
Abstract
The Complex Decision Pathway (CDP) is a novel perioperative shared decision-making pathway that was established in the Bay of Plenty, New Zealand in 2018. Unique features of the pathway include the use of a structured communication tool to facilitate a goals-of-care conversation in addition to medical assessment, and the use of a tikanga Māori framework for Māori patients. From May 2019 until May 2022, 81 patients attending the CDP clinic were recruited to a prospective study of their demographics, health status and experience at the time of presentation, along with outcomes and opinions over the subsequent 12 months. Participants were mostly elderly and frail with multiple comorbidities, and just over half of participants chose to undergo surgery. Participants who chose, or were recommended, not to undergo surgery were older, more comorbid and had worse outcomes over the subsequent 12 months. Qualitative data suggested an overall positive patient experience of the pathway, and an economic analysis demonstrated its cost-effectiveness. Overall, the data presented here suggested that the CDP assisted in risk-stratifying patients into operative and non-operative groups, provided a positive patient experience, and was a cost-effective intervention.
Keywords
Introduction
Since 2018 the perioperative service at Tauranga Hospital in Bay of Plenty, New Zealand, has been running a shared decision-making service for high-risk patients, the Complex Decision Pathway (CDP). Audit results from the first 18 months of this service, along with a detailed description of the service, were published in 2020. 1 Readers seeking to understand in more detail how the service functions, and how the shared decision-making clinic differs from a standard preassessment clinic, are referred to this publication. In May 2019 we commenced a prospective observational study to better understand the outcomes and experiences of patients presenting to the pathway.
Pathway development was iterative in the years after inception but culminated in the process described in our previous publication. 1 Novel and key features of the pathway include the use of a structured communication tool to facilitate goals-of-care conversations (Aotearoa Serious Illness Conversation Guide (SICG), adapted with consumers in New Zealand, August 2018 2 ), as well as a tikanga Māori framework for appointments with Māori patients.
The purpose of this study was to gain a better understanding of our patients and their experiences of a pathway using these novel approaches, and to explore their outcomes over the subsequent 12 months. We also sought to understand how participants felt about the process and the decisions they made over the subsequent 12 months. As part of understanding the economic sustainability of our shared decision-making pathway, we also undertook an economic analysis based on the collected data and present these results here.
Methods
Study design and questions
This study received ethics approval from the Central Health and Disability Ethics Committee, reference number 19/CEN/53, and locality approval from the Bay of Plenty Clinical School, reference number 2019-16.
Patients presenting to the CDP shared decision-making clinic between May 2019 and May 2022, were invited to participate by a nurse on arrival for their appointment. All patients were eligible to participate except for those requiring a proxy decision-maker, that is, patients known to be not competent to provide informed consent for surgery. Patients wishing to participate completed a consent form containing detailed information about the study.
Initially we had planned to enrol participants for 5 years and conduct the analyses after the first year of follow-up, and at the completion of the study. However, the COVID-19 pandemic severely reduced the numbers of patients able to access the service during 2020 and 2021, and resulted in substantial increases in COVID-19-related workload for the research clinicians. As such, a decision was made to cease enrolling participants after 3 years, and to conduct a single analysis once their follow-up was complete.
Following enrolment, participants were asked to complete a health-related quality of life questionnaire (EuroQol 5 Dimension 5 Level; EQ5D5L) 3 prior to their appointment, and to complete a patient experience questionnaire immediately following their appointment. The patient experience questionnaire asked patients to answer questions about their experience of the conversation they had with the doctors using a combination of 4-, 5- and 7-point Likert scales. Questions were designed to explore the extent to which participants felt their understanding of their future health, their sense of control over medical decisions, and hopefulness about their future quality of life, had increased or decreased as a result of the conversation (7-point Likert scales). They were asked to report how worthwhile they felt the conversation was (4-point Likert scale), and the extent to which they felt heard and understood (5-point Likert scale). These questions were provided to us by Associate Professor Rachelle Bernacki. The questions were created by a group of experts for use in researching patient experiences of conversations using the SICG in non-perioperative settings.4,5 Participants were additionally asked to give written feedback in response to the open question ‘How did you feel about the conversation you had today?’
Demographic and health-related data were collected from participants’ electronic health records at the time of appointment and at 6 and 12 months following this appointment. Risk scores were taken from the documentation created at the CDP appointment by the assessing clinicians.
Participants were phoned at 6 and 12 months after presentation and asked to complete the telephone version of the EQ5D5L; all participants were asked two additional questions, and those who had undergone surgery were asked three questions:
How do you feel about the decision that was made about the surgery? *What goals were you hoping to achieve by having surgery and were these goals achieved? Do you have any other comments about your experience of the decision-making pathway you participated in?
*Only participants who had undergone surgery
These questions were generated by our research team and designed to assess the stability of patient views over time, along with their views on goal achievement.
Quantitative analysis
For demographic, health-related quality of life score, and outcome data, descriptive analysis was used. The Likert scale data was also analysed using descriptive analysis and frequency counts of responses in each category.
Two participant groups were identified based on the decisions participants made via the CDP, the group that chose to have surgery (the Yes group) and a group that chose, or were recommended, not to have surgery (the No group). The Yes group and No group were compared with respect to age, sex, ethnicity, American Society of Anesthesiologists Physical Status Classification (ASA PS), 6 surgical indication and mortality outcomes.
Due to low numbers of participants undergoing surgery during the study period and a much lower follow-up rate in the No group, we elected not to further analyse EQ5D5L data at 6 and 12 months.
For the calculation of p-values, the Student’s t-test (one-tailed) was used for continuous data and Fisher’s exact test was used for categorical data.
Qualitative analysis
Free text comments written at the time of the initial appointment, and verbal comments recorded and transcribed from the open-ended question asked over the telephone at 6 and 12 months, were analysed using an inductive thematic analysis following the six-step process outlined by Clarke and Braun, 7 and described in relation to anaesthesia research by Jowsey et al. 8 Two authors (HO and RF) independently coded the data in Excel (Microsoft, Redmond, WA, USA) using open coding. They then met in person to compare codes and identify themes into which the codes were grouped. Both authors then recoded the data, refining themes as needed via an iterative process. Any disagreements were resolved by consensus.
Deductive thematic analysis was used to analyse the answers to two of the questions asked at 6 and 12 months, specifically looking at stability of patient views and goal achievement. Answers to the question ‘How do you feel about the decision that was made about surgery?’ were coded according to the following predetermined themes: satisfied, resigned, ambivalent, or regretful. Answers to whether surgery-related goals were achieved were coded to the predetermined themes of achieved, partially achieved, not achieved, or unsure. Where patients were unable to remember the appointment, the proposed operation or were otherwise unable to answer the question this was coded as ‘Can’t Answer’. Frequency counts were applied to these coded comments.
Economic analysis
An economic analysis was performed by one of the authors (TR), using fully absorbed costing data from the Hauora a Toi Bay of Plenty data warehouse. An estimated cost of providing the CDP to all study participants was compared with an estimate of the avoided cost of operative care for the patients in the No group. The CDP cost estimate was made using 2022–2023 data and covered costs related to the shared decision-making clinic appointment only. Costs incurred as part of a standard surgical assessment and preassessment process were excluded. The cost estimate of avoided surgery was derived from assessing the actual average costs of providing the proposed operations to other high-risk Bay of Plenty patients over the age of 65 years between 2020 and 2023. Where sufficient numbers of comparable patients were available, recent data was used preferentially (2022–2023). Where lower numbers of comparable patients were available earlier data was used (2020–2023), or data from lower risk patients. These estimates included the cost of the avoided operation and inpatient care, as well as standard postoperative surgical follow-up, but excluded rehabilitation facility costs and postoperative community care costs.
Results
Quantitative results
Between May 2019 and May 2022, 107 patients presented to the CDP shared decision-making clinic. Five patients were excluded from this study as they required proxy decision-makers. Of the 102 patients eligible to participate, 21 declined, response rate 79%. Twenty-one participants in this prospective study overlapped with and were included in our previously published audit data. 1 Surveys were completed on the same day following the clinic appointment.
The age, sex, ethnicity, ASA PS, Clinical Frailty Scale 9 , and the American College of Surgeons National Surgical Quality Improvement Programme (NSQIP)10,11 surgical risk calculator–predicted 30-day mortality scores of the participants are given in Table 1.
Demographic data and risk scores.
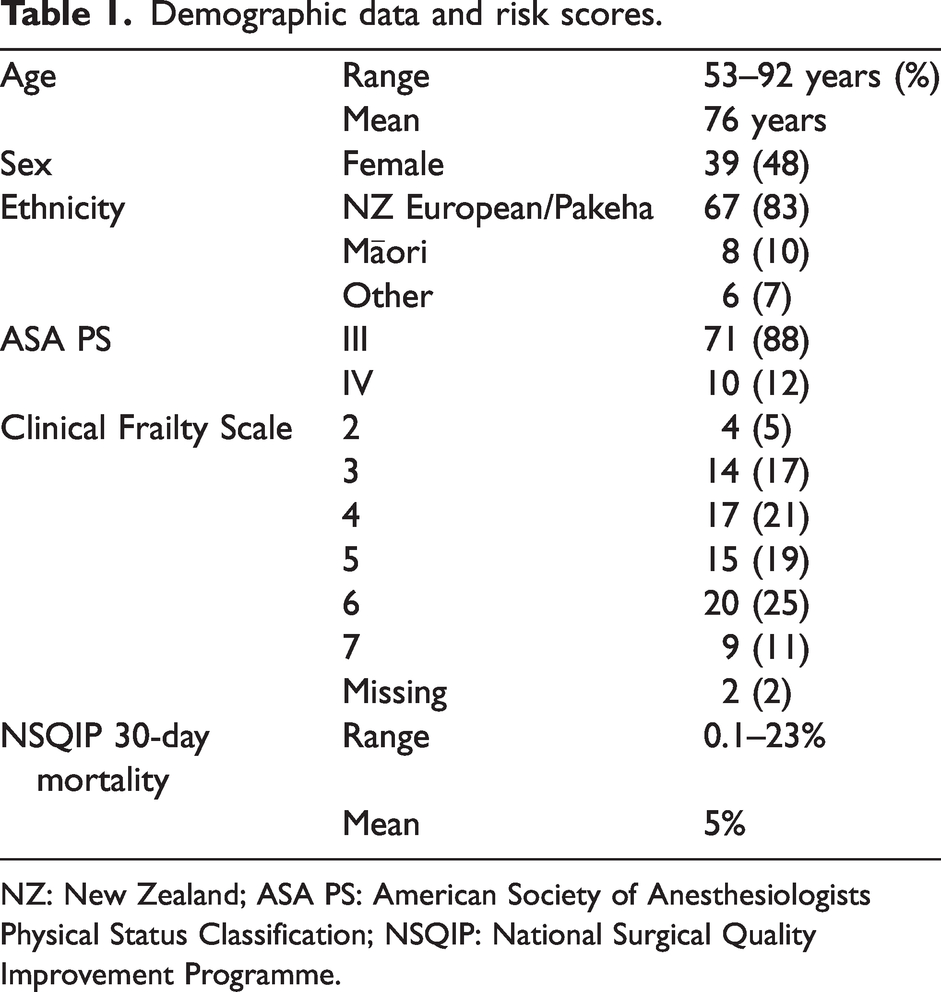
NZ: New Zealand; ASA PS: American Society of Anesthesiologists Physical Status Classification; NSQIP: National Surgical Quality Improvement Programme.
Patients were referred from a range of surgical specialties but predominantly orthopaedic surgery (51 (63%)) and general surgery (22 (27%)). The most common indication for surgery was pain (45 (56%)), with 18 (22%) patients having cancer as the indication for surgery.
Baseline patient responses to the EQ5D5L health-related quality of life questionnaire are presented in Tables 2 and 3. Data on patient comorbidities is listed in Table 4.
Baseline EQ5D5L responses.
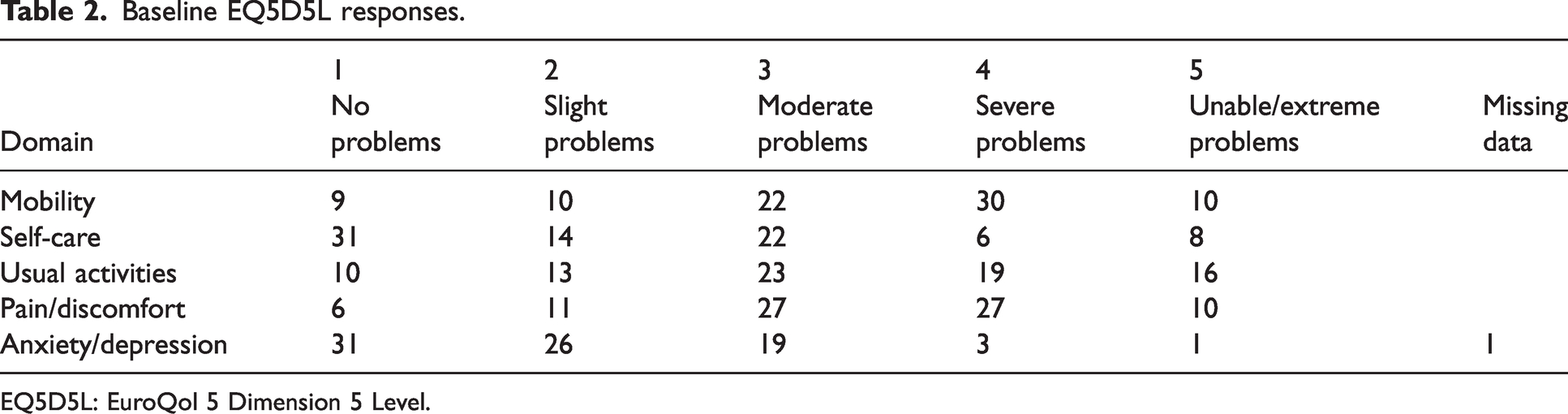
EQ5D5L: EuroQol 5 Dimension 5 Level.
Baseline EQ5D5L visual analogue scale responses.
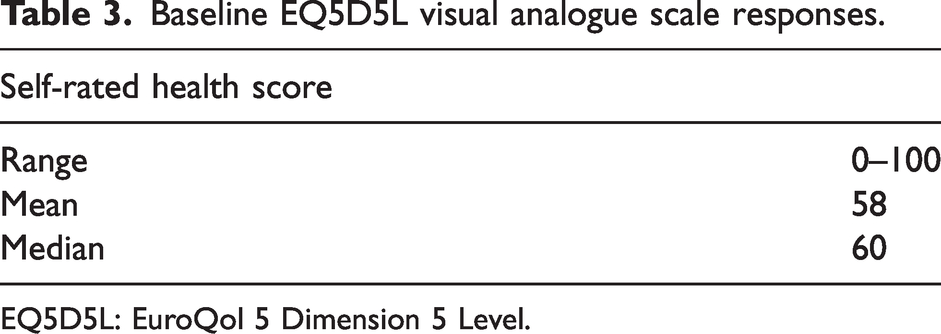
EQ5D5L: EuroQol 5 Dimension 5 Level.
Comorbidities.
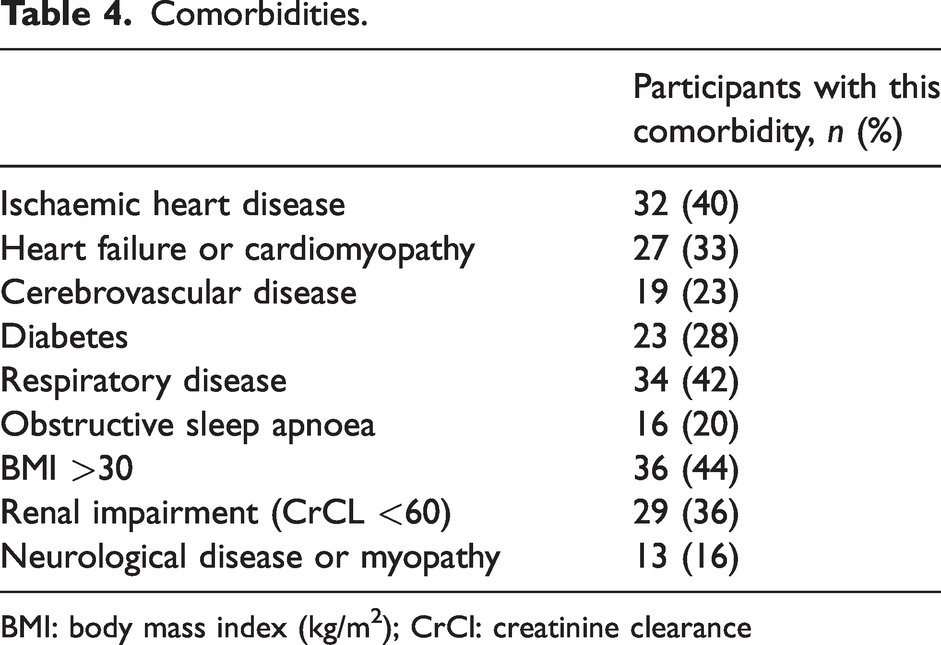
BMI: body mass index (kg/m2); CrCl: creatinine clearance
Forty-two (52%) patients chose to undergo surgery (Yes group), and 39 (48%) chose, or were recommended, not to undergo surgery (No group). Final decisions were often made some time after the shared decision-making clinic appointment, allowing time for reflection and discussion with family members and the referring surgeon. Comparison results for the Yes and No groups are summarised in Table 5. When compared with the Yes group, the No group participants were significantly older (78.2 years versus 73.5 years, P = 0.006), and significantly more likely to be ASA PS IV (9/39 (23%) versus 1/42 (2%), P = 0.006). Women were significantly over-represented in the Yes group (females 27/42 (64%) versus males 15/42 (36%), P = 0.04). Māori participants were equally represented in the Yes group (4/42 (10%)) and No group (4/39 (10%)), P = 1.0. Participants with cancer as the indication for surgery were equally represented in the Yes group (9/42 (21%)) and No group (9/39 (23%)), P = 1.0.
Comparison of Yes and No group characteristics.
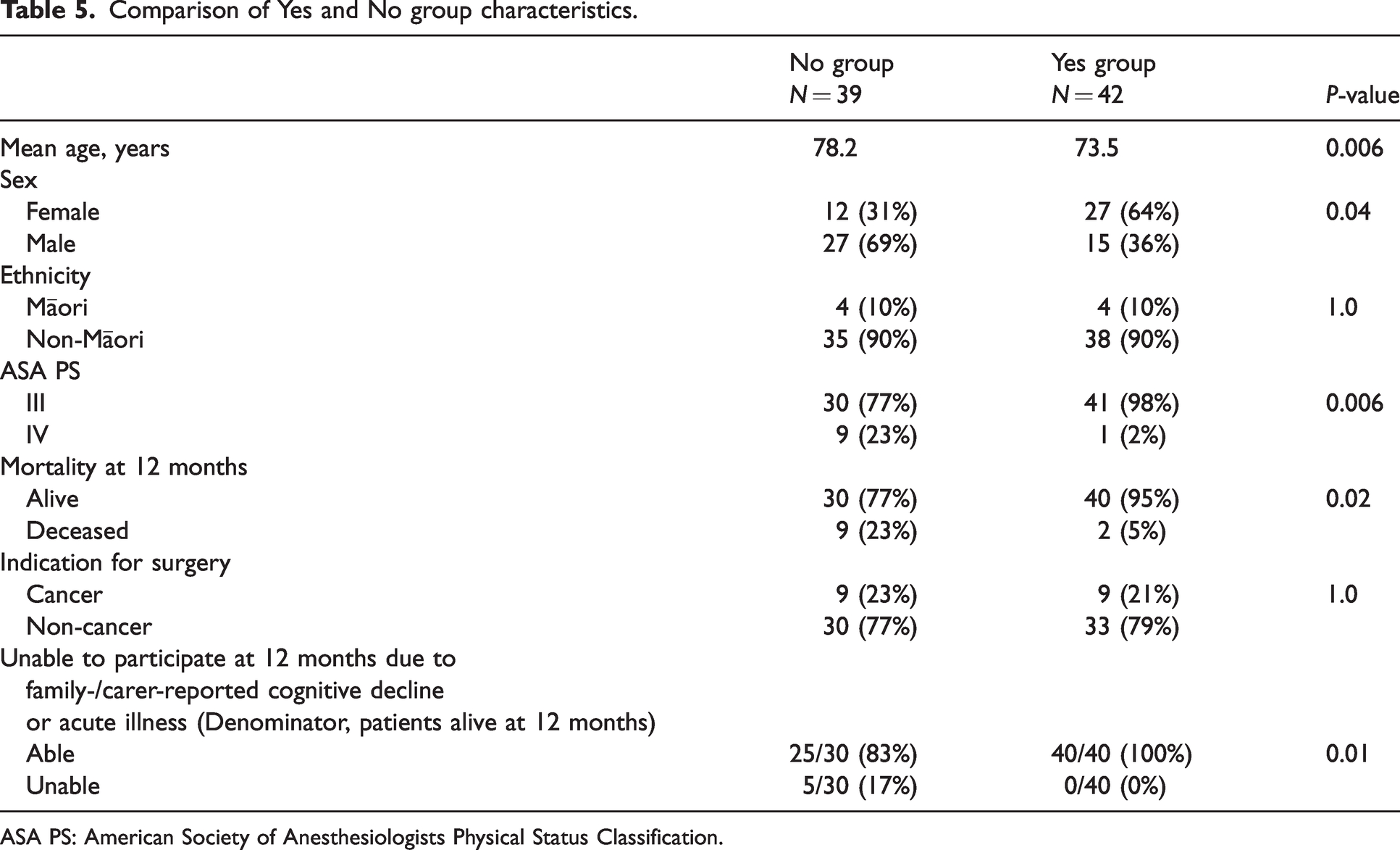
ASA PS: American Society of Anesthesiologists Physical Status Classification.
Participants in the No group had a significantly higher mortality at 12 months (9/39 (23%)), compared with the Yes group (2/42 (5%)), P = 0.02. Deaths in the No group were analysed to assess whether the surgical pathology was related to the cause of death. In six out of the nine cases we could be certain that deaths were unrelated to the surgical pathology; in three cases it was possible that surgical pathology (cancer) may have contributed to the cause of death. Both deaths in the Yes group were in patients who had undergone surgery, but not within 30 days (116- and 253-days post-surgery). Of the participants remaining alive at 12 months, participants in the No group were significantly more likely to have family- or carer-reported cognitive decline, or to be suffering from an acute illness, such that they were no longer able to participate in a telephone interview at 12 months (5/30 (17%) versus 0/40 (0%), P = 0.01).
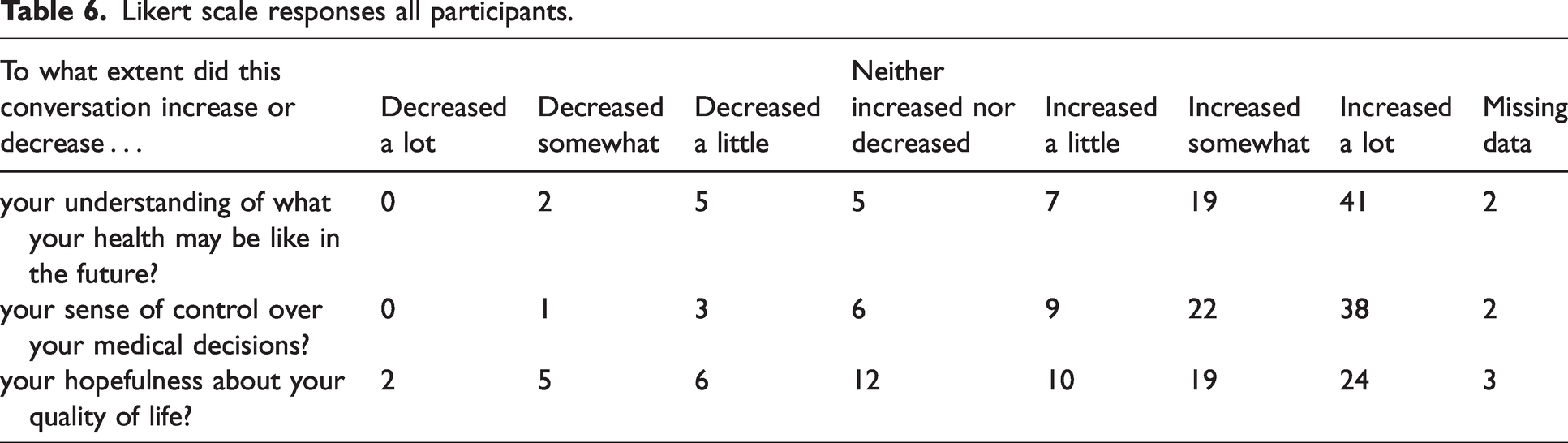
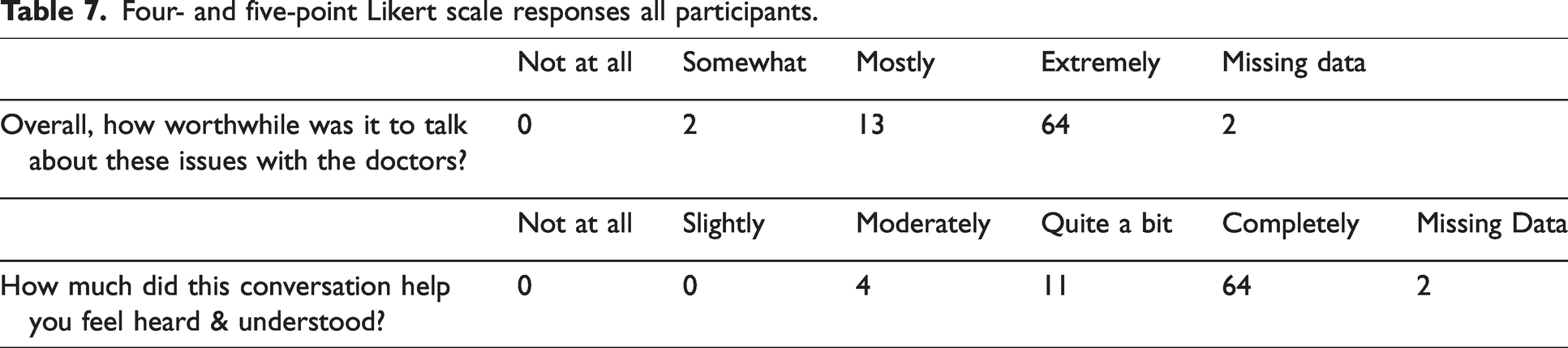
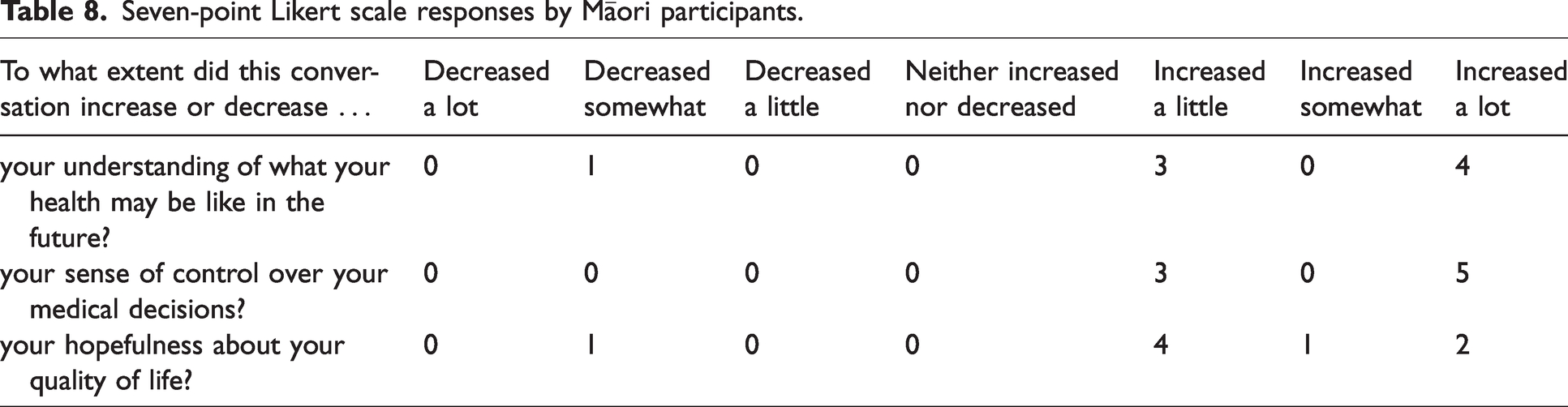
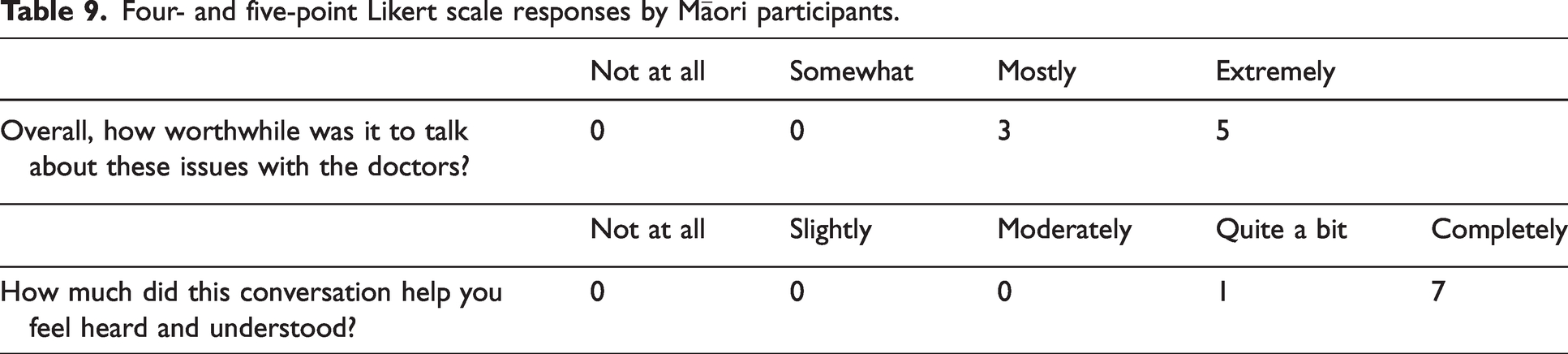
Likert scale responses from all participants are listed in Tables 6 and 7. Subanalyses of Likert-scale responses from Māori patients are listed in Tables 8 and 9.
Likert scale responses all participants.
Four- and five-point Likert scale responses all participants.
Seven-point Likert scale responses by Māori participants.
Four- and five-point Likert scale responses by Māori participants.
Qualitative results
Of the 81 survey respondents, 60 (74%) responded to the free text question ‘How did you feel about the conversation you had today?’. Thematic analysis of the initial written comments identified seven themes, and these are presented in Table 10, with exemplars for each theme. The seven themes are feeling informed, effective communication, feeling more confident or empowered, worthwhile conversation, grateful, positive comments about the process or staff, and describing a positive emotional state. Of these, two themes dominated across responses: feeling informed, and finding the communication to be effective. Several patients covered multiple themes in their responses. Participants were numbered at recruitment and this number is indicated in parentheses after their comment.
Thematic analysis of participant survey responses.
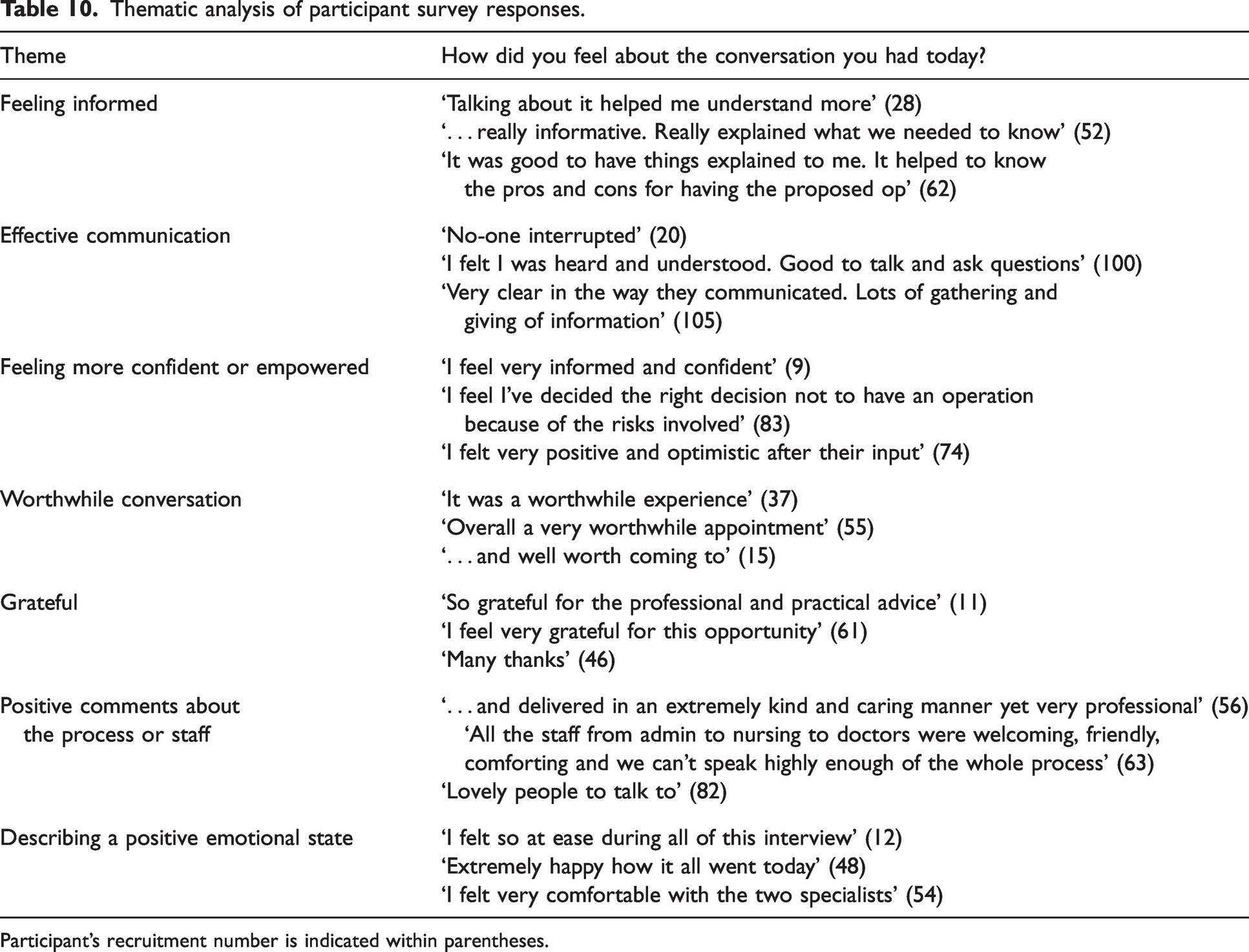
Participant’s recruitment number is indicated within parentheses.
Initial written comments were specifically searched for any information that might reflect poor/negative patient experiences, and we identified three such statements. The statements were unrelated and are reported here individually in turn. One respondent expressed that they should have come to the clinic sooner (re-routed to CDP after operation cancelled by anaesthetist). One respondent found it difficult to hear at times (earthquake-strengthening works were occurring that day). A final respondent expressed some surprise at the nature of the clinic appointment.
Response rates to the follow-up phone interviews at 6 and 12 months differed between the Yes and No groups. The response rate in the Yes group was 41/42 (98%) at 6 months (one participant was unable to be contacted due to acute illness) and 40/42 (95%) at 12 months (two participants deceased). The response rate in the No group was 29/39 (74%) at 6 months (one was not contactable, three deceased, four participants’ family/carers reported they were cognitively incapable, two acute illness) and 22/39 (56%) at 12 months (one not contactable, one declined, nine deceased, four participants’ family/carers reported they were cognitively incapable, one acute illness, one unable to use telephone due to new hearing loss). At the time of the 6-month follow-up 18 (43%) participants in the Yes group had undergone surgery, and at the 12-month follow-up, 26 (62%) participants in the Yes group had undergone surgery.
The results of the thematic analysis of responses to the question asking how participants felt about the decision at 6 and 12 months are presented in Figures 1 and 2, respectively. The theme of satisfaction was dominant in the Yes group: 35/41 (85%) at 6 months and 32/40 (80%) at 12 months. The theme of satisfaction was also seen in the No group: 11/29 (38%) at 6 months and 9/22 (41%) at 12 months. The theme of resignation was seen in the No group at 6 months, 11/29 (38%), and at 12 months, 6/22 (27%). The theme of ambivalence existed in small numbers in both groups at 6 months, 3/29 (10%) in the No group and 4/41 (10%) in the Yes group, and again at 12 months 2/22 (9%) in the No group and 3/40 (8%) in the Yes group. The theme of regret was seen only in the No group, 1/29 (3%) at 6 months (indication for surgery, pain), and 3/22 (14%) at 12 months (indications for surgery, pain (2) and poor mobility (1)).
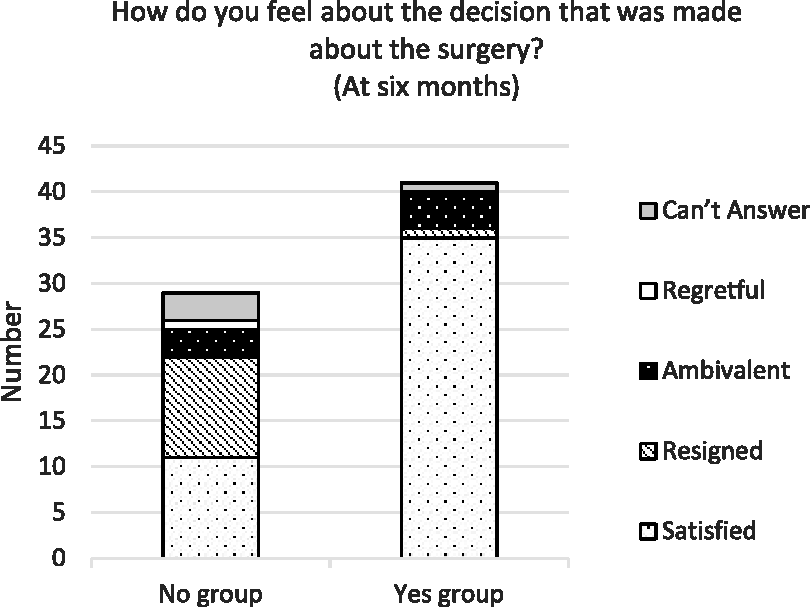
Feelings about decision at 6 months.
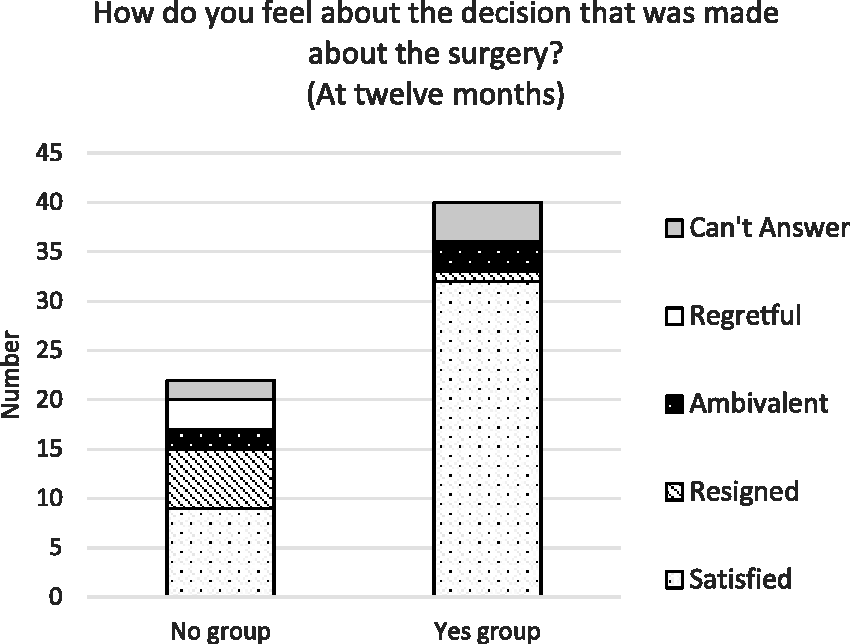
Feelings about decision at 12 months.
Patients who had undergone surgery at 6 and 12 months were asked whether their goals related to the surgery had been achieved; the thematic analysis applied to these responses is presented in Figure 3. All 18 participants who had undergone surgery at 6 months were contactable and were asked this question. Of the 26 participants who had undergone surgery at 12 months, two patients were deceased, and the question was omitted for one patient (interviewer error), giving a response rate of 88%. The theme of goals being achieved was seen in 9/18 (50%) of participants at 6 months, and 13/23 (57%) of participants at 12 months.
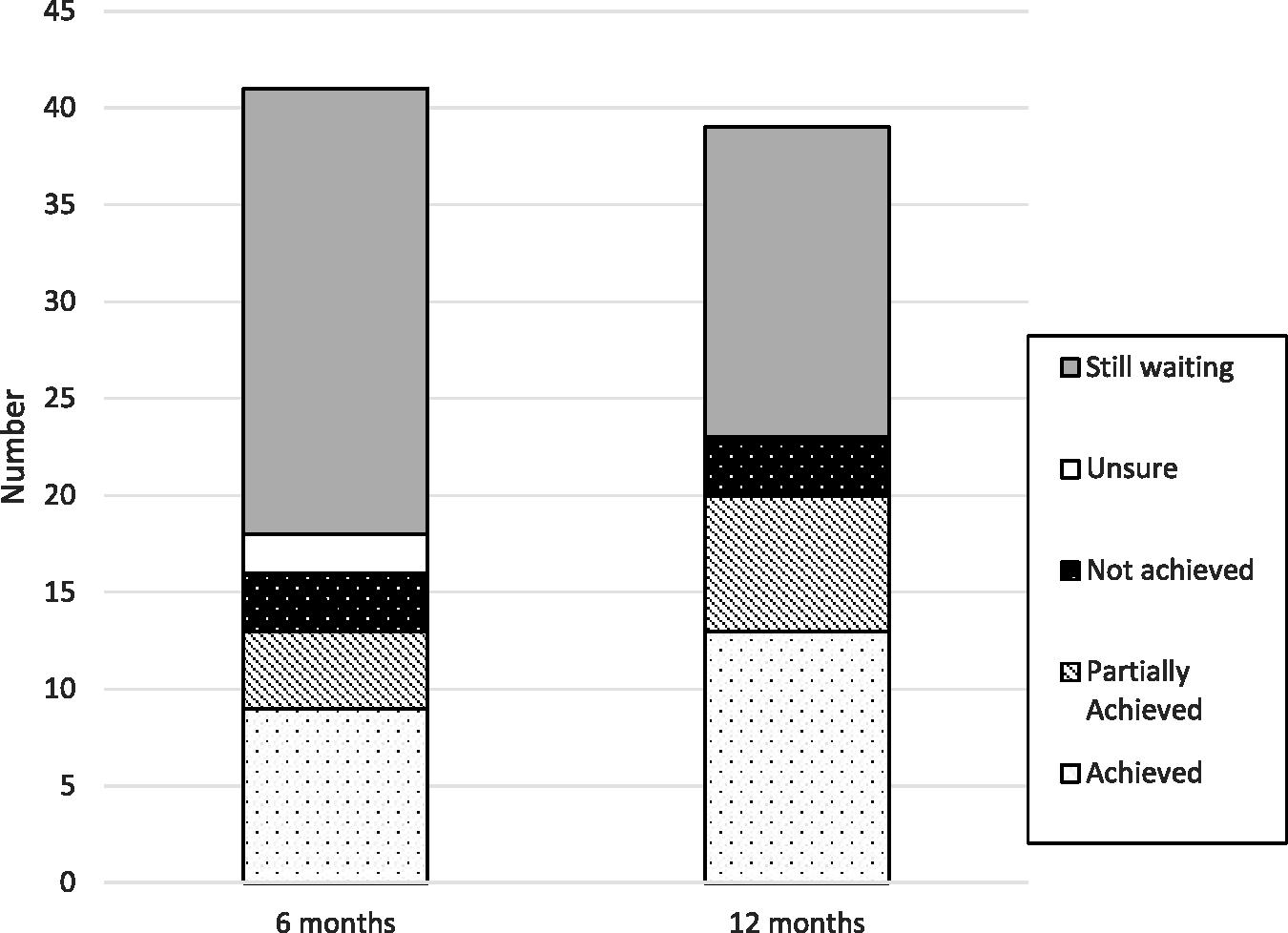
Were goals achieved with surgery?
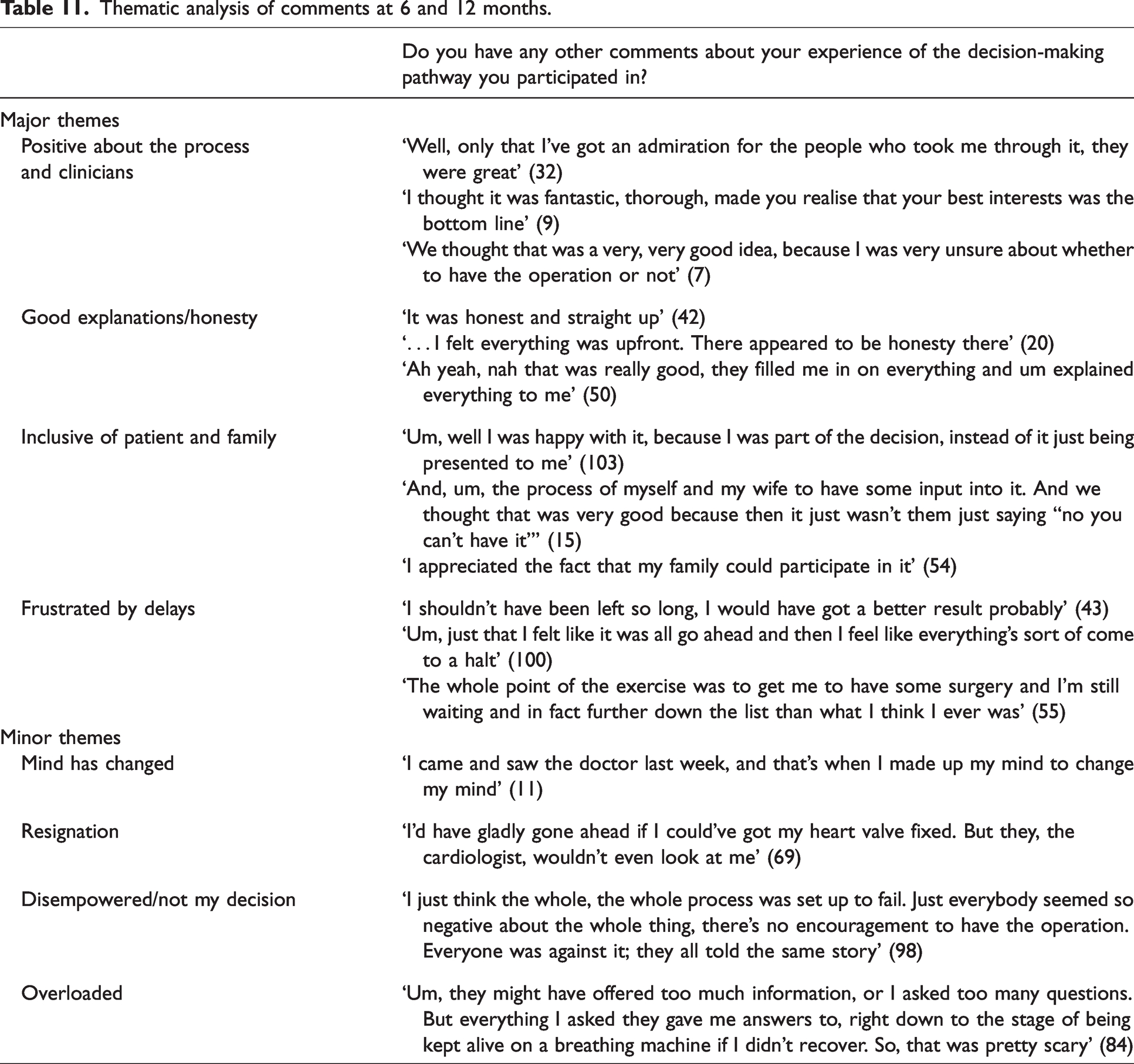
A number of patients had no further comments to make about their experience of the decision-making pathway when offered the opportunity to provide open feedback at 6 and 12 months. A smaller number of patients talked about other aspects of their healthcare not relevant to the pathway, and where this occurred these comments were excluded from the analysis. Thematic analysis of the remaining relevant responses from 51 patients at 6 months (63%) and 40 patients at 12 months (49%) identified four major and four minor themes (responses numbering fewer than five were coded to minor themes) and these are presented in Table 11. Some patients covered more than one theme in their response. Three out of the four major themes were present in both the Yes and the No groups, but the theme of frustration with delay in accessing surgery was seen only in the Yes group. The minor themes of resignation and feeling disempowered were seen in both the Yes and No groups, but the theme of changed mind was only seen in the No group, and the theme of feeling overloaded with information or the process was only seen in the Yes group.
Thematic analysis of comments at 6 and 12 months.
Economic results
The estimated cost of providing the CDP to each participant (above the standard preassessment process) was NZ$1518, giving a total cost of CDP participation for our study participants of NZ$122,958. The total estimated cost of providing the 39 operations in the No group that were considered but ultimately decided against was NZ$1,260,727. Costs differed depending on the operation type, but an average cost of NZ$32,326 per operation avoided was calculated from the above estimate. The annual cost of running our service was estimated to be approximately NZ$66,792 based on the per patient estimate above, and our experience of running 22 clinics per year, catering to 44 patients (i.e. in years not affected by COVID-19 lockdowns).
Discussion
Background information on the development and structure of our shared decision-making pathway, and the importance of shared decision-making in perioperative services, can be found in our previously published work. 1 The role of shared decision-making in perioperative services is increasingly well understood, and forms a key component of the Australian and New Zealand College of Anaesthetists (ANZCA) Perioperative Care Framework. 12
Our shared decision-making pathway, the CDP, was utilised by a group of patients who were predominantly elderly, frail, functionally impaired, and comorbid, with a high mortality rate in the year following their participation in the pathway. Just over half the participants in this study chose to undergo surgery, consistent with our previously published audit findings. 1 The data presented here shows that as participants progressed through the pathway, they were risk stratified into an older, higher risk group of participants who chose, or were advised, not to undergo surgery (No group). This risk stratification was evident in the significantly worse outcomes for the No group over the subsequent 12 months. These adverse outcomes most likely reflected the baseline characteristics of this group rather than the decision not to undergo surgery.
Attending the CDP clinic appeared to be beneficial to participants. As a result of the clinic conversation, the majority saw an increase in their understanding of their future health, their sense of control over medical decisions, and hopefulness about what their health may be like in the future. At these appointments patients and clinicians necessarily discuss a lot of medical information, and as such it is a positive finding that participants did not report feeling confused, and predominantly rated their understanding as increased, a finding that was reinforced by the open feedback. It was also a positive finding that the majority of participants felt a greater sense of control over their medical decisions and hopefulness about their future quality of life. The latter is a somewhat surprising finding given that many of the discussions are likely to revolve around the idea that an operation is not an easy solution to the problem they are experiencing and may be very high risk and/or may sometimes not be in their best interests. Paladino et al. 4 have previously demonstrated the feasibility and acceptability of the SICG as a tool for use in oncology practice, with positive experiences for patients and clinicians. They hypothesise in their discussion that the person-centred focus of the SICG with an emphasis on what is important to the patient may protect against psychological distress in discussing end-of-life care. It is possible that the use of this structured communication tool in our clinic, and the resultant patient-centred discussion, is also protective for our participants when discussing the potential adverse risk–benefit balance of an operation, allowing increases in many participants’ sense of control and hopefulness, despite facing a difficult decision.
All participants rated the conversation as worthwhile, and all reported that they felt heard and understood to some extent, with 79% of participants feeling ‘completely’ heard and understood, suggesting that the process adds value for participants. Thematic analysis of the general comments provided at the time of the clinic appointment reinforced these findings, with themes of feeling informed and experiencing effective communication particularly evident. In developing the CDP, early input from our Māori Health Gains and Development team was sought, and co-design of the service has resulted in Māori patients being offered a shared decision-making clinic appointment that utilises a tikanga Māori framework. This includes a different location for the appointment, along with cultural liaison support, and an appointment structure that follows the Hui process. 13 Subanalysis of the Likert scale data offered reassurance that the feedback was also predominantly positive from our Māori participants, although these results should be interpreted with caution due to the small number of responses.
Follow-up was limited in the No group at 6 and 12 months due to a high incidence of adverse outcomes. The data available at 6 and 12 months suggests decisional regret was an uncommon theme overall. The theme of regret was seen only in the No group, predominantly at 12 months, in participants with pain or poor mobility as their primary indication for surgery. This finding reflects the importance of integrating reassessment as a crucial part of the pathway when required, and providing robust alternatives to surgical intervention, such as assessment and advice from other services, for example, pain specialists and occupational therapists, where possible. Although not demonstrated in participants during the study period, the authors are aware that reassessment of patients has occurred in our service, albeit rarely.
Participants in the Yes group expressed high levels of satisfaction with their decision at 6 and 12 months, but only just over half felt that they had achieved their surgical goals when surveyed postoperatively. This finding may reflect an inadequate period of recovery before the question was asked, however, we postulate that it may also reflect the difficulty participants experience in meeting their high expectations of postoperative function when they are elderly, frail and have multiple other comorbidities to begin with.
The COVID-19 pandemic had an unexpected and negative impact on our study. A major limitation was that participants experienced lengthy delays in accessing surgery, which at the time of our study was a nationwide phenomenon. 14 At the end of 1 year of follow-up only 62% of the Yes group had undergone surgery, and a third of these within the previous 6 months. As such, we are not able to comment meaningfully on 1-year postoperative outcomes for this group. It is unsurprising to the authors that frustration with delay in accessing surgery emerged as a theme, particularly at 12 months. Two of the authors (HO and RF) have experience in triaging for the pathway, and it is evident that being referred to the CDP does not in itself cause significant delays. Wait times for CDP appointments are minimal, the pathway often results in a more streamlined assessment process (with early specialist input) and we have an agreement with the surgeons that patients who have been through the CDP and decided to proceed will be expedited to surgery whenever possible. The authors are aware however that delay in accessing surgery is exaggerated for this patient group. Many of these patients require postoperative high dependency unit care, and almost without exception are unsuitable for outsourcing to the private sector, which is a key strategy in reducing elective surgery waiting times in our region. 14
The economic analysis demonstrated that the estimated cost of surgery avoided by the No group dwarfed the estimated cost of providing the CDP to all participants, by a factor of 10. Not all the participants in the No group would have proceeded to have an operation in the absence of the CDP. It is very likely that the referring surgeons, or our traditional preassessment pathway, would have sometimes encouraged reconsideration of surgery in similar patients prior to the inception of the CDP. Without a direct comparison with standard care, it is not possible to know how many more patients avoided having an operation as a result of participating in the CDP. However, it was a shared concern that our traditional preassessment model did not always offer our highest-risk patients the opportunity to make carefully considered, value-congruent decisions which led to the development of the CDP, and we do believe that the service has resulted in more patients appropriately choosing not have surgery. The economic analysis necessarily includes numerous assumptions and is indicative only. We believe that by deriving the cost estimate of avoided surgery from actual costs of the same operations in elderly, comorbid patients we have made a conservative estimate, as the participants in the No group are likely to have had an even higher risk of perioperative complications than patients who actually underwent surgery. Regardless, the analysis demonstrated that the pathway costs were so small compared to the cost of major surgery in elderly, frail, and comorbid patients that on average avoiding two to three operations per year would result in the pathway achieving cost neutrality at our institution. Avoiding surgery is not the purpose of the CDP; the purpose is for patients and clinicians to share in decision-making so that the resultant decisions are informed, wise and value-congruent, and to achieve the best possible outcomes for our patients. The economic analysis of our study data suggests that the pathway has been an economically sustainable addition to our service.
The combined quantitative, qualitative and economic analysis presented here suggests that the CDP may help to contribute to the Institute for Healthcare Improvement Triple Aim, of ‘simultaneously improving the patient experience of care (including quality and satisfaction), improving the health of the population, and reducing per capita cost of care for the benefit of communities’. 15 However, we must express caution in this assessment, as such improvements are not provable in the absence of direct comparison with a group of patients accessing routine preassessment care. We do believe our pathway facilitates a ‘choosing wisely’ approach to surgery, aligning with the ANZCA Choosing Wisely statement number four, 16 and Health Quality and Safety New Zealand’s goal of promoting shared decision-making as a component of choosing wisely. 17 A Cochrane Review 18 of studies on the use of decision aids suggests that they enable patients to feel better informed and more knowledgeable, which may result in patients having better risk perception and making more value-congruent choices. There was evidence from this meta-analysis that decision aids reduced decisional conflict, improved patient–clinician communication, and some evidence that their use reduced the number of patients choosing major elective invasive surgery in favour of more conservative options. The study findings presented here suggest that our decision-making pathway may lead to similar outcomes, with themes of feeling informed and experiencing good communication particularly evident in participant responses, and a high percentage of participants deciding against major surgery. Although again, we are unable to definitively demonstrate such impacts in the absence of a direct comparison with standard care.
In conclusion, the results of this prospective study demonstrated that our shared decision-making pathway assisted in appropriately risk-stratifying participants into operative and non-operative groups, resulted in positive participant experiences, and was a cost-effective intervention. We have achieved these results in a non-tertiary centre, using resources that are widely available to perioperative services throughout Australasia, and we believe the service is highly reproducible.
Footnotes
Author Contribution(s)
Acknowledgements
Thank you to Associate Professor Rachelle Bernacki (MD MS FAAHPM AGSF, Director of Quality Initiatives in Adult Palliative Care, Department of Psychosocial Oncology and Palliative Care, Dana-Farber Cancer Institute; Director of Care Transformation and Postoperative Services, Brigham and Women’s Hospital Center for Geriatric Surgery; Founder of the Serious Illness Community of Practice, Ariadne Labs; and Associate Professor, Harvard Medical School) and Associate Professor Tanisha Jowsey for answering questions and providing advice. Thank you to the many CDP clinicians and administrators who make the service possible. And thank you to our study participants for contributing their time, data and feedback.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.