
Abstract
Deterioration after major surgery is common, with many patients experiencing a medical emergency team (MET) activation. Understanding the triggers for MET calls may help design interventions to prevent deterioration. We aimed to identify triggers for MET activation in non-cardiac surgical patients. A retrospective cohort study of adult patients who experienced a postoperative MET call at a single tertiary hospital was undertaken. The trigger and timing of each MET call and patient characteristics were collected.
Four hundred and one MET calls occurred after 23,258 surgical procedures, a rate of 1.7% of all non-cardiac surgical procedures, accounting for 11.7% of all MET calls over the study period. Hypotension (41.4%) was the most common trigger, followed by tachycardia (18.5%), altered conscious state (11.0%), hypoxia (10.0%), tachypnoea (5.7%), ‘other’ (5.7%), clinical concern (4.0%), increased work of breathing (1.5%) and bradypnoea (0.7%). Cardiac and/or respiratory arrest triggered 1.2% of MET activations. Eighty-six percent of patients had a single MET call, 10.2% had two, 1.8% had three and one patient (0.3%) had four. The median interval between post-anaesthetic care unit (PACU) discharge and MET call was 14.7 h (95% confidence interval 4.2 to 28.9 h). MET calls resulted in intensive care unit (ICU) admission in 40 patients (10%), while 82% remained on the ward, 4% had a MET call shortly after ICU discharge and returned there, 2% returned to theatre, and 2% went to a high dependency unit.
Hypotension was the most common trigger for MET calls after non-cardiac surgery. Deterioration frequently occurred within 24 h of PACU discharge. Future research should focus on prevention of hypotension and tachycardia after surgery.
Introduction
Complications after major non-cardiac surgery occur in up to 20% of patients. 1 Surgical mortality is only 0.44% during the index hospital admission, but a subgroup of 12.5% of high-risk patients account for more than 80% of deaths. 2 Complications significantly increase the risk of mortality, and have a greater impact than comorbidities or surgical factors. 3 Complications include direct surgical problems such as wound dehiscence, and multifactorial issues such as pulmonary complications, kidney injury, myocardial injury, unplanned intensive care unit (ICU) admission and death. Many of these complications have physiological causes and may be preventable. Management of this risk is variable, including routine ICU admission for high-risk patients, enhanced monitoring in specialised surgical high dependency units (HDUs) or the deployment of medical emergency teams (METs) to rescue deteriorating patients on the surgical ward.4,5 In the event of extreme deterioration (cardiac or respiratory arrest), a ‘Code Blue’ process is activated in our hospital and most other Australian hospitals, 6 using the same mechanism as a MET call. The best approach is controversial, due to resource limitations, 7 mixed evidence of efficacy of ICU admission,8,9 a lack of evidence of efficacy of HDU care, 10 and difficulties triaging patients to avoid overuse of ICU resources. 11 Ward-based care with MET rescue in the event of physiological deterioration is the most common strategy used in Australian hospitals, as MET systems reduce mortality for surgical patients.12,13 However, recent evidence suggested that high-risk patients were more likely to die if their admission to ICU after surgery occurred following a MET call compared with immediate admission to ICU, suggesting that preventing deterioration of physiology was preferable to delayed rescue via MET call.2,14,15 Utilisation of MET systems also varied widely between hospitals. 16
Little is understood regarding the physiological triggers for MET calls after surgery. The criteria in use in most Australian hospitals 6 are displayed in Table 1. Different triggers for activation of MET calls may be more common at different timepoints after discharge from the post-anaesthesia care unit (PACU). 17 In surgical patients selected from mixed cohorts, the commonest triggers were hypotension, hypoxia and tachycardia.18–20 Risk factors for MET calls in surgical patients in previous studies included older age, more extensive comorbidity, living with greater degrees of frailty,21,22 atrial fibrillation, 23 obstructive sleep apnoea (OSA), 24 chronic liver disease, surgical duration, and sedation in PACU. 25 Up to 22% of surgical patients who experience a MET call have more than one activation,26,27 increasing the risk of mortality compared with a single MET call. 28 Without a clear understanding of the incidence and causes of postoperative physiological deterioration it is impossible to prevent such deterioration, and in turn to prevent complications and reduce morbidity and mortality risk to surgical patients. We aimed to investigate the incidence of different physiological triggers for a mixed group of non-cardiac surgical patients who were not planned for ICU admission experiencing MET calls.
Common medical emergency team (MET) trigger criteria.
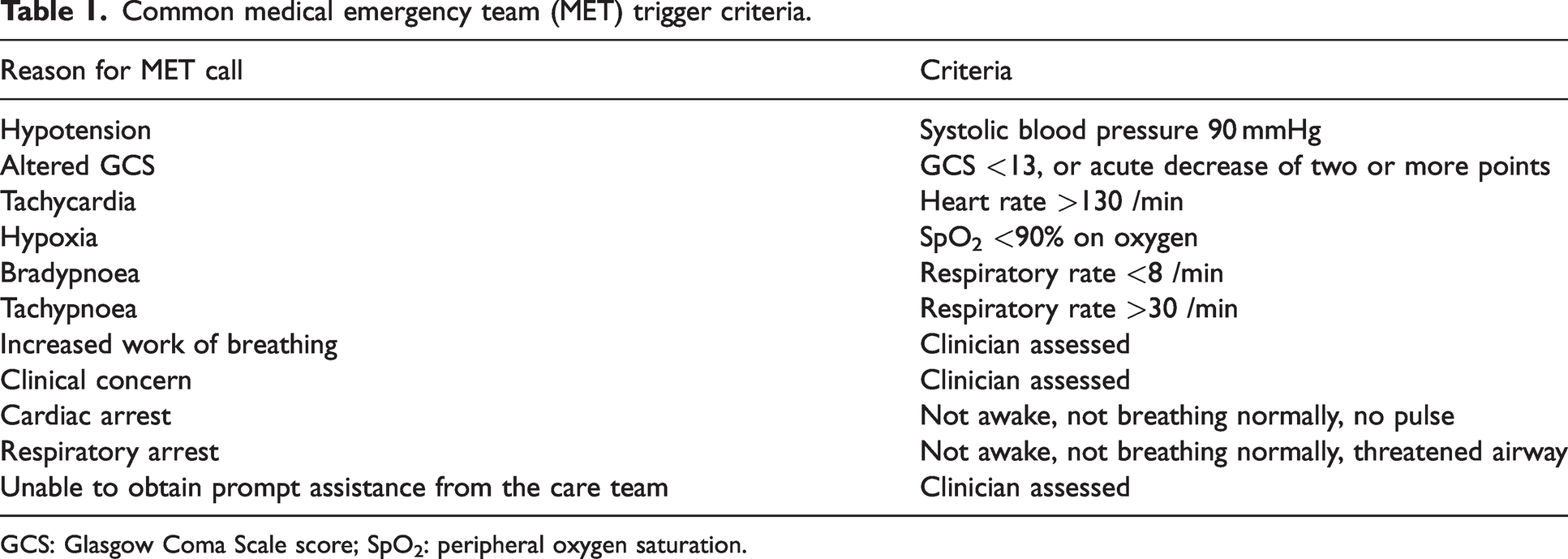
GCS: Glasgow Coma Scale score; SpO2: peripheral oxygen saturation.
Methods
A retrospective single-centre cohort study was performed of all patients who experienced a MET call or Code Blue (resuscitation call) within 48 h of the completion of a surgical procedure, from 1 January 2018 to 31 December 2018 at the Royal Melbourne Hospital, a metropolitan tertiary referral and trauma centre in Australia. The Melbourne Health Human Research Ethics Committee provided ethical approval for the study (QA2019.58). The study was performed in accordance with the Declaration of Helsinki and National Health and Medical Research Council code of practice.
Patients aged under 18 years and those who had non-surgical percutaneous procedures including coronary angiograms, pacemaker insertions or arrhythmia ablations, or endovascular clot retrievals for stroke were then excluded, as the basis for MET call events in these groups were unlikely to be relevant to the surgical population in question (less tissue destruction with concomitant inflammatory response than in patients undergoing surgery). Patients can be transferred to intensive care via three pathways at our institution. The first is directly from the operating theatre, and these patients are usually receiving postoperative mechanical ventilation. The second is via a planned high dependency unit (which is co-located with and managed by intensive care staff) admission pathway, where patients are extubated in theatre, transferred to PACU for a period of time and then transferred to intensive care. The third is after an unexpected deterioration either in PACU or the ward, via a MET call. The study excluded patients in the first two groups and included patients in the third group.
Patients were identified using the hospital’s administrative database. Data were then manually extracted from the hospital’s scanned medical records. Data were extracted by two investigators after training, which included discussion of variable coding and thresholds, example cases and feedback. Regular discussions were held during the extraction process to clarify points of difference. No formal testing of inter-rater reliability was undertaken.
The entry criterion was a MET call after a surgical procedure during the study period. A MET call was defined as an episode of care activated through the MET call system and recorded in the MET call database. The primary outcome was the triggering criterion for the MET call. Triggers for MET calls were pragmatically selected as the triggers in use at the institution, which are consistent with most institutions in Australia. 6 Secondary outcomes included the number of MET calls experienced by a patient in the 48 h after surgery, the destination after the MET call (remaining on the ward, transfer to ICU or another specialised care area, or death) and the time between PACU discharge and the MET call.
We studied a convenience sample of one calendar year of data, anticipating hundreds of relevant MET calls.
The primary and secondary outcomes were presented descriptively. Differences between outcomes between patients with one MET call and patients with more than one MET call were evaluated using Student’s t-tests for normally distributed continuous data and Mann–Whitney U-tests for non-normally distributed continuous data. These analyses were exploratory. Data analysis was undertaken using SPSS (Version 23, IBM Corporation, Armonk, NY, USA). A pre-planned subgroup analysis was performed examining those patients who had repeated MET calls, and for each of the patients who had MET calls for hypotension, tachycardia and hypoxia as triggers for their MET call.
Results
A total of 406 MET calls or resuscitation calls (1.7%) occurred after the 23,258 surgical procedures performed at the hospital in the study year. MET calls in patients who had had surgery within 48 h accounted for 11.7% of the 3455 MET calls in the hospital in the study period. Five records had no data available or an abandoned surgical procedure and were excluded. Analysis was conducted on 401 MET call events, which occurred in 342 individual patients. Comorbidity details are presented in Table 2. American Society of Anesthesiologists Physical Status (ASA PS) classifications and anaesthetic details are presented in Tables 3 and 4 respectively.
Comorbidity status.
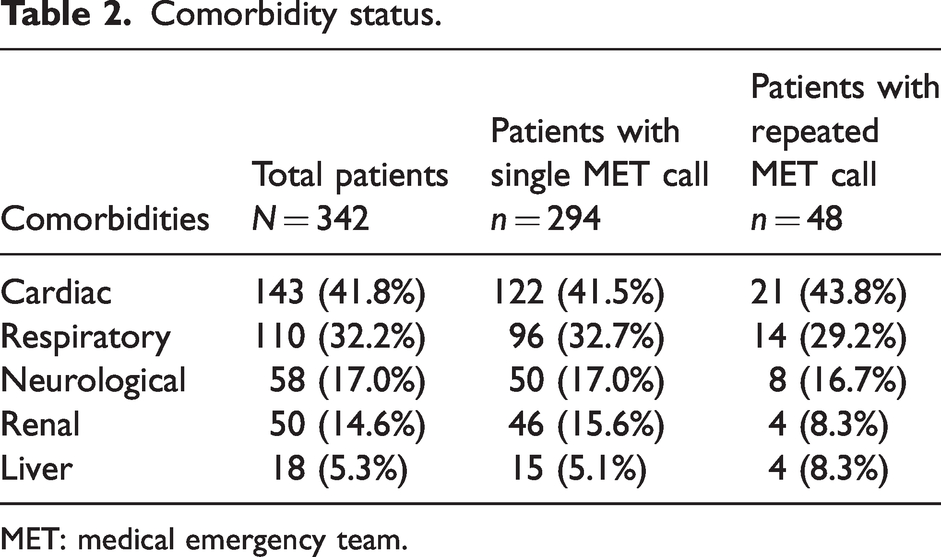
MET: medical emergency team.
American Society of Anesthesiologists Physical Status classification and extent of surgery and medical emergency team calls.
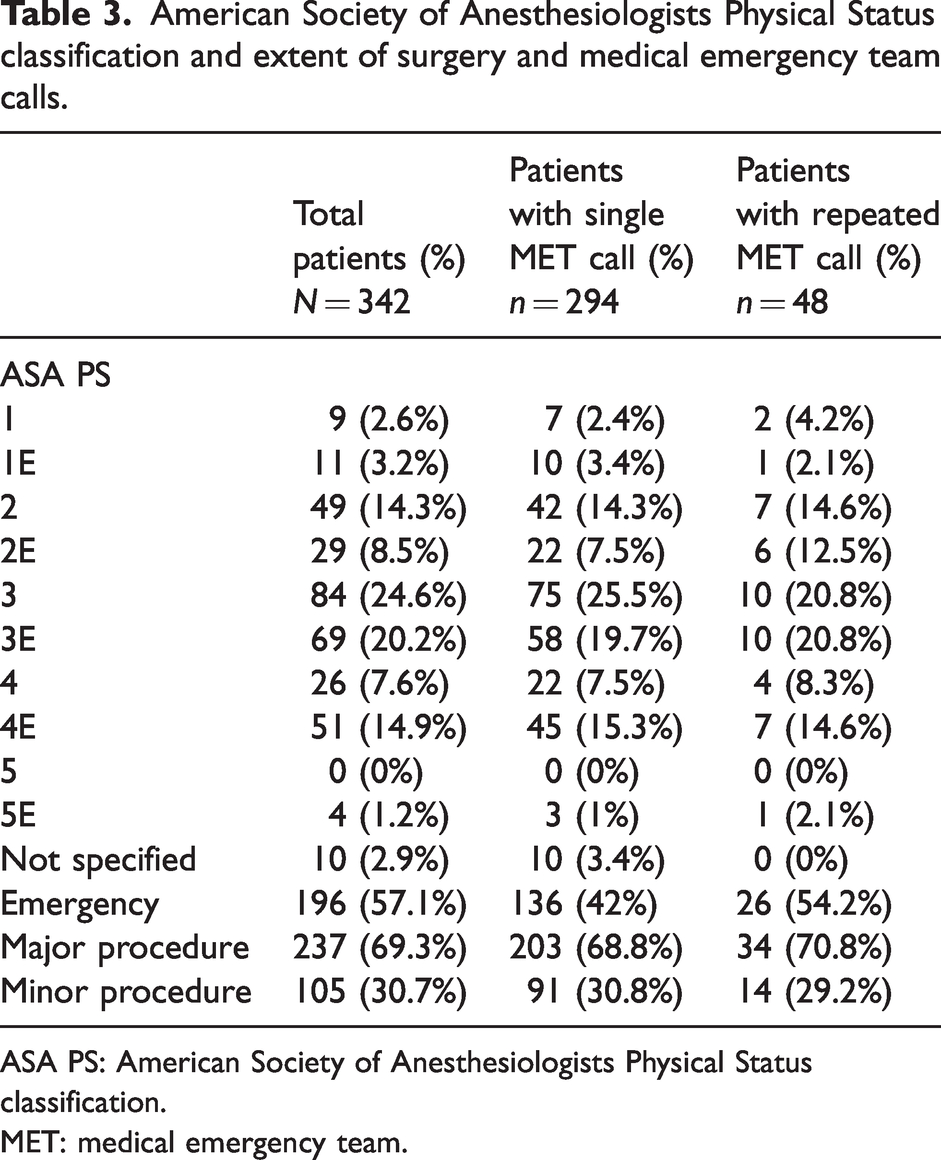
ASA PS: American Society of Anesthesiologists Physical Status classification.
MET: medical emergency team.
Anaesthetic details of patients receiving a medical emergency team call.
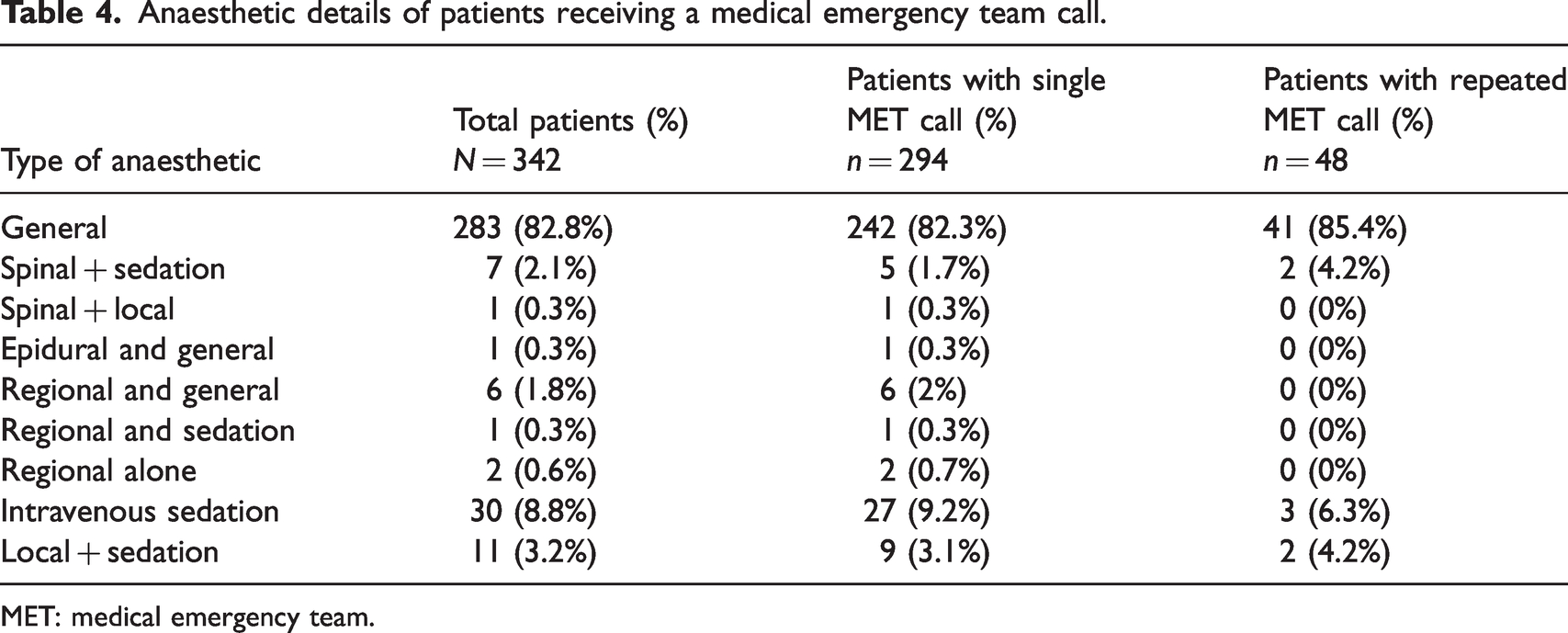
MET: medical emergency team.
Demographics
The median age was 66 (interquartile range (IQR) 25, 16–98) years. Most patients had an ASA PS classification of 3 (24.6%) or 3E (20.2%), and 23.6% had an ASA PS classification of 4 or 5. The most common comorbidities identified in preoperative assessment were cardiac (41.8%), respiratory (32.2%), neurological (17.0%), renal (14.6%) and hepatic (5.3%) disease. The index operation was identified as an emergency case in 57.1% of patients. Ten (2.5%) MET calls occurred in PACU, 16 (4%) on wards immediately following ICU discharge, and the remaining 375 (93.5%) occurred on wards after discharge from PACU.
Primary outcome: trigger for MET call
The most common trigger for a MET call was hypotension (41.4%), followed by tachycardia (18.5%), altered conscious state (11.0%), hypoxia (10.0%), tachypnoea (5.7%), ‘other’ (5.7%), clinical concern (4.0%), increased work of breathing (1.5%), and bradypnoea (0.7%). Cardiac and/or respiratory arrest occurred in five patients (1.4%). Details of triggers are outlined in Table 5.
Triggers of medical emergency team calls.
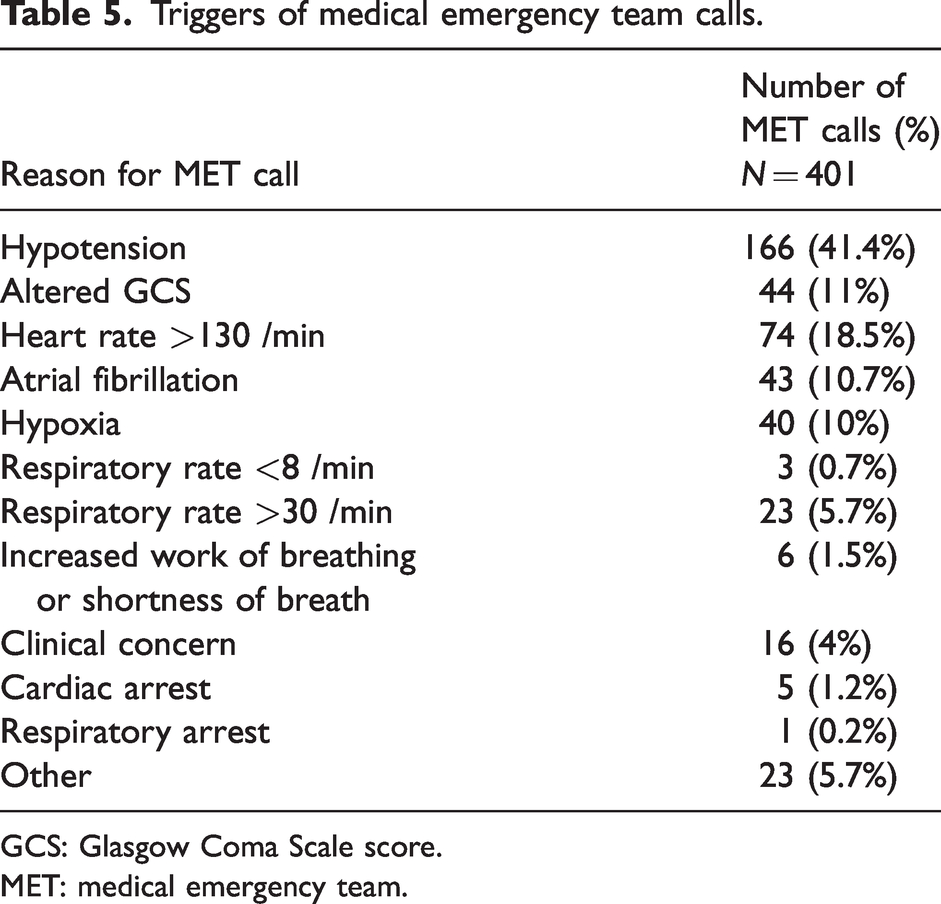
GCS: Glasgow Coma Scale score.
MET: medical emergency team.
Multiple MET calls
In this sample 85% of patients had a single MET call, 13% had two MET calls and 1.5% had three MET calls. One patient (0.3%) had four MET calls. Four patients had a second MET call after an additional procedure within 48 h. The group of 52 patients who had more than one MET call accounted for 15% of the total number of METs. Details are presented in Table 6. The median age of patients with one versus multiple MET calls was 62.9 years versus 63.6 years respectively, P = 0.85. Patients who had multiple MET calls compared with those who had a single MET call were not more likely to have emergency compared with elective surgery (46% versus 52%, P = 0.45), a different ASA PS classification (χ2 = 5.74, P = 0.77), or any type of medical condition (cardiac 33% versus 29%, χ2 = 0.086, P = 0.77; respiratory 32% versus 29%, χ2 = 0.23, P = 0.63; neurological 17% versus 17%, χ2 = 0.003, P = 0.95; renal 15% versus 10%, χ2 = 0.89, P = 0.35; hepatic 5% versus 8%, χ2 = 0.82, P = 0.37). The mean duration of surgical procedure was also not statistically significantly different (124 min versus 148 min, z = –1.7, P = 0.008) and neither was the duration of time the patients spent in PACU (112 min versus 146 min) z = –0.49, P = 0.62) between the groups. Elective surgical patients who had a MET call were more likely to have multiple MET calls than patients having emergency surgery who had a MET call (46% versus 16%, χ2 = 42.9, P < 0.0001).
Number of medical emergency team calls.
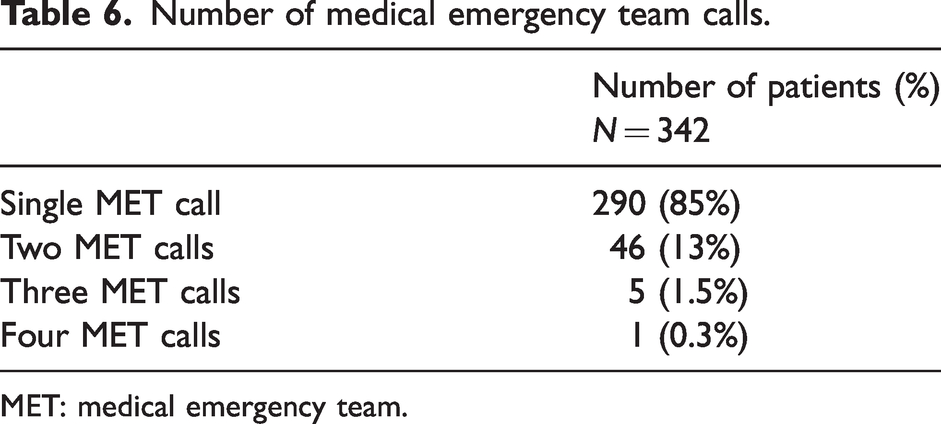
MET: medical emergency team.
MET call destination
A MET call resulted in unplanned ICU admission in 40 patients (10%). Most patients (82%) remained on their ward, 16 (4%) had a MET call shortly after ICU discharge and returned there, seven patients (2%) returned to theatre, four went to an HDU, one patient was transferred to the cardiac catheter laboratory, two died and one was discharged home. The two patients who died were transitioned to palliative supportive care as it was recognised at the MET call that they were dying. In one case, the patient died of cardiac failure after surgery for a fractured neck of femur, and in the other the patient died of septic shock after an emergency gastrointestinal procedure. The patient discharged home following their MET call was a young fit person with significant shivering after minor orthopaedic surgery for whom the nursing staff were unable to obtain prompt assistance from the home team and activated the MET service to obtain support for the patient. The MET team concluded the diagnosis was post-anaesthetic shivering and was prepared to discharge the patient.
Time between PACU discharge and MET call
The median interval between PACU discharge and MET call was 14.7 (95% confidence intervals (CI) 4.2 to 28.9) h. The median interval for MET calls due to hypotension was 8.4 (95% CI 2.7 to 18.0) h, which was significantly shorter than the comparison non-hypotension MET calls (median 18.9 (95% CI 6.45 to 33.9) h (P < 0.001). The interval for the hypoxia MET calls was 16.5 (95% CI 4.2 to 35.7) h, which was not significantly different from the non-hypoxia MET calls (median 14.5 (95% CI 4.1 to 28.1) h, P = 0.66). The median interval for MET calls related to atrial fibrillation was 26.2 (95% CI 10.2 to 38.3) h, which was significantly longer than the MET calls not related to atrial fibrillation 14.1 (95% CI 3.8 to 27.5) h, P = 0.018.
Hypotension
There were 166 (41.4%) MET calls for hypotension (systolic blood pressure <90 mmHg). Twenty (12%) of these occurred in patients who had previously had a MET call for hypotension. A prior history of cardiovascular disease (including hypertension, ischaemic heart disease, arrhythmias, congestive cardiac failure) was identified in 38.0% of patients. Thirty-three percent were taking an angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB), of which 30.3% had taken their ACEI/ARB on day of surgery, while 69.7% had their ACEI/ARB withheld postoperatively.
Hypoxia
There were 40 MET calls for oxygen saturation <90%, with one patient having two MET calls for hypoxia. A history of OSA was noted in 15.0%, while 51.0% were active or ex-smokers, and 30.0% had a diagnosis of chronic obstructive pulmonary disease. Four patients (10%) had a history of asthma, and nine (22%) another respiratory comorbidity.
Tachycardia
Seventy-four MET calls were for heart rate >130 /min with 58.1% of these due to atrial fibrillation. Seven patients had more than one MET call for atrial fibrillation. A beta-blocker was prescribed preoperatively in 31.2% of these patients and digoxin prescribed in 14%. Of those taking a beta-blocker 25% had it withheld postoperatively.
Discussion
Hypotension and tachycardia were the commonest triggers for MET calls in the first 48 h after surgical procedures in this mixed non-cardiac surgical cohort. While the overall frequency of MET calls in this population was 1.7% of all procedures, the burden resulting from deterioration with MET call activation was still a significant challenge for patients recovering from surgery. The dominance of hypotension and tachycardia as triggers for MET calls is consistent with previous work in orthopaedic surgical cohorts.18,19 These observations suggest that future research could focus on identifying predictive factors for hypotension and tachycardia after surgery, and subsequently potential therapeutic interventions to reduce the risk of deterioration. Additionally, while knowing the most likely trigger for a MET call is helpful, the deterioration syndrome of postoperative hypotension, for example, can be caused by a number of underlying pathological processes. Future research should investigate the physiological and pathological drivers of the more common deterioration syndromes, in order that preventive and rescue therapies can be more precisely targeted.
Reassuringly, only 1.7% of MET calls led to ICU admission in this cohort, demonstrating that most patients can be successfully rescued from their physiological deterioration in a ward environment in our hospital. The observation that most MET calls for hypotension occurred in the first 8.4 h after PACU discharge may indicate that the first 8.4 h after PACU discharge represent a high risk period for patients who go on to experience a MET call for hypotension after surgery. This data supports a conservative approach to patients at high risk of postoperative deterioration, including ICU admission where indicated. The data also suggests that clinician assessment in PACU may be insufficient to identify patients at high risk, and alternative strategies are required. The fact that 14% of the included patients experienced repeated MET calls represents an opportunity to identify and select a group of patients who might be better cared for in ICU as opposed to the ward. Further research is required to identify those who are at risk of multiple MET calls, and to identify clinically useful predictors that may assist in developing safer discharge practice from the PACU. There may be separate predictors for each physiological cause of MET calls, and future research should investigate this hypothesis. Specific priority should be given to predictors identifying hypotension and tachycardia given the high proportion of such problems in the study.
Limitations
The study is limited by the fact that it is a retrospective study, and that there was no opportunity to compare the characteristics of the group who had MET calls with those who did not. Without information regarding the group of patients who did not experience a MET call, no conclusion can be drawn regarding the predictive utility of any variable to identify patients who will experience a MET call after surgery. It is also a single-centre study in a tertiary referral and trauma centre, so the results may not be widely generalisable to different institutions. Future studies enrolling patients from multiple centres may produce different results.
Conclusion
MET calls represent severe postoperative deterioration that was rare but important in this single centre study of non-cardiac surgical patients who were discharged to the ward from PACU. The most common triggers of a MET call were hypotension and tachycardia. Few patients died. A small subset of patients experienced repeated MET calls. There is a pressing need to address the causes of hypotension and tachycardia in this patient population to reduce the risk of complications following surgery.
Footnotes
Author Contributions
Acknowledgements
The authors wish to acknowledge Dr Irene Ng and Dr Timothy Fazio for their assistance with the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.