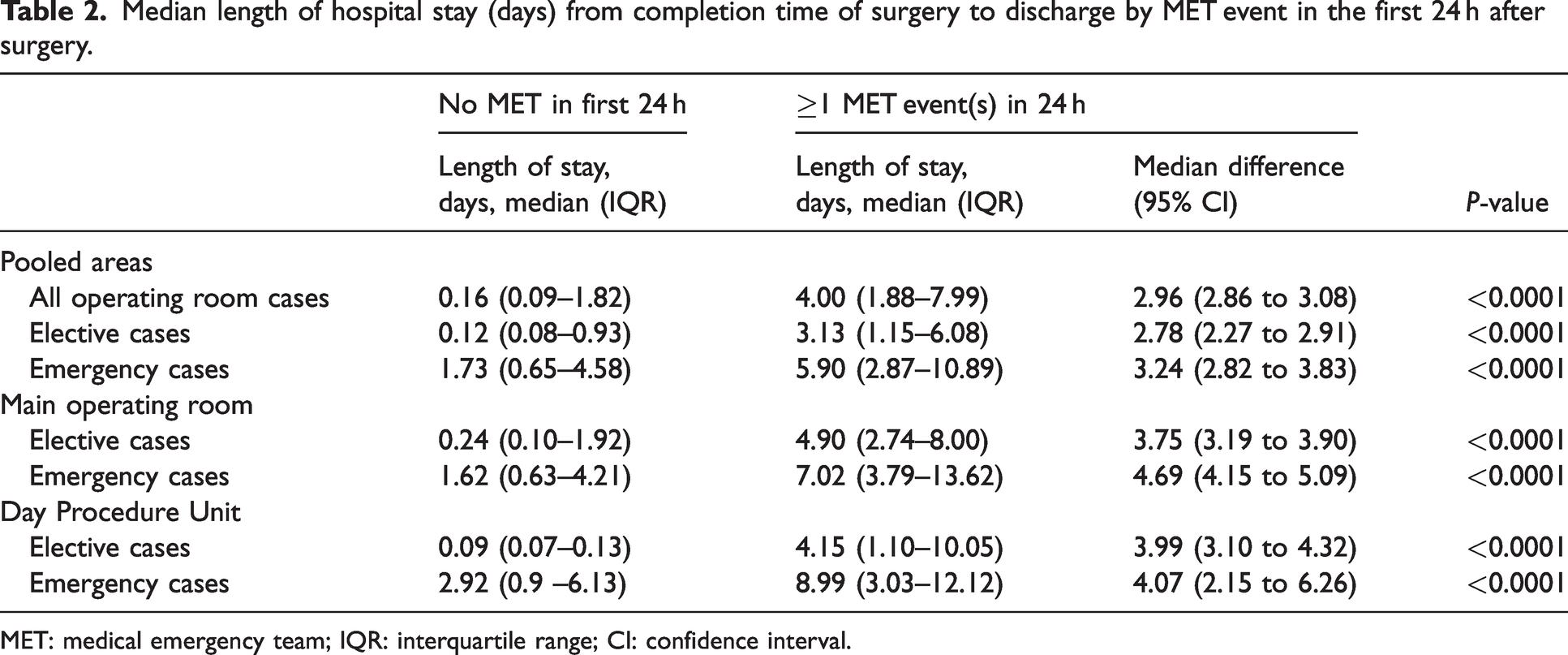
MET: medical emergency team; IQR: interquartile range; CI: confidence interval.
Time-to-event analysis
Unadjusted and adjusted multivariate mixed-effects Cox model results are listed in Table 3 and Figure 2. In the unadjusted model, any MET event within the first 24 h after surgery more than doubled the hazard of in-hospital mortality for each day that a patient remained in hospital after completion of surgery (hazard ratio 2.3, 95% CI 1.9 to 2.8).
Multivariate mixed effects Cox model results.
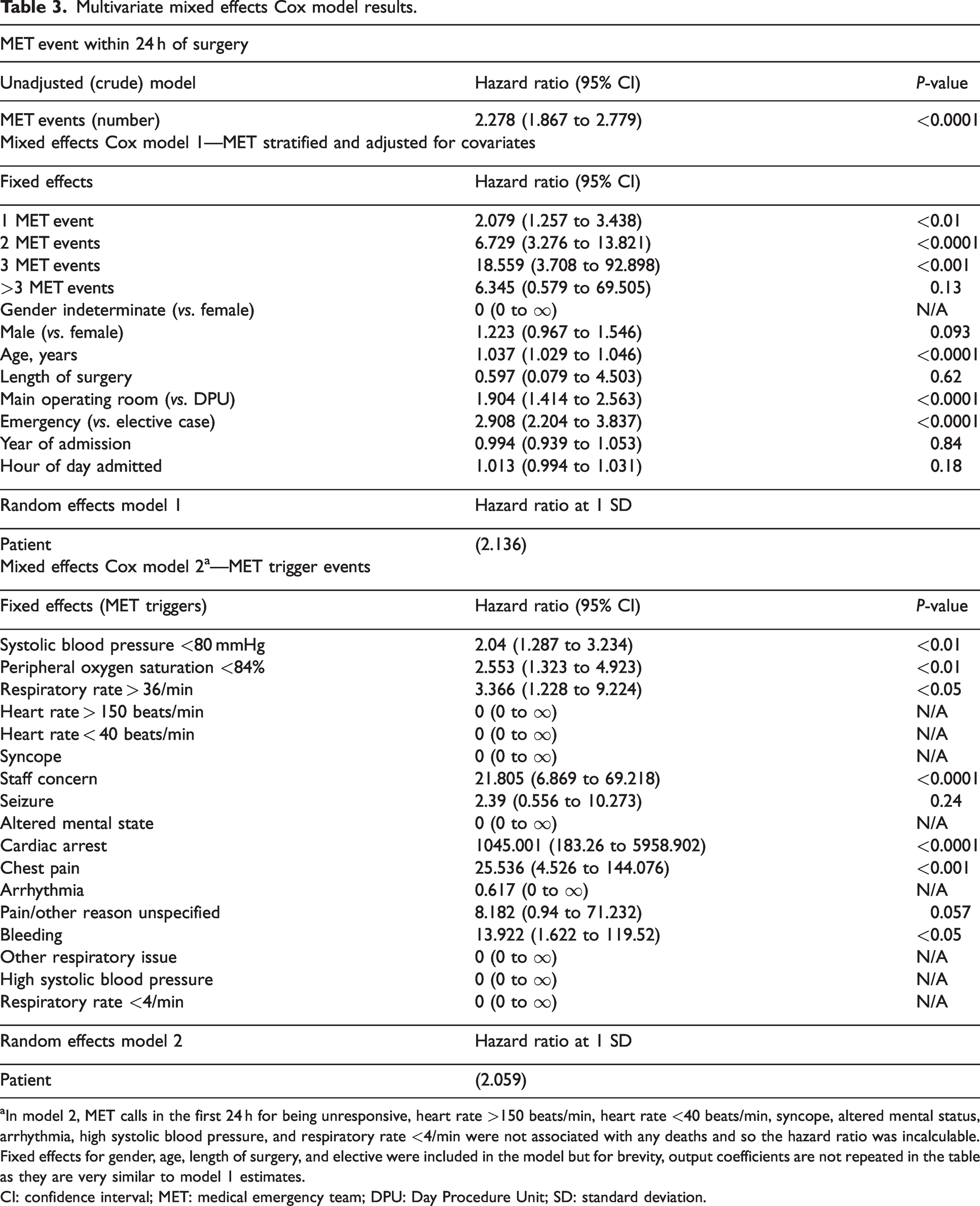
In model 2, MET calls in the first 24 h for being unresponsive, heart rate >150 beats/min, heart rate <40 beats/min, syncope, altered mental status, arrhythmia, high systolic blood pressure, and respiratory rate <4/min were not associated with any deaths and so the hazard ratio was incalculable. Fixed effects for gender, age, length of surgery, and elective were included in the model but for brevity, output coefficients are not repeated in the table as they are very similar to model 1 estimates.
CI: confidence interval; MET: medical emergency team; DPU: Day Procedure Unit; SD: standard deviation.
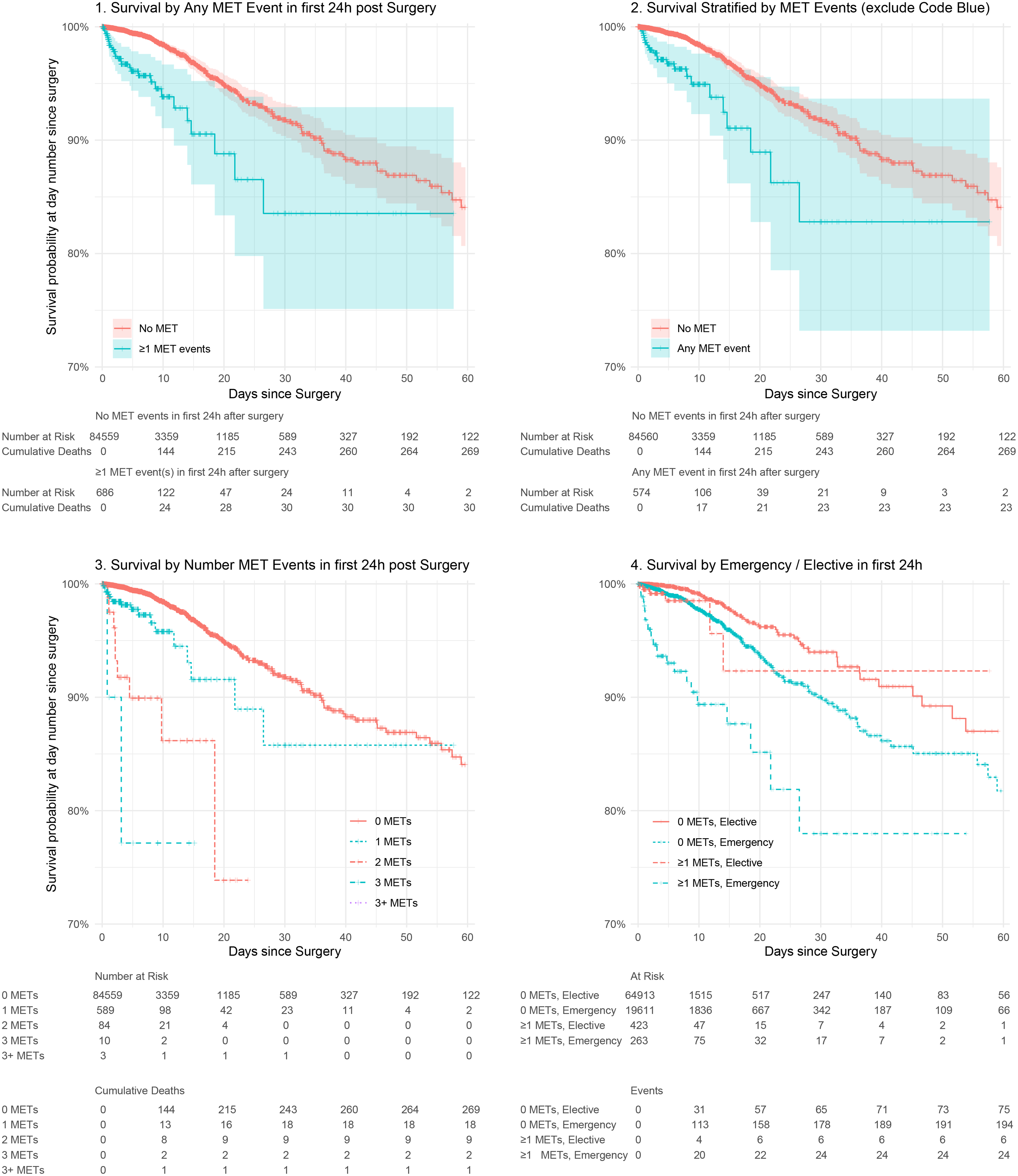
Time-to-event analysis. Bold cross marks indicate patients censored due to discharge alive. Numbers at risk are shown below each figure. As instantaneous survival curves with censoring of those discharged, these should be read as ‘for those remaining in hospital at day n, risk was y%’. MET: medical emergency team
Amongst emergency patients, 77.7% were discharged by day 5. However, of the remaining 4435 still admitted, 142 had triggered a MET call in the first 24 h postoperatively and the day 5 risk of death was 7% (95% 3.6 to 10.3) compared with 1% (95% CI 0.7 to 1.2) in those without a MET event by 24 h. Similarly, 93.4% of elective patients were discharged by day 5. However, of the remaining 4313 still admitted, the 138 who had triggered a MET call in the first 24 h postoperatively had a risk of death of 1.5% (95% CI 0.0 to 3.0) compared with 0.2% (95% CI 0.1 to 0.3) without a MET event.
Analysis stratified by number of MET calls (model 1) demonstrated significant and successively higher hazard ratios for up to three MET events in the first 24 h, though more than three was not statistically significant. Model 1 was adjusted for covariates and significant factors included age, which was associated with 3.5% increase in risk for each year (95% CI 2.7 to 4.4), operating room episode being in the DPU (hazard ratio 1.9, 95% CI 1.4 to 2.6) and being an emergency case (hazard ratio 2.9, 95% CI 2.2 to 3.8).
When triggers of MET events were included (model 2), cardiac arrest was unsurprisingly the event most strongly associated with in-hospital mortality. Notably, staff concern (hazard ratio 21.8, 95% CI 6.9 to 69.2) as a trigger for a MET call was associated with a hazard nearly as great as chest pain (hazard ratio 25.5, 95% CI 4.6 to 144.3). Other MET triggers that reached significance were bleeding, respiratory rate over 36/min, peripheral oxygen saturations less than 84% and systolic blood pressure less than 80 mmHg. Additional details regarding number of calls by trigger versus key variables has been included in online Supplementary Table 2.
In both model 1 and model 2, the random effects coefficient demonstrated that wide variation existed between patients, with approximately 16% of patients (1 SD) having 2.1 times the in-hospital mortality risk per day in hospital compared with baseline.
Repeat analysis using a subset of 37,015 patients, after excluding all in-hours elective cases who were discharged alive within 8 h of the end of surgery, yielded very similar results, the difference being that by excluding short-stay surgery cases performed in the operating room, the hazard of death in the main operating room area exceeded that for the DPU. This sensitivity analysis is included in online Supplementary Table 3.
Given the large hazard coefficient associated with cardiac arrest, we repeated model 1 with code blue call events excluded (Figure 2) to test whether MET events alone yielded the same results. Excluding code blue call events, the hazard of in-hospital mortality from a MET call was 2.535 (95% CI 1.631 to 3.94, P < 0.0001) for each day the patient remained in hospital. Age, location of surgery and being an emergency case were again significant variables.
Discussion
This observational analysis within a broad surgical caseload in a regional referral hospital over a five-year period highlights the association of increased in-hospital mortality and length of admission for patients after a MET event. Although overall survival was 99.9% for elective cases and 98.9% for emergency surgical cases, time-to-event analysis demonstrates that, of patients who remain in hospital for multiple days, those who experienced a MET event within 24 h of surgery completion had a demonstrably higher in-hospital mortality and LOS, particularly after emergency surgery.
Pragmatically, it is the subset of patients who stay multiple days that comprises the majority of patients on postoperative surgical wards. While it is logical that the more physiologically compromised patient will stay longer and have a higher risk of a poor outcome, a MET event in the first 24 h can be viewed as a significant marker that a patient is at risk for an extended stay and mortality. This early identification could serve as a trigger for a more sustained resource allocation beyond the immediate resuscitation focus of the MET team.
We acknowledge several limitations inherent in our study. First, the study was conducted in a single centre and therefore the generalisability of findings may be limited owing to the specific population, time period and organisational resource allocation decisions. Furthermore, being retrospective and over five years, our study is prone to alterations in demographics and patient selection, particularly the possibility that restrictions imposed by the COVID-19 pandemic in the first half of 2020 could have affected outcomes. The MET call reporting database has some limitations too—there is a small percentage of calls that, due to high staff clinical demand, are not entered into the database, and we acknowledge that it includes both objective and subjective information describing MET events recorded by immediate responders; however, the trigger events used in this study are clearly defined. It should also be noted that the standardised observation and response charts endorsed by ACSQHC which were utilised in Tasmanian hospitals at the time of this study had lower MET trigger thresholds than some others referenced in the literature.14,15 Operationally this is mitigated by having urgent clinical review triggers that prompt a response (defined in Appendix 1). However, this may mean that patients who triggered a MET call in this study are ‘sicker’ than those who triggered a MET call in other studies in the literature.
In our study we aimed to limit this impact by defining the time period as 24 h from the end of surgery to be a clinically relevant window where MET events are likely to be related to the surgical episode and by using a robust statistical model that accounts for repeated events on the same subject.
Despite the known limitations of retrospective datasets, our MET call reporting database and surgical case-mix data are well established clinical systems used for hospital quality reporting from prospectively entered events. By including all admissions where an operation was performed rather than retrospectively selecting a sample, we have been able to provide a service-level picture of outcomes from surgery although there will be factors specific to our institution that are not generalisable.
Bias effects in time-to-event analysis are well described. In this study the major consideration is right censoring by not having final mortality dates for surgical patients, discharged home alive, which may alter survival estimates. For this reason, our time-to-event results require strict interpretation as the instantaneous risk of in-hospital mortality at that specific time point (number of days) after surgery in each group. This risk rises with each day in hospital and by the factors with a positive significant hazard (Table 3). It should not be interpreted as the overall risk of a surgical procedure or of being in an operative area.
Left censoring, where the inciting event occurs before the study starts, is a risk for emergency patients in this study. We regarded the surgical event as the major physiologic insult, which is a reasonable assumption for elective patients, but could be hours to days earlier for some emergency cases. That said, the anaesthetic and surgical process is still a major decision and care-point, and pragmatically is a key clinical event. This is also partially mitigated by the sickest patients being identified for direct transfer to ICU from the operating room and are thus not eligible to trigger a MET event. We hope to highlight that, particularly for those remaining, the time of surgery completion should mark a crucial opportunity to reassess treatment goals and manage with intention.
Caution should also be applied in interpretation of the survival curves, keeping in mind that the plot represents the instantaneous hazard (‘risk’) at that day after surgery. In the results, we cite the example of the risk at day 5 in elective and emergency patients and, from the Kaplan–Meier curves, the risk at other days from surgery can be inferred.
Regarding interpretation of results, it is in keeping with the existing literature that older patients 16 and those admitted for emergency surgical intervention have worse outcomes, with increased risk of inpatient mortality when compared with elective patients where more preoperative conditioning and selection occurs. Although initially it seems counter-intuitive that procedures done in the DPU had a higher hazard of in-hospital mortality with each day of admission, this can be reasoned that a multiple-day stay after what is often a less invasive procedure in the DPU is likely a marker for more severe patient morbidity than a multiple-day stay after major surgery in the main operating room complex. Further sensitivity analysis after excluding all in-hours elective cases who were discharged alive within 8 h of the end of surgery showed the hazard of death in the main operating room to exceed that for DPU patients.
Our findings are consistent with those described in existing literature where surgical patients who have MET events have associated increased LOS and a more complicated hospital course with higher mortality rates,16 –18 particularly for those who trigger multiple MET activations. Notably, from our research, even with MET events isolated from code blue call events (which have a higher potential to be terminal), patients have a significantly heightened hazard of in-hospital death. Our results further enhance the current literature by describing the temporal relationship between a MET event early in the postoperative course and in-hospital mortality. Our study suggests that of recorded MET triggers, after cardiac arrest, the triggers of staff concern, chest pain, bleeding, hypoxia and hypotension are strongly associated with increased in-hospital mortality. Douglas et al identified hypotension and tachycardia as the commonest triggers for MET calls after surgical procedures and suggested that a clinical assessment in the post-anaesthetic recovery unit may be insufficient to identify patients at high risk of deterioration. 19 A variety of models have been proposed to manage this ‘at-risk’ group. Ludbrook et al offer a strong argument that for medium-risk patients, brief high-acuity care with advanced recovery room care allows enhanced detection and management of early medical emergency response-level complications and increased days at home at 30 days. 20 This is an area we feel will be crucial to explore further in future research.
We emphasise the significance of our study findings in highlighting the associated increased risk of inpatient mortality and prolonged hospital admission for those individuals who trigger a MET event early in their postoperative period. We also feel there is utility in clinicians and carers recognising the associated increased risk of death for all surgical patients with extended postoperative stays. We hypothesise that MET events as a marker for earlier focused intervention with a sustained higher level of observation and care could improve outcomes.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241272107 - Supplemental material for Association of medical emergency team activation in the 24-hour postoperative period with length of stay and in-hospital mortality
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241272107 for Association of medical emergency team activation in the 24-hour postoperative period with length of stay and in-hospital mortality by Tess I Donoghue and Matthew J Brain in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.