
Abstract
Routine chest X-ray (CXR) post intrathoracic drain removal in cardiac surgical patients is common practice to identify the presence of a pneumothorax following drain removal. Such pneumothoraces occur infrequently and rarely require intervention. We investigated the utility of routine CXR post drain removal and hypothesised that the practice is unnecessary and a possible area for significant cost saving. We conducted a single-centre, retrospective study of 390 patients who underwent cardiac surgery over a one-year period. Routine CXR post drain removal was reviewed for the presence of a pneumothorax. Rates of intervention post routine CXR were analysed to assess for clinical benefit obtained from this practice. Potential cost savings were calculated by the cost of a mobile CXR and by considering the radiographer’s time. There were 15 pneumothoraces detected on routine CXR post drain removal. All pneumothoraces detected on routine post drain removal CXR were defined as small. No patients had a clinically significant pneumothorax requiring re-insertion of a chest drain. The potential cost saved by omitting routine CXR post drain removal was estimated to be approximately A$7750 per year. This study did not detect any clinically significant pneumothoraces requiring intervention. It also suggests that routine CXR post drain removal does not provide any clinical benefit and indicates that current practice should be reviewed.
Introduction
Routine chest X-ray (CXR) post intrathoracic drain removal is common practice and is usually driven by surgeon preference or institutional policies. 1 The use of routine CXR post intrathoracic drain removal aims to identify complications, including the occurrence of a pneumothorax. 2 Studies on the utility of CXR post intrathoracic drain removal are limited; however, published data indicates that the incidence of pneumothorax post drain removal in cardiac surgical patients is low. Furthermore, the incidence of clinically significant pneumothorax post drain removal requiring re-insertion of an intrathoracic drain is very low.1 –3
A review of the available literature was conducted as part of this study using PubMed and SCOPUS with the search terms ‘routine chest x-ray’, ‘chest drain removal’, ‘cardiac surgery’, limiting the results to journal articles published from the year 2006 onwards. A total of 78 articles across both search platforms had titles and abstracts reviewed, with 10 articles being identified as relevant, excluding paediatric and trauma patients.
The most recent consensus guideline produced by the New South Wales Agency for Clinical Innovation Respiratory Network advises to perform a routine CXR 2–4 h post drain removal. 4 A more recent expert panel review conducted by the American College of Radiology (ACR) disagreed with the recommendation of performing routine CXR post intrathoracic drain removal. 5 Although neither of these guidelines is specific to intrathoracic drain removal post-cardiac surgery, a number of other studies that are specific to post-cardiac surgical patients suggest that omission of post chest drain removal CXR can be safe, resulting in a reduction of healthcare costs and resource utilisation.1 –3,5 –7
Post drain removal pneumothorax incidence in cardiac surgical patients has been reported in the range of 0.23% to 9.3% across a number of prospective and retrospective studies.2,3,8 –10 Within the study reporting the highest incidence rate, 70.3% of the newly detected pneumothoraces post drain removal were barely perceptible, with an intervention rate of only 0.25%. 8 A 2022 systematic review reported an intervention rate of 0.5% to 1.3% and summarised that routine CXR post intrathoracic drain removal can be safely omitted without compromising patient safety. 11 Further studies also concluded that the use of routine CXR post chest drain removal has limited utility and that CXRs should only be obtained when there is a clinical indication.1,12 –14
Alternatively, the use of bedside ultrasonography may be used to accurately identify clinically significant pneumothoraces, avoiding ionising radiation and reducing costs compared with CXR.11,15 Furthermore, a best evidence topic reviewing six articles on routine CXR post chest drain removal following cardiac surgery stated that clinical findings were a major predictor of re-intervention, 10 suggesting that these could be relied upon to predict the need for additional CXRs.
With rising healthcare costs and a growing population, optimising resource utilisation with cost-effective practices requires continued evaluation of current practices. Evidence-based practice has been demonstrated to improve patient outcomes as well as reduce healthcare costs and unnecessary procedures and investigations.16,17 The cost saving by omitting routine CXR post drain removal will depend on how many procedures are completed each year. However, a UK study within a centre performing approximately 750 cardiac surgical procedures each year estimated an annual saving of £10,000 (A$20,000) from performing CXR only when clinically indicated rather than routinely. 2
Currently there is a paucity of data on routine CXR post intrathoracic drain removal in cardiac surgical patients, with the ACR expert panel stating that there is insufficient evidence to conclude whether patients benefit from this practice. The limited literature that does exist indicates that routine CXR is an unnecessary investigation and that performing CXR only when clinically indicated may lead to better utilisation of healthcare resources and reduced costs without compromising patient safety.
Method
This was a single centre retrospective study that included patients who underwent cardiac surgery from 1 January to 31 December 2021 at Westmead Hospital, NSW, Australia. All patient data was obtained by review of electronic medical records covering their entire hospital and intensive care admission. All data was anonymised. Inclusion criteria were age ≥18 years old, cardiac surgery including coronary artery bypass graft (CABG), valvular and congenital cardiac surgeries, and having a routine CXR performed post intrathoracic drain removal. Exclusion criteria included pulmonary surgery, upper gastrointestinal surgery and the absence of an intrathoracic drain.
Patients with Acute Physiology and Chronic Health Evaluation III diagnosis codes 1206 (valvular heart surgery), 1207 (CABG), 1212 (CABG with valve repair/replacement), 1208.02 (aneurysm repair, ventricular), 1208.05 (CABG—minimally invasive), 1208.08 (complications of previous open-heart surgery), 1208.09 (defibrillator, insertion of), 1208.13 (pericardial effusion/tamponade), 1208.14 (pericardiectomy—total/subtotal), 1208.15 (tumour removal, intracardiac), 1208.19 (congenital defect repair—other), 1208.20 (atrial septal defect repair), 1208.21 (ventricular septal defect repair), 1208.22 (heart transplant), 1208.24 (Bentall’s repair), 1209.02 (aneurysm, thoracic aorta; with dissection) and 1210.02 (aneurysm, thoracic aorta; with rupture) admitted to the intensive care unit (ICU) postoperatively throughout the year of 2021 were accepted for this study.
Data was collected on patient demographics, surgery performed, number of intrathoracic drains, drain position, ventilation, timing of drain removal, time to routine CXR post drain removal, presence of pneumothorax post intrathoracic drain removal and re-insertion of drain and ICU length of stay (LOS).
Patients followed the local post-cardiac surgical protocol, which involves routine CXR on admission to ICU; daily CXR whilst drains are in situ; routine post drain removal CXR; routine CXR the next day after drain removal; routine CXR on postoperative day 4; and then as otherwise clinically indicated. If drains are expected to be removed, then the morning CXR may be delayed until post drain removal. All surgical intrathoracic drains are removed in ICU with continuous monitoring post drain removal. Further CXRs are then performed on the cardiothoracic step-down ward as indicated by the cardiothoracic surgical team.
Chest drain removal was at the discretion of the cardiothoracic surgical team, who followed the protocol of removing the drain once there was an absence of an air leak and drain output was <50 ml/h for two consecutive hours, unless otherwise clinically indicated. Chest drains were removed by experienced cardiothoracic nurses who have received local training and accreditation to remove intrathoracic drains in a standardised manner utilising the Valsalva manoeuvre, with an occlusive dressing placed on the site post removal. The current policy at this institution is to perform a routine CXR no sooner than 4 h after drain removal.
Pneumothorax post intrathoracic drain removal was identified via the formal CXR radiologist report. If no formal CXR report was available, then the CXR image was reviewed by two independent researchers for diagnosis of pneumothorax.
Pneumothorax size was defined using the British Thoracic Society pleural disease guideline, which defines a small pneumothorax as the distance from lung margin to chest wall as <2 cm at the level of the hilum and a large pneumothorax as >2 cm. 18
Clinical signs and symptoms were identified via analysing vital sign trends, medication titration and clinical documentation available from the electronic medical record. Criteria for clinical signs and symptoms included the presence of two or more of the following: documentation of new onset shortness of breath, chest pain, distended neck veins, new unequal air entry, desaturation, tachycardia, hypotension or new or increasing vasopressor requirement not explained by an alternative pathology.
Of the patients who had a pneumothorax present on the post drain removal CXR, the presence of chronic obstructive pulmonary disease (COPD) was assessed. COPD was deemed present if it was documented within the patient’s past medical history, if they were taking medication for COPD, or if they had a documented spirometry result consistent with the diagnosis of COPD.
Cost analysis of post drain CXRs was performed with an extra CXR being defined as a second CXR performed on the same day specifically for the purpose of post drain removal. Cost savings were then calculated based on the cost of a mobile CXR.
Ethical approval was received from the Human Research Ethics Committee, Westmead Hospital prior to commencement of data collection. The study was performed in accordance with the Good Clinical Research Practice Guidelines. As this study was a retrospective observational study, it was considered as low/negligible risk to patients and, as a result, the requirement for informed consent was waived. Study data was analysed using Microsoft Excel.
Results
A sample size of 413 patients admitted to the cardiothoracic ICU were screened, of which a total of 390 met inclusion criteria as demonstrated in Figure 1.
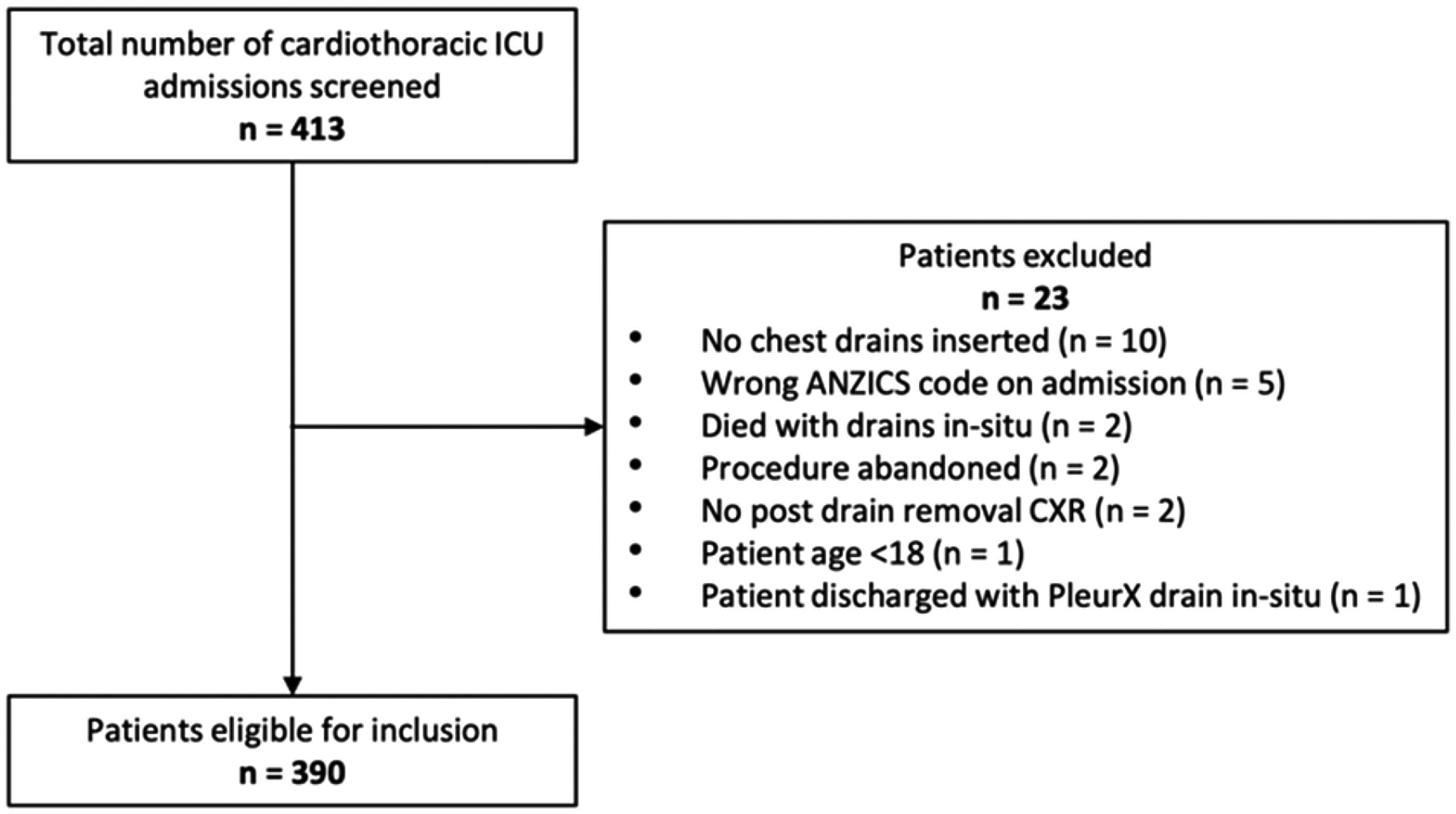
Flowchart of patient enrolment. ICU: intensive care unit; ANZICS: Australian and New Zealand Intensive Care Society; CXR: chest X-ray.
Only 5.1% of patients had a routine CXR at least 4 h post drain removal, while 73.1% of patients had a routine CXR post drain removal within 2 h, as shown in Table 1. All patients returned to ICU intubated and ventilated post-cardiac surgery, but only 14.1% had intrathoracic drains removed whilst ventilated.
Demographics and clinical characteristics.
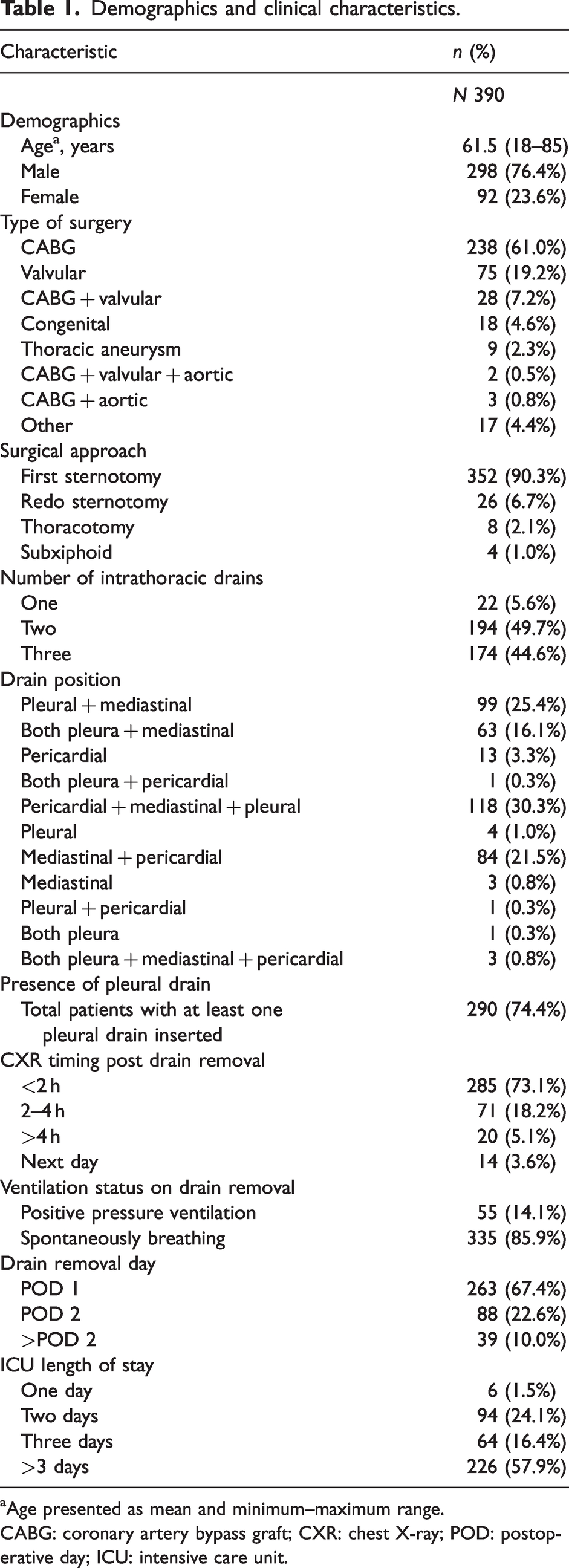
Age presented as mean and minimum–maximum range.
CABG: coronary artery bypass graft; CXR: chest X-ray; POD: postoperative day; ICU: intensive care unit.
Tables 2 and 3 present the incidence and definition of pneumothoraces detected during the study. There were a total of 15 pneumothoraces detected, of which 13 had at least one pleural drain in situ. All post drain removal CXRs had a formal report available to assess for the presence of a pneumothorax.
Incidence of pneumothorax.

CI: confidence interval
Pneumothorax definition.
Three of the patients who had a pneumothorax detected on routine CXR had an air leak recorded that had resolved prior to drain removal to meet removal criteria. No pneumothoraces that were detected on routine CXR post drain removal required intervention.
One patient developed a large pneumothorax 20 h post drain removal that was not detected on routine drain removal CXR. A further CXR was performed following the development of tachypnoea and reduced right-sided air entry. This pneumothorax was monitored clinically and radiologically and resolved without further intervention.
Three patients had drains inserted for symptomatic pneumothoraces that developed despite the presence of existing surgical drains. Symptoms present included desaturation, tachypnoea and haemodynamic instability evidenced by increasing vasopressor requirements.
Two patients had drains inserted for asymptomatic pneumothoraces identified on routine CXR performed outside of ICU. Of these two patients, one had a drain inserted prophylactically for a pneumothorax that developed two days post drain removal and the other had a drain inserted for a pneumothorax that developed four days post drain removal.
Of the patients that had drains inserted for pneumothoraces, 66.7% had signs and symptoms. Of the patients requiring drain insertion for a pneumothorax, none had an intervention as a result of a pneumothorax detected on a routine CXR post drain removal.
Characteristics of patients who developed a pneumothorax post drain removal
The age range of patients who developed a pneumothorax post drain removal was 18–81 years. Table 4 presents data on the characteristics of those patients who had a pneumothorax detected on routine post drain removal CXR. Only one patient who developed a pneumothorax was ventilated at the time of drain removal.
Characteristics of post drain removal pneumothoraces.
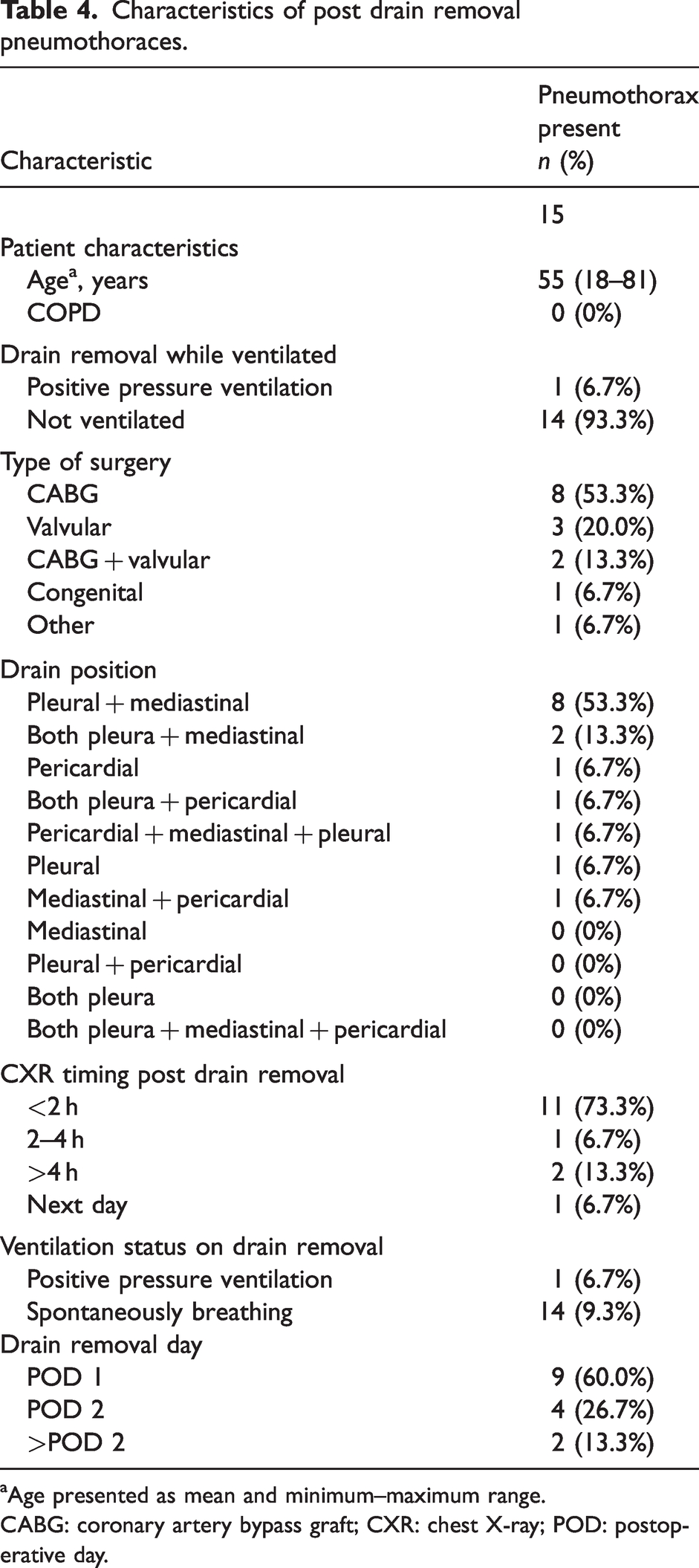
Age presented as mean and minimum–maximum range.
CABG: coronary artery bypass graft; CXR: chest X-ray; POD: postoperative day.
The drain combination of pleural and mediastinal represented 53.3% of the pneumothoraces but was used only 25.4% of the time out of all the participants. The drain combination of pericardial, mediastinal and pleural was utilised 30.3% of the time but represented only 6.7% of pneumothoraces.
Of the 15 pneumothoraces that were present post drain removal, three were right-sided, 11 were left-sided and one was bilateral. All but three had drains in the same pleural space as the pneumothorax and only three of the pneumothoraces had a central line inserted on the same side. None of the patients with a pneumothorax present on post drain removal CXR had a formal diagnosis of COPD. No patient who developed a pneumothorax detected on routine drain removal CXR was symptomatic.
Cost analysis
A total of 158 CXRs were performed specifically for chest drain removal. The cost of an individual mobile CXR as defined by Medicare is A$49.05. A total saving of approximately A$7750 per year could be obtained by omitting these CXRs. The cost associated to diagnose one asymptomatic pneumothorax is A$1275.30 when accounting for all patients. The cost to diagnose one asymptomatic pneumothorax accounting only for patients with at least one pleural drain inserted is A$1094.19.
The time taken to perform a mobile CXR in ICU by the radiographer was approximately 20 min.
Discussion
Diagnosis of a new pneumothorax occurred in 3.8% of patients on routine post drain removal CXR. In all of these cases, the pneumothorax was defined as small using the British Thoracic Society guideline on pneumothorax definition and none of these cases required intervention. In this study, routine post drain removal CXR provided no clinical benefit.
Demographics, cardiothoracic procedure rates and incidence of pneumothorax identified were comparable to previous studies.2,3,8,9,19 ICU LOS appeared to be longer in this study with a median ICU LOS of greater than three days compared with a median of one day reported in other studies.3,19 Despite this difference in ICU LOS, pneumothorax incidence and intervention rate remained comparable. A longer ICU LOS possibly reflects reduced bed pressures throughout a year of fewer surgical procedures being completed as a result of the COVID pandemic. Another potential explanation may be a difference in patient comorbidities, although this data was not obtained for patients in this study.
Interestingly, the chest drain combination of pleural and mediastinal position appeared to be disproportionately represented within the group that had pneumothoraces detected on routine post drain removal CXR. Inadvertent puncture of the contralateral pleura, without drain placement, does not explain this observation as the majority of pneumothoraces detected had a drain in the same side as the pneumothorax. It is possible that this combination of drains is at higher risk for developing a pneumothorax post drain removal; however, further research is required to understand the nature of this relationship.
Although not specifically examined in this study, of the five patients who had drains inserted for a pneumothorax, 66.7% had signs and symptoms present. One of these patients had a drain inserted prophylactically to prevent deterioration and therefore did not develop symptoms. The reliability and safety of signs and symptoms predicting the need for a CXR cannot be commented on based on the results of this study. Although, multiple previous studies have concluded that signs and symptoms are a reliable predictor of the need for intervention and that clinically significant pneumothorax post drain removal does not occur in asymptomatic patients.1,9 –11,14 These studies concluded that omission of routine post drain removal CXR is safe. This study, in combination with current literature, suggests that standardised training in drain removal and close monitoring post drain removal could obviate the need for routine post drain removal CXR.
The potential cost saving as a result of omitting post drain removal CXRs was estimated at A$7750 per year. Additional savings could be calculated by taking into account the cost of the radiographer performing the CXR, additional staff assisting the radiographer to perform the CXR, radiologist time taken to report the CXR and maintenance costs of equipment. This represents a considerable saving to an individual department, as well as a large saving to state health departments if all centres were to omit post drain removal CXRs. It should be noted that the cost saving was calculated only on patients who had two CXRs on the same day with the second CXR being performed specifically for the purpose of routine post drain removal assessment.
There are inconsistencies in the recommended time frame for post drain removal CXR. The current practice of obtaining a CXR 4 h post drain removal at Westmead Hospital does not appear to be evidence based. A study in 2002 examined when the most appropriate timing for a post drain removal CXR should be taken and concluded that a CXR performed within 1–3 h post drain removal effectively identified a pneumothorax in ventilated patients. 20 Currently, timing of post drain removal CXR is often a result of surgeon preference and institutional policy. 1 However, even with a policy of obtaining a CXR 4 h post drain removal, adherence to this was poor with the majority of CXRs in this study obtained within 2 h. This short time interval to routine post drain removal CXR needs to be considered as a possible contributor to finding a reduced incidence of pneumothoraces and finding no clinically significant pneumothoraces. Furthermore, inconsistent clinical practice in the healthcare setting has been shown to reduce patient safety and increase patient morbidity and mortality. 21 Therefore, we should aim to develop policies to standardise care in line with evidence-based practice.
This study suggests that developing a standardised practice of not performing routine CXR post drain removal may result in avoiding unnecessary ionising radiation for patients, avoidance of over-utilising resources and a cost saving of approximately A$7750 each year. It also adds to the evidence base that routine CXR post drain removal in cardiac surgical patients provides limited clinical benefit. Future studies should be conducted to confirm this finding.
Notable strengths of this study include a large population, no missing data from all included subjects and all post drain removal CXRs having a formal report from a qualified radiologist to identify presence of a pneumothorax and eliminate bias from researchers analysing CXRs.
Limitations of this study include being a single centre study with a retrospective design; having limited data on the presence of chronic lung disease; and order form comments potentially impacting interpretation of drain removal CXRs. In addition, having the majority of routine post drain removal CXRs within 2 h limits the interpretability of the data, with the possibility of missing pneumothoraces when the CXR is taken too early. Finally, limited analysis was able to be performed to determine why this patient group had a longer ICU LOS. However, the increased LOS seen within this study did not affect the comparability of results to previous studies.
Conclusion
Despite our local protocol of taking a routine CXR no sooner than 4 h post drain removal, the majority of CXRs were performed within 2 h. This practice did not detect any clinically significant pneumothoraces requiring intervention. This study has indicated a possible avenue for potential cost saving, as well as a pathway to better resource utilisation without compromising patient safety. This study presents data that suggests the routine use of post drain CXRs provides limited clinical benefit and indicates that it may be possible to perform CXRs post drain removal only when clinically indicated. Further risk-stratified studies are needed to identify evidence-based criteria for CXR indication post drain removal and to identify populations at risk of developing a pneumothorax amongst cardiac surgical patients.