
Abstract
We present a case of severe taipan envenoming in northern New South Wales in a 68-year-old man. He developed severe neurotoxicity requiring intubation and ventilation, venom-induced consumption coagulopathy, myotoxicity and thrombotic microangiopathy with acute kidney injury requiring dialysis. He was administered brown and tiger snake antivenom consistent with guidelines and snake occurrence in the region. Taipan venom was detected in serum (72 ng/ml) following concern about the severity of neurotoxicity, clinical toxicology consultation and a concurrent report of a taipan in the area. Based on this it would be prudent to stock and consider treating with polyvalent antivenom in north-eastern New South Wales and south-eastern Queensland.
Introduction
Taipans (Oxyuranus spp.) are large snakes that can cause life-threatening neurotoxic and coagulopathic envenoming (Figure 1). 1 They mainly occur in northern Australia, but have a patchy distribution. Wild taipan bites have not previously been reported south of the Sunshine Coast (half occur in snake handlers). 1 For this reason, taipan or polyvalent antivenom is currently not recommended for venom-induced consumption coagulopathy (VICC) south of the Sunshine Coast, 2 because a combination of brown and tiger snake antivenom has been thought to be adequate.

Image of a coastal taipan (Oxyurnaus scutellatus) from the ‘Gorge’ near Grafton taken by Steve McEwan.
The common important venomous snakes in north-eastern New South Wales (NSW) reported to cause bites are brown snakes (Pseudonaja spp.), rough-scale snakes (Tropidechis carinatus), red-bellied black snakes (Pseudechis porphyriacus) and less commonly tiger snakes (Notechis scutatus) and Stephens banded snakes (Hoplocephalus stephensii), which are all covered by brown and tiger snake antivenoms. However, taipans have been found in north-eastern NSW and south-eastern Queensland for decades.3,4
We report a case of confirmed taipan envenoming presenting with VICC and neurotoxicity in northern NSW.
Clinical case
A 68-year-old man presented to Grafton Hospital with severe envenoming following a snakebite while hiking near the ‘Gorge’ camping ground (approximately 60 km from Grafton). During a solo morning hike in September 2023, he felt something hit the side of his ankle at about 09:30 hours, but dismissed it as a stick. He soon felt dizzy and fell, but was able to walk back to his car. He drove back to the campsite and proceeded to vomit profusely for about 4 hours. He eventually called for help and presented via NSW Ambulance Service to Grafton Hospital emergency department at 18:50 hours, about 9.5 hours post bite. A pressure bandage was applied in the emergency department. His past medical history included hypertension and hypercholesterolaemia.
On examination there were two puncture marks on his right ankle and widespread bruising. He had dysarthria, fixed and dilated (7 mm) pupils, bilateral ptosis, complete external ophthalmoplegia and laboured tachypnoea. Initial laboratory investigations were an international normalised ratio >10, activated partial thromboplastin time >180 s (reference range (RR) 25–37), fibrinogen <0.4 g/l (RR 2.0–4.6 g/l), haemoglobin 175 g/l (RR 130–180 g/l), platelets 180 × 109/l (RR 150–400 × 109/l), creatinine 189 µmol/l (RR 60–110 µmol/l) and creatine kinase (CK) 4911 U/l (RR 40–200 U/l). An indwelling catheter was inserted, with minimal urine output after initial drainage.
His respiratory compromise progressed over the initial hour in the emergency department requiring intubation and invasive ventilation. He was administered one vial of brown and one vial of tiger snake antivenom, post intubation and 11 hours post bite. He was retrieved to Lismore Base Hospital and on admission to intensive care he had no brainstem reflexes or apparent response to the external environment. The following morning, he was able to move his right thumb and so demonstrate awareness and comprehension. He was sedated for comfort, with daily interruption, to assess neurological recovery. Further discussion with a clinical toxicologist (GKI) raised the possibility of this being a taipan bite because of the severity of neurotoxicity and concurrent report of a road-killed taipan near the Gorge, reported by a herpetologist (TT), serum was frozen for taipan venom-specific enzyme immunoassays. 5
The coagulopathy resolved over 24 hours (Figure 2(a)), but he developed mild thrombocytopenia (Figure 2(b)) and red cell fragments on his blood film consistent with thrombotic microangiopathy. 6 The CK peaked at 15,337 U/l, but the creatinine continued to increase (Figure 2(c)) with anuria consistent with stage 3 acute kidney injury due to the thrombotic microangiopathy. Continuous renal replacement therapy commenced on day 2, transitioning to intermittent haemodialysis which continued until day 12. The paralysis improved and he was extubated on day 6. He was discharged home 16 days post bite with a creatinine of 410 µmol/l, which improved to 203 µmol/l, 6 weeks post discharge.
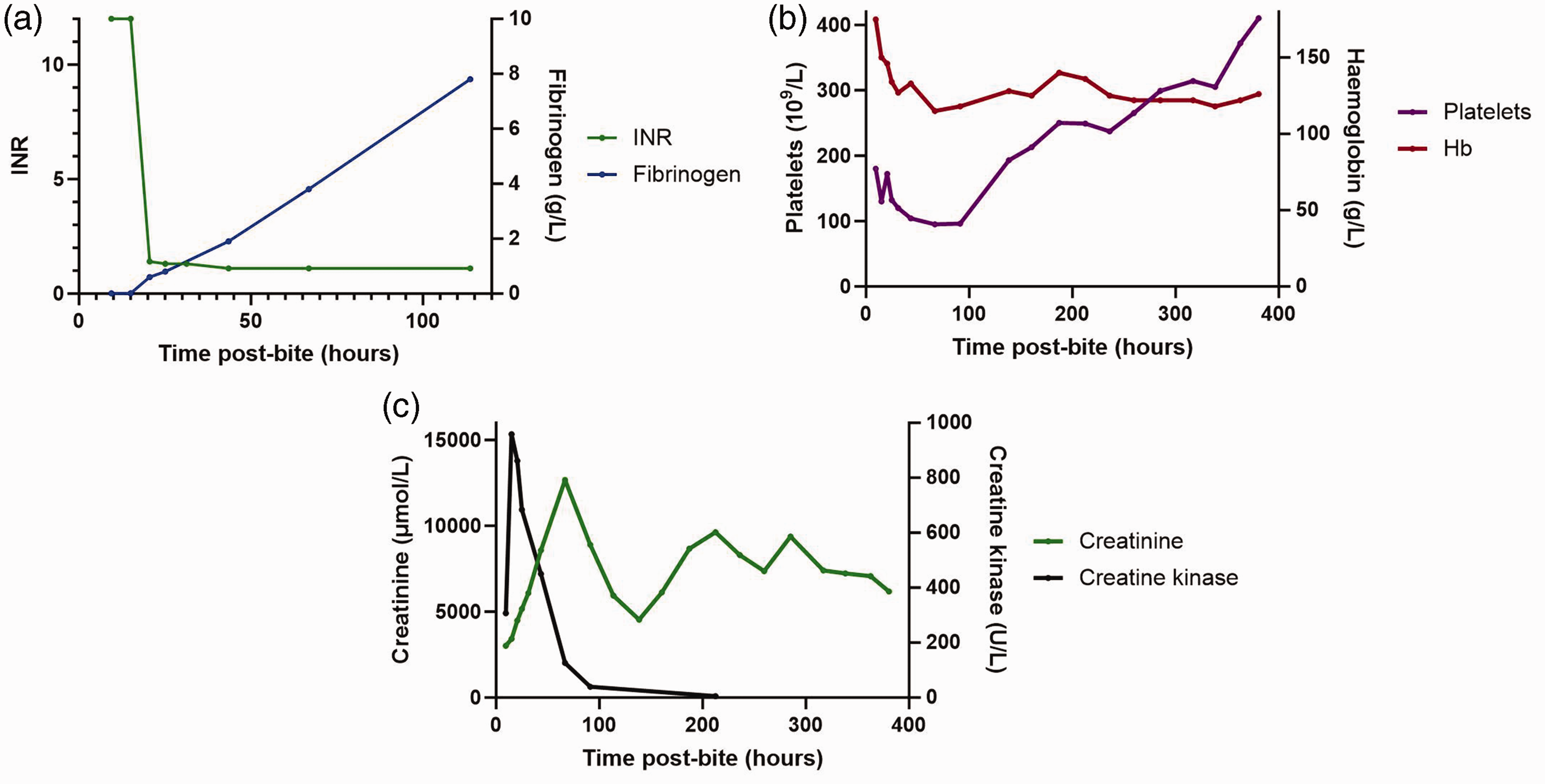
Plots of laboratory investigations over time: (a) international normalised ratio (INR) and fibrinogen (g/l); (b) haemoglobin (Hb g/l) and platelets (109/l); and (c) creatinine (µmol/l) and creatine kinase (U/l).
Serum taipan venom concentration was 72 ng/ml, 11 hours post bite. Informed consent to publish the details in this case report and permission to collect blood for the venom assay was obtained from the patient as part of the Australian Snakebite Project.
Discussion
We present a confirmed taipan envenoming south of Queensland, with severe neurotoxicity requiring intubation and mechanical ventilation, VICC, myotoxicity and thrombotic microangiopathy, with an acute kidney injury requiring dialysis. Brown and tiger snake antivenom were administered, but the lack of response is more likely to be due to the delay in antivenom, rather than taipan or polyvalent antivenom not being used.
Exact confirmation of the snake type causing envenoming is less important for antivenom administration than covering the likely snake groups involved, based on local snake distribution and the envenoming syndrome. 2 Brown and tiger snake antivenom were administered in this case to cover the local fauna known to cause VICC and neurotoxicity. However, the severity of the neurotoxicity in this case, and the report of a taipan being found near to the locality of the bite, was more consistent with taipan envenoming. This was confirmed by the measurement of a high taipan venom concentration, 72 ng/ml, based on a previous series in which the median taipan venom concentration was 8.4 ng/ml (interquartile range 3–30 ng/ml). 1
Antivenom stocking, like any antidote, is an ongoing issue because of cost, requirement for administration within hours of a bite and the uncommonness of snake envenoming. 5 Antivenom administration only requires the healthcare team to be able to treat an allergic reaction, so should be available in every hospital, even if there is subsequently transfer to a larger hospital. For the majority of Australia, a combination of brown and tiger snake antivenom covers 86% of snakebites—brown snake (Pseudonaja spp.), tiger snake (Notechis scutatus), rough-scaled snake (Tropidechis carinatus), broad-headed snakes (Hoplocephalus spp.) and red-bellied black snakes (Pseudechis porphyriacus) 7 – which was the reason for their administration in this case. Stocking of polyvalent antivenom is more problematic as it is more expensive, and is only required for the minority of cases, 2 but is recommended for taipan bites in regions where the snake is commonly reported, 1 mainly northern Queensland.
This case raises an important issue for antivenom treatment and stocking in hospitals south of the Sunshine Coast, including northern NSW. It would be prudent to stock and consider treating with polyvalent antivenom in north-eastern NSW and south-eastern Queensland, because of the small but important risk of taipan bites. Currently polyvalent antivenom is stocked in major hospitals to cover other uncommon snakes, such as death adders and mulga snakes, as well as snakes held in captivity outside their normal distribution. Therefore, having polyvalent antivenom available for taipans in these regions south of the Sunshine Coast would be feasible.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the search, authorship and/or publication of this article.