
Abstract
Occupationally acquired COVID-19 is a hazard for healthcare workers (HCWs). In four hospitals of the Metro North Hospitals and Health Service in Queensland, Australia, we invited HCWs to report the nature of any anaesthesia interactions with COVID-19-positive and COVID-19-suspect patients. This was to assist workforce planning in future pandemics. Data collection consisted of three phases; 1) participating HCWs recorded details of episodes of care (EOCs) with COVID-19-positive or COVID-19-suspect patients; 2) these HCWs were invited to complete a follow-up survey about their own health status regarding COVID-19 infections; 3) electronic health records were used to assess patient demographics, infectious status and outcomes. Between 21 March 2020 and 17 May 2022, 63 anaesthesia HCWs reported 90 EOCs with 67 unique patients. The median (interquartile range (IQR)) age of the HCWs was 40.5 years (34–46); 55% (34/62) were male, 62% (39/63) were consultants and 21% (13/63) were registrars. The median (IQR) age of patients was 39 (28–63) years. Personal protective equipment (PPE) was deemed to be appropriate by the HCWs in (86/88) 98% of the EOCs. Twenty-four HCWs (38%) responded to a follow-up survey. Of 12 HCWs who subsequently tested positive to COVID-19, only four had cared for a COVID-19-positive patient in the two weeks prior to their diagnosis. Most responding HCWs perceived they contracted COVID-19 in the community, experiencing mild illness. We found relatively low COVID-19 case numbers, high PPE use and low transmission of COVID-19 within the hospital setting.
Introduction
With the arrival of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and the subsequent declaration in March 2020 of a coronavirus disease 2019 (COVID-19) pandemic, healthcare workers (HCWs) have been exposed to increased occupational risk. 1 While workers in non-healthcare settings were asked to work from home and socially distance, HCWs were often unable to work from home and required to be proximate to COVID-19-positive patients to provide care. During previous severe acute respiratory syndrome (SARS) epidemics, transmission was more likely to occur in a hospital setting, and early in the COVID-19 pandemic it was noted that frontline HCWs had a threefold increased risk of COVID-19 infection when compared with the general community. 2 Among hospital-based HCWs during the COVID-19 pandemic, those that were patient-facing had the highest risk of SARS-CoV-2 infection. 3
At the start of the COVID-19 pandemic there were concerns that anaesthesia HCWs would be at increased risk of nosocomial COVID-19 infection due to their work environment, patient caseload and exposure to aerosol-generating procedures (AGPs) such as tracheal intubation. 4 Further, non-AGPs performed in proximity to the patient (for example, leaning across the patient to place electrocardiograph (ECG) monitoring) may also increase risk, as demonstrated in previous SARS outbreaks. 5
Nosocomial infection prevention research from previous SARS outbreaks relied on retrospectively collected data.5 –7 HCWs were asked to recall, sometimes months after an episode of care (EOC), the types of care they delivered and the steps they took to mitigate transmission, such as the wearing of personal protective equipment (PPE).
It is our impression that there is a disconnect in the literature between theoretical risk management and real world outcomes. For example, it has been theorised that strategies such as using regional anaesthesia (to avoid using AGPs) could either decrease risk as intended, or increase risk (due to unintended consequences such as unplanned intubation). 8 We believe this paucity of real world data may extend to other strategies intended to decrease risk such as intubation/extubation protocols, avoidance of supraglottic airways, and novel devices (such as plastic shielding).
We designed a study to prospectively collect detailed observational data regarding the type, frequency and nature of anaesthesia HCW interactions with COVID-19-positive and COVID-19-suspect patients during the pandemic. Tracking these activities may allow anaesthesia departments to monitor the health and safety of HCWs and to mitigate risk. These insights may help inform planning for future pandemics (for example, workforce planning, allocation of staff to tasks, PPE utilisation and best practice for reducing occupational risk).
Methods
We designed a multicentre longitudinal observational cohort study. Data were collected at four hospitals of the Metro North Hospitals and Health Service in Queensland, Australia: The Royal Brisbane and Women’s Hospital, The Prince Charles Hospital, Redcliffe Hospital and Caboolture Hospital.
The Royal Brisbane and Women’s Hospital is a major quaternary hospital and is one of the largest hospitals in Australia, with almost 1000 beds and a 36-bed intensive care unit (ICU). Covering all major medical and surgical specialties (except paediatrics and cardiac), it is a referral centre for specialist cancer, maternity, trauma and burns care. The Prince Charles Hospital is a 700-bed quaternary teaching hospital in north Brisbane with a 25-bed adult ICU. It is the hub for specialised cardiothoracic services, including heart and lung transplants, and provides general surgical, medical and paediatric services. Redcliffe Hospital is a regional hospital providing medical, surgical, maternity and paediatric services. It is a 250-bed hospital located about 30 km north of Brisbane. Caboolture Hospital is a regional hospital located almost 50 km north of Brisbane. It has 265 beds and offers medical and surgical services to around 150,000 people per year. The Metro North Hospitals and Health Service policies regarding PPE and vaccination were consistent across the four participating hospitals. COVID-19 vaccination became available in February 2021 and was mandatory for all anaesthesia HCWs.
Ethical approval was obtained from the RBWH Human Research Ethics Committee (LNR/2020/QRBW/63539). Participant consent was implied by reporting cases and survey completion.
Data collection consisted of three phases. Phase 1 involved prospective data collection. Anaesthesia HCWs were invited to keep an electronic ‘logbook’ record of EOCs with a COVID-19-positive or COVID-19-suspect patient. Anaesthesia HCWs were defined as anaesthesia consultants, anaesthesia registrars, medical trainees doing an anaesthesia rotation, anaesthesia health practitioners or anaesthesia nurses. Departmental emails, meetings, posters, social media and a site ‘champion’ were used to promote data entry. Participants could use their own devices or a hospital computer to enter data for each EOC into the Research Electronic Data Capture database (REDCap9,10). Participants entered details regarding their own demographic data, a description of the care they provided, and the PPE used (online Supplementary material, ‘Survey questions and data queries’). For the purposes of our research a COVID-19-positive patient was defined in 2020 as having a documented polymerase chain reaction positive nasal or oropharyngeal swab, or positive to any future Metro North Hospital and Healthcare Service approved tests using different methodology. A COVID-19-suspect patient was defined as meeting contemporaneous Metro North Hospital and Healthcare Service criteria (which changed during the pandemic). COVID-19-suspect patients were treated as if they were COVID-19-positive.
A second phase of retrospective data collection was a HCW self-reported survey assessing HCW COVID-19 infections acquired during the pandemic. Participants provided information including timing, severity, risk factors and perceptions about COVID-19 transmission. The third phase of retrospective data collection utilised electronic health records to assess patient demographics, COVID-19 status and outcomes. Information collected included patient age, gender, body mass index, comorbidities, COVID-19 severity, surgery and anaesthesia type, length of stay and in-hospital mortality.
Data were summarised using mean (standard deviation (SD)), median (interquartile range (IQR)) or frequency (percent) as appropriate, using STATA 15 (Stata Corp (2017) Stata Statistical Software: Release 15. College Station, TX, USA). Pre-planned analyses included exploring factors associated with occurrence of COVID-19 in HCWs. However, this associative analysis was not feasible due to lower numbers of COVID-19-positive or -suspect patients than expected, as a result of State-specific government interventions.
Results
Between 21 March 2020 and 17 May 2022, 63 anaesthesia HCWs reported 90 EOCs with 67 unique patients. Sixty-four (71%) EOCs documented caring for COVID-19-positive patients and 26 (29%) EOCs documented caring for COVID-19-suspect patients (online Supplementary Table S1). Subsequent interrogation of medical records showed that of the 26 EOCs documented as COVID-19-suspect, four of these EOCs represented patients that subsequently tested positive to COVID-19 during their admission. Medical records also revealed that of the 64 EOCs documented by HCWs as COVID-19-positive, four were with COVID-19-suspect patients that did not test positive during their admission.
HCWs self-reported their own demographic data (Table 1). The median (IQR) age of participating HCWs was 40.5 (34–46) years, and 43% of workers had five or fewer years of experience in their current role.
Characteristics of 63 healthcare workers who had episodes of care with COVID-19-positive or COVID-19-suspect patients.
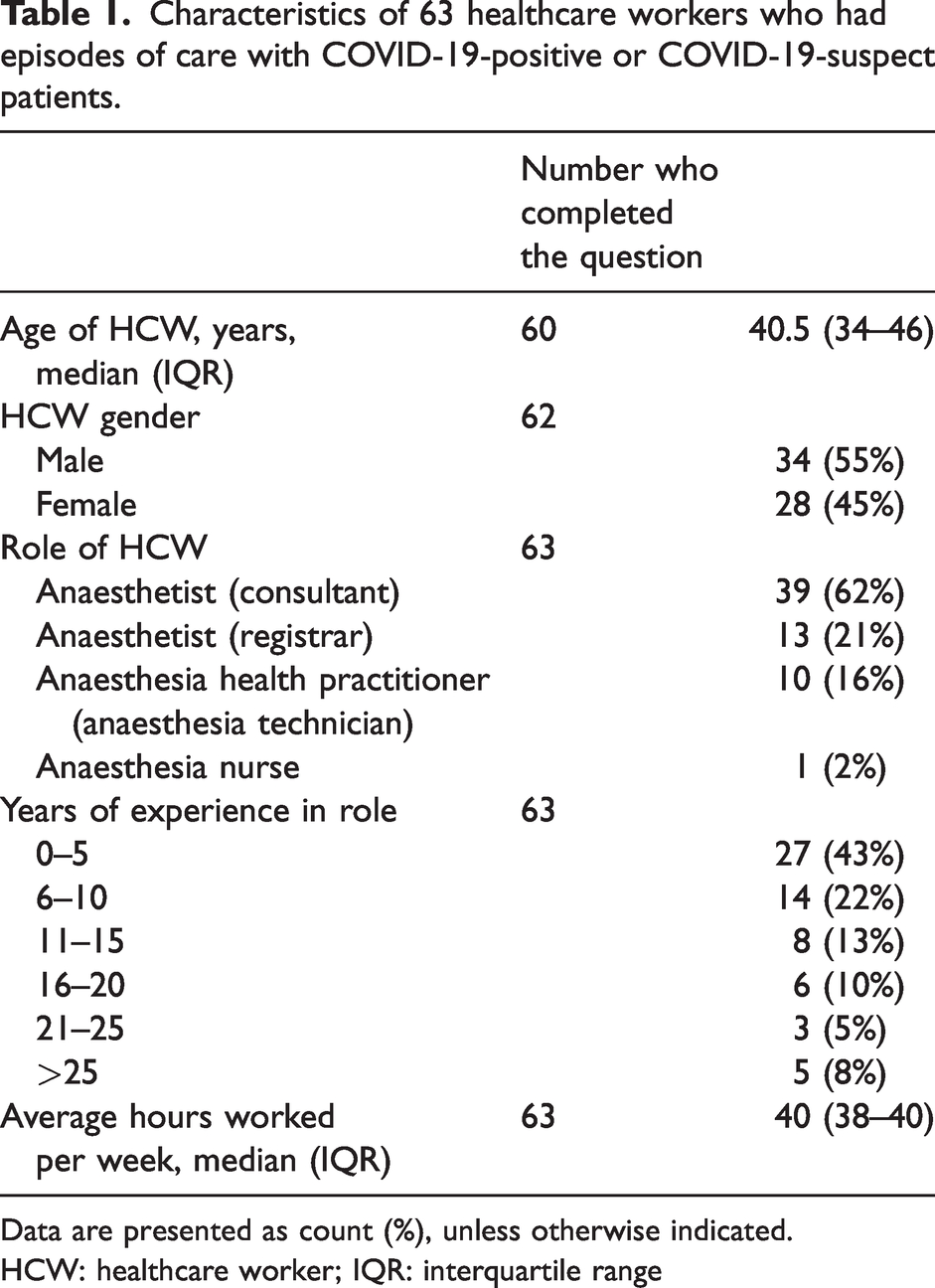
Data are presented as count (%), unless otherwise indicated.
HCW: healthcare worker; IQR: interquartile range
Medical records were used to record patient demographics and outcomes (Table 2). The median (IQR) age of patients was 39 (28–63) years. Most patients had either asymptomatic (51%) or mild disease (38%). Two patients (3%) died in hospital. Sixty percent of patients had general anaesthesia, 32% had regional anaesthesia and 5% had combined general and regional anaesthesia.
Patient characteristics, based on 67 patients cared for during 90 episodes of care.
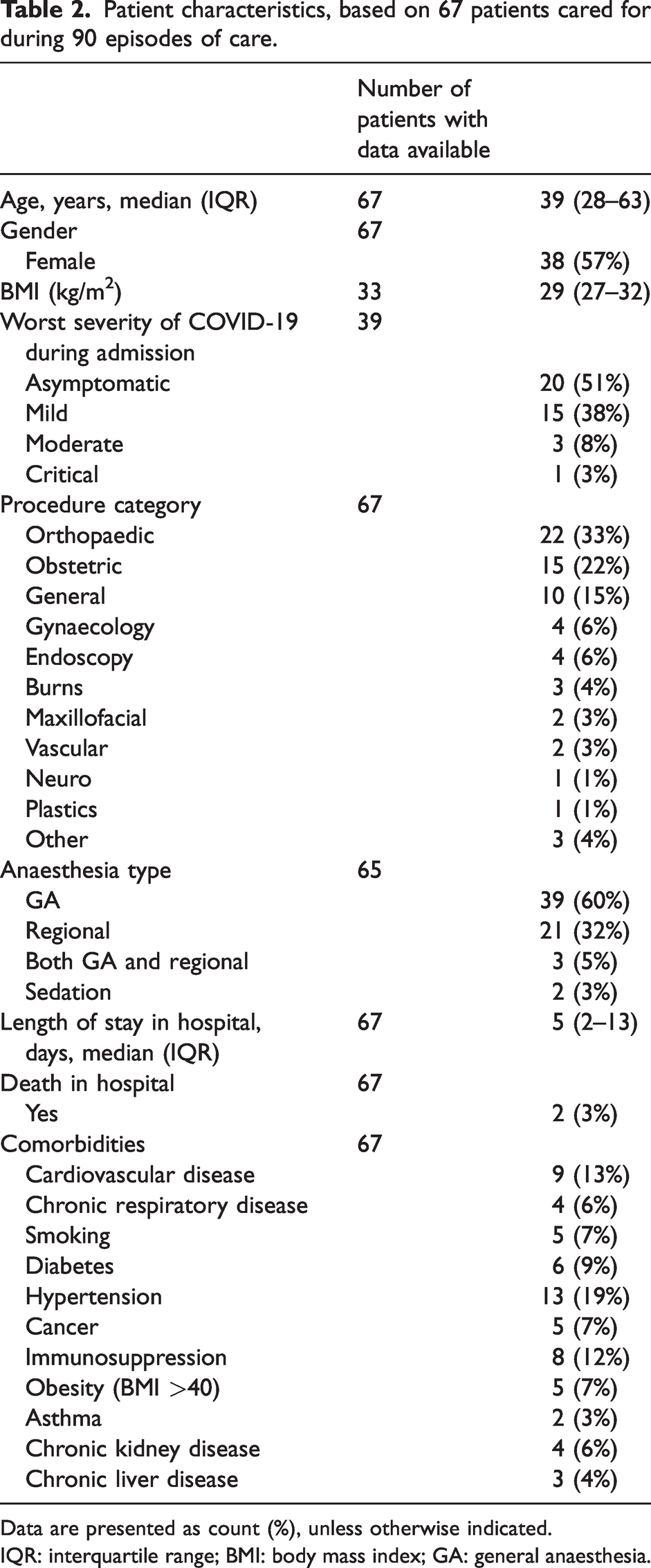
Data are presented as count (%), unless otherwise indicated.
IQR: interquartile range; BMI: body mass index; GA: general anaesthesia.
Most EOCs were for providing anaesthesia services in the operating theatre, with nine (10%) occurring in remote locations (Table 3). Only one EOC involved anaesthesia HCWs intubating a patient for the sole reason of respiratory compromise. Forty-one EOCs involved an insertion of an airway device. Of those 41, 25 (61%) involved endotracheal tube (ETT) insertion, with videolaryngoscopy utilised in 17 (41%). Planned laryngeal mask (LMA) insertion occurred in 14 (34%) of EOCs. Airway devices were removed during 34 EOCs, with a planned exchange from ETT to LMA used in five (15%) EOCs. Regional anaesthesia was performed in 25 (28%) EOCs. Eighteen of these were for obstetric procedures. In six EOCs (24%), the HCW recorded the patient as being without a facemask when first encountered.
Episode of care characteristics, as reported by healthcare workers (N = 90 episodes).
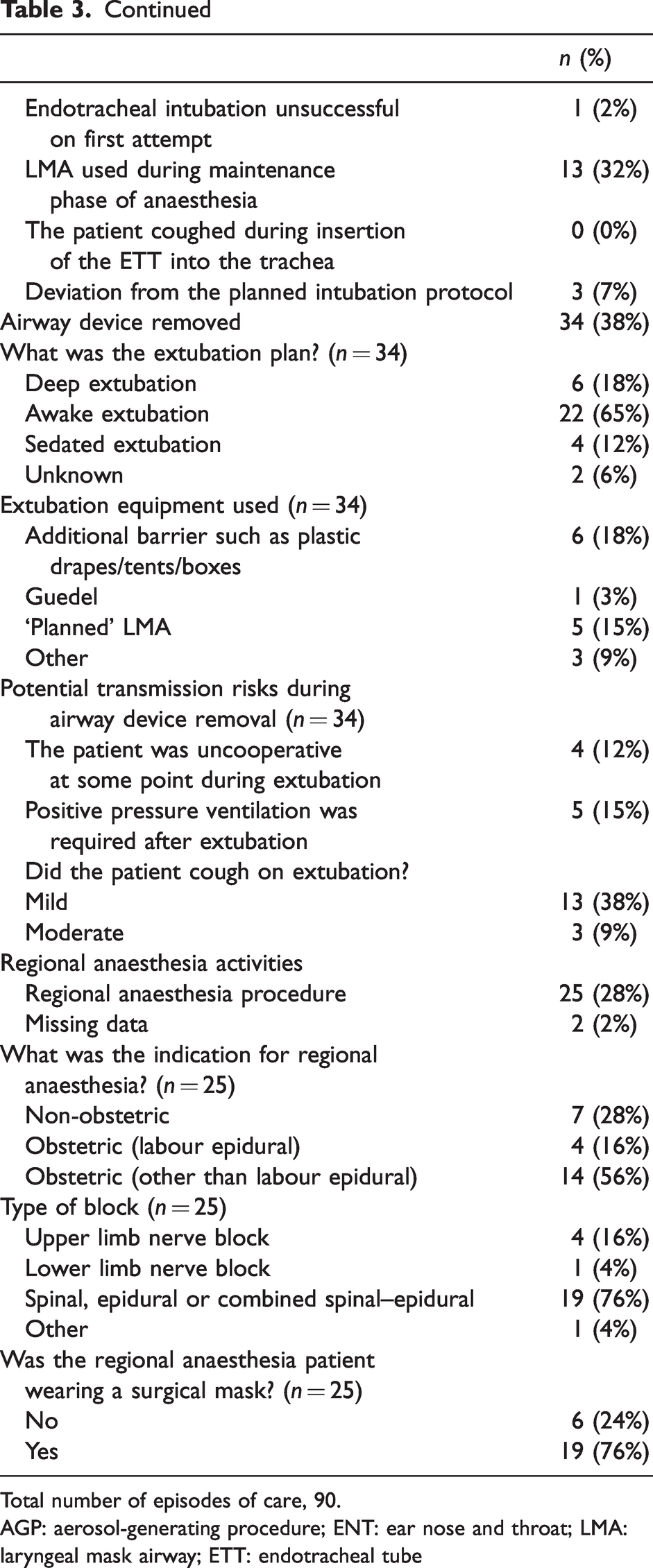
Total number of episodes of care, 90.
AGP: aerosol-generating procedure; ENT: ear nose and throat; LMA: laryngeal mask airway; ETT: endotracheal tube
The nature of anaesthesia HCW activities involved a variety of tasks that exposed HCWs to potential COVID-19 transmission (Table 4). During 65 EOCs (72%) the anaesthesia HCW was involved in patient positioning. Other activities bringing HCWs into proximity with COVID-19 patients included venous cannulation (24 EOCs, 27%), placement of ECG monitoring (43 EOCs, 48%), administering medicines (58 EOCs, 64%) and touching patient eye covers (37 EOCs, 41%). HCWs spent greater than 3 h in proximity (within 2 m) to COVID-19 patients in 19 EOCs (22%).
The nature of healthcare worker activities during episodes of care.
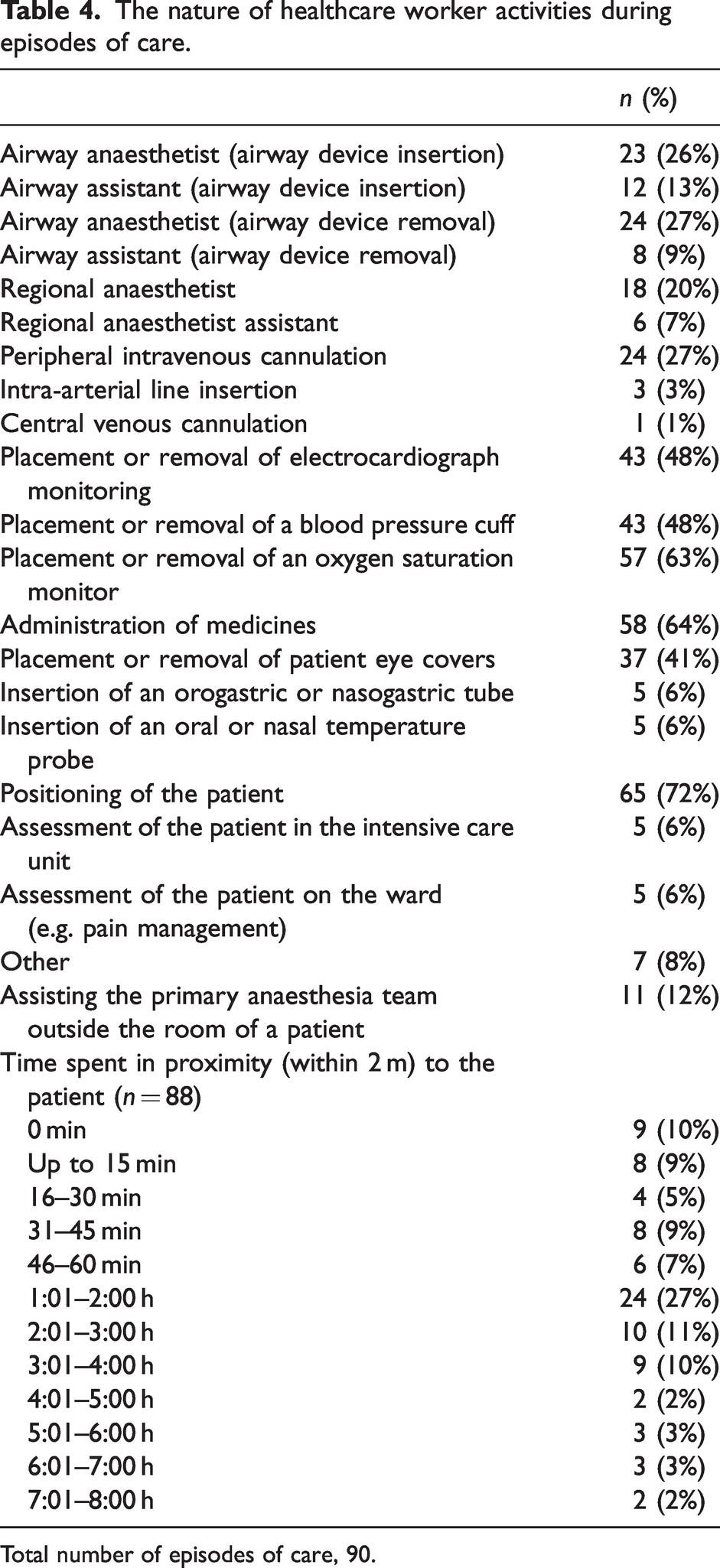
Total number of episodes of care, 90.
The availability of PPE was deemed to be appropriate by participating HCWs in 98% of EOCs (online Supplementary Table S2). HCWs reported a high usage of either N95/P2 mask (92% of EOCs) or Powered Air Purifying Respirator (8% of EOCs). Doffing was checked by a second HCW in 92% of EOCs. PPE breaches were recorded in 5% of EOCs.
A follow-up survey sent to 63 HCWs received 24 responses (response rate 38%). Twelve of the 24 responding HCWs reported testing positive to COVID-19 at some time between an EOC and follow-up (Table 5).
Health outcomes of healthcare workers.
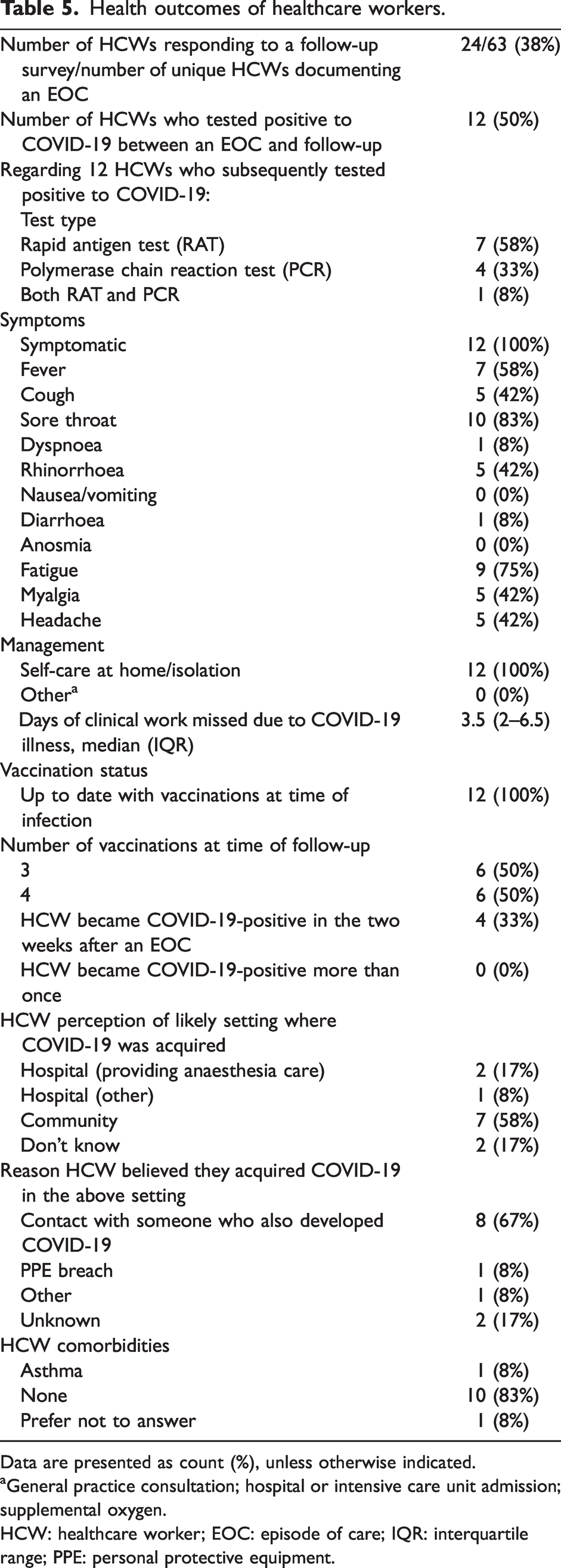
Data are presented as count (%), unless otherwise indicated.
General practice consultation; hospital or intensive care unit admission; supplemental oxygen.
HCW: healthcare worker; EOC: episode of care; IQR: interquartile range; PPE: personal protective equipment.
Regarding the 12 HCW respondents who subsequently tested positive to COVID-19, only four respondents (33%) had cared for a COVID-19-positive patient in the two weeks prior to their own diagnosis. Two respondents (17%) perceived they contracted COVID-19 in an anaesthesia clinical setting; most respondents (n = 7, 58%) believed they contracted COVID-19 in the community. Only one respondent attributed their COVID-19 diagnosis to a breach in PPE.
All HCWs who tested positive to COVID-19 reported being up to date with vaccination at the time of diagnosis. Most (n = 10, 83%) had no pre-existing health conditions. All HCWs who reported a diagnosis of COVID-19 reported a mild illness requiring self-care at home without hospital admission. The total number of missed days of work owing to illness or isolation requirement among the 12 HCWs diagnosed with COVID-19 was 49.
Discussion
We have used contemporaneously collected self-reported data from participating anaesthesia HCWs, cross-referenced with electronic medical records, to describe HCW interactions with COVID-19-positive and COVID-19-suspect patients during the pandemic in four hospitals of the Metro North Hospitals and Health Service in Queensland, Australia. We believe our process for data collection can be replicated and upscaled in the event of future pandemics.
Results of this research need to be viewed in the context of the Australian and Queensland (QLD) experience of the global pandemic, during the period of data collection. When this study was conceived in March 2020 there was a fear that the northern hemisphere experience of large numbers of COVID-19 deaths, including HCWs, would be replicated in Australia. However, by July 2021, QLD had recorded only seven COVID-19 deaths. 11 Several significant changes occurred in QLD during this research: the development and distribution of vaccinations (first available in QLD in February 2021, and mandatory for HCWs); restricted movements of people (multiple Brisbane lockdowns, State and Federal border closures, isolation and quarantine requirements, restricted public gatherings); mandatory facemask wearing requirements; contact testing; and tracing measures.
At the end of the data collection (31 May 2022) there had been 1,174,627 recorded cases of COVID-19 in QLD and 1051 deaths, 12 among an estimated population of 5,322,058 persons (QLD Government Statistician’s Office, 30 June 2022). On 30 May 2022 the cumulative COVID-19 death rate was estimated to be 353 per million people in Australia, compared with over 2900 deaths per million in the UK and USA. 13 In summary, there were fewer cases of COVID-19 in QLD than predicted at study conception. We found a low number of HCW interactions with COVID-19-positive or -suspect patients, high PPE use and low transmission of COVID-19 within the hospital setting.
During previous SARS outbreaks, transmission of coronavirus occurred mostly in the healthcare setting. For example, during the 2003 Toronto SARS coronavirus outbreak 72% of cases were acquired in the healthcare setting. 5 By contrast, during the COVID-19 pandemic community transmission was common. In the Australian setting (Melbourne, 2020) HCWs were more likely to be infected in the community rather than in the workplace. 14 Our research found that two-thirds of HCW respondents who tested positive for COVID-19 had not cared for a COVID-19 positive patient in the two weeks prior to their own diagnosis, suggesting community rather than hospital transmission. When surveyed, most believed that they were infected in the community.
Previous research has identified several associations with occupational transmission of SARS-CoV-2 in HCWs, including inadequate PPE use,2,15 presence of comorbidities, 15 working in a doctor’s role, 15 taking public transport to work, 15 female HCWs, 16 patient-facing HCWs,2,3 junior doctors, 3 healthcare support workers, 3 hospital nurses, 3 younger HCWs, 3 living in more deprived areas, 3 clinical setting, 2 ethnicity 2 and country of practice. 16 An observational study in the UK in 2020 identified increasing contact with COVID-19-positive or -suspect cases without adequate PPE as the strongest risk factor. 15
Preventing occupational transmission of COVID-19 in the hospital setting can be achieved by measures such as correct PPE usage. Even in high-risk settings, such as emergency intubations of COVID-19 patients, it is possible to avoid occupational transmission with the use of intubation protocols including PPE. 17 We found high levels of PPE availability and utilisation. Compared with 22.5% of British HCWs who reported inadequate access to PPE, 15 anaesthesia HCWs in our series reported adequate PPE supply in 98% of interactions.
Even with ample PPE, transmission of SARS-CoV-2 can still occur in HCWs, 18 emphasising the need for PPE training. Only two-thirds of HCWs in one study appropriately used PPE consistent with current guidelines. 18 Correct doffing behaviour is thought to be particularly important. 19 Our study showed adequate staffing levels for reported cases such that a second HCW could check doffing technique.
During the pandemic anaesthesia departments faced the dilemma of deciding which HCWs would be assigned COVID-19-positive cases and whether some staff should be exempt from such cases. While some COVID-19 intubation protocols recommend that intubation should be performed by the most skilled clinicians, 20 who are likely to be more experienced and thus older, known risk factors for severe COVID-19 infection include older age and comorbidities. 4 Our research showed that anaesthesia HCWs who participated in our survey and cared for COVID-19-positive or -suspect cases had a median age of 40.5 years. Although many had less than five years’ experience in their current role, that role was described as ‘consultant’ in 62% and ‘registrar’ in 21%. Of those who reported being infected, most had no pre-existing conditions. Younger age and a lack of comorbidities may account for the low severity of COVID-19 disease seen in infected HCWs in our series.
The requirement for HCWs to isolate, even with asymptomatic or mild illness, has major ramifications for workforce numbers, provision of care, and surgical waiting lists. Similar to our experience, others have reported large numbers of missed working days. 15
Strengths of our study design include prospective contemporaneous collection of data that did not limit episodes of care to endotracheal intubation, in recognition of multiple mechanisms of COVID-19 transmission. A further strength is that, unlike other COVID-19 research solely relying on self-reported data, we were able to validate HCW-reported data by cross-referencing with electronic medical records. In a time of healthcare crisis, we rapidly designed, obtained approvals for and implemented a detailed method of data collection which could be upscaled in future pandemics, to monitor the practice and occupational safety of anaesthesia HCWs.
A major limitation of our research is the lower than predicted number of COVID-19 cases recorded. This is likely due to a combination of a low incidence of COVID-19 cases and a small number of HCWs self-reporting in Phase 1 of data collection. Participation of HCWs was voluntary, thus we are unable to determine the total number of HCW interactions or the proportion of respondents in Phase 1. There was also a low response rate to the second phase of data collection and the results may be influenced by responder bias. Caution should be exercised when interpreting these small datasets as inferences can be unreliable. HCW follow-up rate may have been hampered by staff being fatigued or unwell (for example, severe COVID-19, long COVID-19, or death). We are not aware of any COVID-19-related deaths of anaesthesia HCWs at any of our four anaesthesia departments. Planned analysis for associations between HCW activities and COVID-19 infection was not appropriate owing to the low numbers of cases and the advent of mandatory vaccination. Our research was conducted at public hospitals in and around Brisbane City and is limited in its generalisability to similar hospitals, and may not represent other settings such as private hospitals, rural hospitals and other jurisdictions that had differing COVID-19 policies.
Preventing occupational infection of HCWs is crucial, as workers may be part of the solution (caring for pandemic patients) and problem (potential vectors for transmission) in pandemic management. ‘Hierarchy of Controls’ theory 1 suggests that elimination (physically avoiding the hazard, via isolation strategies, for example) is the most effective strategy for protecting workers. Australian, and specifically QLD, HCWs were fortunate to be exposed to relatively few COVID-19-positive patients, particularly in the time frame prior to vaccine distribution. Should elimination strategies fail during future pandemics, there will need to be greater understanding of the other tiers of hazard control: substitution, engineering, administration and PPE.
We have described the nature of anaesthesia HCW interactions with COVID-19-positive and -suspect patients in a subpopulation of workers from within the Metro North Hospitals and Health Service in QLD. We found relatively low COVID-19 case numbers, high PPE use and low hospital transmission of COVID-19.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X241265723 - Supplemental material for Anaesthesia healthcare workers’ interactions with COVID-19-positive and -suspect patients: A multi-site observational study from Queensland, Australia
Supplemental material, sj-pdf-1-aic-10.1177_0310057X241265723 for Anaesthesia healthcare workers’ interactions with COVID-19-positive and -suspect patients: A multi-site observational study from Queensland, Australia by Adrian Chin, Christine Woods, Anita M Pelecanos, Angela Tognolini, Gunjan Chawla, Sheridan Bell, Ivan L Rapchuk, Jimmy Wang and Victoria A Eley in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.