
Abstract
Two recent cases of central retinal artery occlusion under otherwise uncomplicated sub-Tenon’s block that resulted in significant visual loss after cataract surgery prompted us to undertake a literature review of such cases. We identified 97 cases of retinal artery occlusion after ophthalmic surgery under regional anaesthesia that had no immediate signs of block-related complications. These occurred after various intraocular (87%) and extraocular (13%) operations, across a wide range of ages (19–89 years) on patients with (59%) or without (39%) known risk factors. The anaesthetic techniques included 40 retrobulbar blocks, 36 peribulbar blocks, 19 sub-Tenon’s blocks, one topical anaesthetic and one unspecified local anaesthetic. Different strengths of lidocaine, bupivacaine, mepivacaine and ropivacaine, either alone or in various combinations, were used. The details of the anaesthetic techniques were often incomplete in the reports, which made comparison and analysis difficult. Only nine cases had their cause (optic nerve sheath injury) identified, while the mechanism of injury was unclear in the remaining patients. Various mechanisms were postulated; however, the cause was likely to be multifactorial due to patient, surgical and anaesthetic risk factors, especially in those with compromised retinal circulation. As there were no definite risk factors identified, no specific recommendations could be made to avoid this devastating outcome. We have provided rationales for some general considerations, which may reduce this risk, and propose anaesthetic options for ophthalmic surgery on the fellow eye if required, based both on our literature review and our personal experience.
Introduction
Retinal artery occlusion (RAO) refers to compromised blood supply to the retina, resulting in retinal and disc infarction and leading to partial or complete loss of central vision.1,2 The causes include embolic (e.g. atrial fibrillation, ipsilateral carotid plaque), vasculitis (e.g. giant cell arteritis, other autoimmune vasculitis), and iatrogenic (e.g. cosmetic facial injections, 3 periocular triamcinolone injection,4,5 and ophthalmic block).6,7
We recently encountered two cases of central retinal artery occlusion (CRAO) under sub-Tenon’s block which unfortunately resulted in significant visual loss after cataract surgery. There were no immediate signs of block-related complications or surgery-related complications. Fundoscopy was not performed during the procedures. The eyes were covered with an eyepad overnight and CRAO was only discovered on the first postoperative day when the patients returned for follow-up review. While a thromboembolic event related to their pre-existing atrial fibrillation was suspected and a cardiac source was excluded, no cause could be confirmed despite extensive investigations. Discussions among anaesthetist colleagues revealed that there was a gap in the knowledge about this condition. We have therefore undertaken a comprehensive review of this rare but catastrophic outcome. This narrative review describes RAO associated with ophthalmic surgery under regional anaesthesia, including relevant anatomy of retinal arteries, incidence, risk factors, mechanisms, presentation, diagnosis and management. We did not include RAO cases under general anaesthesia alone. We have also made some general recommendations that may influence this risk when performing an ophthalmic block and discuss anaesthetic options for ophthalmic surgery on the fellow eye if required.
Methodology
A literature review was conducted using PubMed, Google Scholar, Medline and Scopus with the aim of identifying English language publications between January 1980 and December 2022. The keywords searched were ‘retinal artery occlusion’, ‘regional anaesthesia’, ‘local anaesthesia’ and ‘ophthalmic block’, in various combinations. Our search included prospective randomised controlled trials, case series, case studies, and opinion articles. Further related articles were retrieved from the references of key articles. There were no prospective randomised controlled trials found. Each case from the identified articles (case series, case studies and opinion articles) was screened. We included all the cases of RAO after ophthalmic surgery under regional anaesthesia, and excluded any cases that had immediate clinical signs of block-related complications, for example, retrobulbar haemorrhage or globe perforation.
Retinal artery circulation
The central retinal artery arises from the ophthalmic artery, which is the first branch of the internal carotid artery. It runs inferior to the optic nerve sheath before it enters the sheath 10–15 mm behind the globe. It supplies the inner layers of the retina that contain cones and rods. There are other branches of the ophthalmic artery, including long, short, and lateral posterior ciliary arteries, which supply the outer layers of the retina containing the photoreceptors (Figure 1). 2 A cilioretinal artery is present in about 30% of eyes and supplies the fovea which is critical for central vision.2,8 The cilioretinal artery originates from the short posterior ciliary arteries and not the central retinal artery.
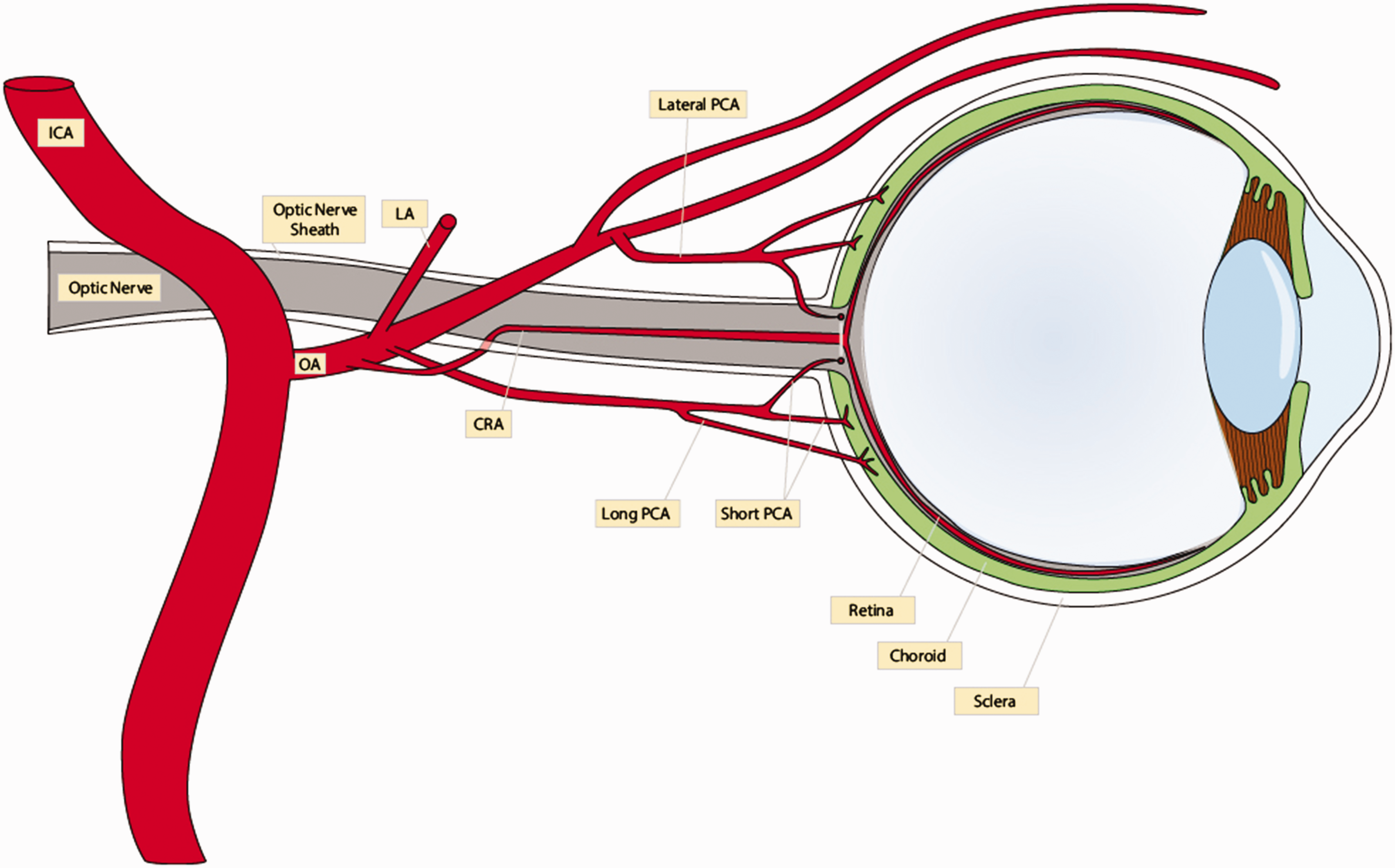
Arterial blood supply to the retina. CRA: central retinal artery; ICA: internal carotid artery; LA: lacrimal artery; OA: ophthalmic artery; PCA: posterior ciliary artery.
The mean (standard deviation) central retinal artery systolic pressure is 54 (14) mmHg while normal intraocular pressure (IOP) ranges from 10 to 21 mmHg.9,10 The pressure gradient enables adequate ocular perfusion. Any causes that reduce central retinal artery pressure or increase IOP could potentially compromise ocular perfusion.
Retinal artery occlusion
RAO includes occlusion of the central retinal artery, branches of retinal artery, or cilioretinal artery. Of these, CRAO is the most commonly encountered. Its incidence increases with age but is overall rare, approximately 1.9 per 100,000 people annually.2,8 Typically, it presents as sudden, painless loss of vision in the affected eye. If a cilioretinal artery is present, central vision may be preserved but peripheral vision is severely impaired. 2
Risk factors include carotid artery disease (e.g. stenosis, thrombus, dissection), cardiac disease (e.g. hypertension, arrhythmia [especially atrial fibrillation], valvular disease, heart failure), haematological disorders (e.g. sickle cell haemoglobinopathy, leukaemia, non-Hodgkin’s lymphoma), diabetes, renal failure, obesity, hypercholesterolaemia and smoking.2,11 The visual outcome may vary but fewer than 20% of patients regain functional vision in the affected eye.2,12
Retinal artery occlusion after ophthalmic surgery under regional anaesthesia
Incidence, demographics, and risk factors
We identified 97 cases of RAO after ophthalmic surgery under regional anaesthesia, including two cases of recurrent RAO after a second ophthalmic block,13,14 which fulfilled our search criteria. Our search only included those without immediate signs of block-related complications, and under-reporting is common in the literature, thus the actual number of cases may be higher. Due to the wide variety of details included in reports, the numbers reported in each variable do not always add up to 97. In a large one-year survey on complications of local anaesthesia in cataract surgery, there was one case of cilioretinal artery occlusion reported among 180,000 sub-Tenon’s blocks. 15
Transient RAO, however, may be more common but not recognised. One author examined the fundus of every eye that received regional local anaesthetic injection over a 10-year period and reported two cases of transient RAO without sequalae among 335 sub-Tenon’s blocks. 16
Reported cases included a similar number of men (49) and women (45) affected, with ages ranging from 19 to 89 years. The majority were older than 60 years (55%), which is likely to be a reflection of cataracts (59% of the operations) being the most common eye surgery performed worldwide and predominantly an age-related health problem. 17 Fifty-seven patients had one or more risk factors. Alarmingly, 38 patients had no risk factors. However, given the very low incidence of RAO under regional anaesthesia and the high incidence of the risk factors mentioned in elderly patients, knowledge of the risk factors would be unlikely to facilitate prediction or prevention in most cases.
Characteristics of the surgery and regional anaesthesia
Most of the operations (87%) were intraocular procedures, including cataract surgery, complicated cataract surgery requiring anterior vitrectomy because of posterior capsule rupture, vitreoretinal surgery, glaucoma surgery, photocoagulation, or Descemet membrane repositioning. Extraocular procedures accounted for 13%, including pterygium removal, scleral buckle surgery, strabismus correction and radial keratotomy. The IOP was reported as normal in 38 patients and elevated (22–48 mmHg) in six patients at the time of diagnosis.
RAO appeared to be unrelated to the type of regional block: the reported cases occurred in relation to retrobulbar blocks (40/97, 41%)5,7,13,14,18 –33 (Supplementary Table 1), peribulbar blocks (36/97, 37%)27,32,34 –42 (Supplementary Table 2), sub-Tenon’s blocks (19/97, 20%)16,32,39,43 –49 (Supplementary Table 3), one topical local anaesthetic (1/97, 1%) 50 and one unknown local anaesthetic technique (1/97, 1%), 51 which contained no anaesthetic details.
It is not possible to compare and analyse the occurrence of RAO related to different ophthalmic regional anaesthetic techniques from the literature. There are too many variables, including the type of block, insertion site, needle trajectory, insertion depth, injecting speed, volume administered, method and duration of ocular compression, and any difficulty encountered, as well as individual variations in orbital anatomy. Nothing short of a video replay of the actual block would allow adequate comparison and appraisal. 52 Furthermore, these details were often incomplete in the reports.
There was a combined total of 76 retrobulbar and peribulbar blocks: 19 cases used a long needle of 35–38 mm and two cases used a shorter needle of 22–25 mm. A sharp needle tip was involved in 32 cases, while a short-bevel needle tip (often described as ‘blunt’ or ‘Atkinson needle’ in the reports) was used in 11 cases. ‘Difficulty’ during insertion or injection was reported in two cases.
Different strengths of amide local anaesthetics, including lidocaine (2–4%), bupivacaine (0.25–0.75%), mepivacaine (2%), and ropivacaine (0.75–0.8%), either alone or in various combinations, were administered. The most frequently used agents were lidocaine (35/97, 36%) and a lidocaine–bupivacaine mixture (28/97, 29%). The case of topical anaesthesia involved proparacaine 0.5% (commercial preparation contains preservative benzalkonium chloride). Parahydroxybenzoate (better known as methylparaben), a preservative, was involved in eight cases, while there was no specific mention of this in the remaining cases. We therefore assumed the remaining local anaesthetics were preservative-free preparations, as these were the most common forms used clinically in regional anaesthesia.
Among the 40 cases of retrobulbar block, 2–4 ml local anaesthetic was used in 21 patients, whereas 5 ml or greater (range 5–7 ml) was used in nine patients. Among the 36 cases of peribulbar block, 2–7 ml of local anaesthetic was used in 31 patients, whereas more than 10 ml (range 13–17 ml) was used in three patients. Among the 19 cases of sub-Tenon’s block, 3–5 ml of local anaesthetic was used in 16 patients, whereas 6 ml was used in two patients.
Only six cases involved adrenaline-containing local anaesthetic, whereas 82 cases used adrenaline-free local anaesthetic. Intracameral adrenaline (0.1 ml of 1:100,000 = 1 µg) was administered to six cases during complicated cataract surgery.
Hyaluronidase was an adjuvant to the local anaesthetic in 32 cases, whereas 41 cases did not include it as an additive. Ocular compression after regional anaesthesia, using either manual massage or an ocular compression device, was applied in 25 patients and was not used in 24 cases.
Mechanisms
The duration of arterial occlusion is a crucial factor influencing the eventual retinal damage and visual outcome. In an animal study, no damage was found if the occlusion was less than 97 min and irreversible damage occurred after 240 min. 53 However, in a review article, Tobalem et al. argued that the animal study produced only partial occlusion of retinal circulation. In addition, they concluded that as little as 12–15 min of complete CRAO may result in retinal infarct. 54
The exposed section of central retinal artery before it enters the optic nerve sheath is potentially more vulnerable to direct needle trauma. 13 Although direct injury cases were often associated with immediately detectable retrobulbar haemorrhage, 19 one reported case had no signs of retrobulbar haemorrhage at the time of surgery. 24 It had been demonstrated that the tip of various sub-Tenon’s cannulas (length 22–25 mm) could reach the optic nerve without advancing the cannula hub to the limbal insertion site, which was 5–8 mm further away from the usual conjunctival insertion point for a sub-Tenon’s block. 55 Short posterior ciliary arteries cross the sub-Tenon space close to the optic nerve head and are vulnerable to damage by metal cannulas that are inserted very posteriorly. 56 Vasospasm, induced by direct touching from the needle/cannula, local anaesthetic injection or adrenaline, has been postulated as another mechanism. 13
Compression within the optic nerve sheath (by injectate or haematoma) could lead to CRAO. In a cadaver study, with the eye at the superonasal position, the optic nerve sheath could be penetrated with ‘only moderate resistance’ by a 38 mm needle without the needle hub reaching the inferior orbital rim. 57 As the tip of a sub-Tenon’s cannula, including the tri-port cannula used for the incisionless technique, could reach the optic nerve, 55 it would be possible that the cannula could also pierce through the optic nerve sheath. 56 Combined CRAO and central retinal vein occlusion have been reported, as occluding the central retinal vein within the optic nerve sheath can result in secondary CRAO. 11 There were nine confirmed cases of optic nerve sheath injury after retrobulbar or peribulbar block leading to CRAO.7,20,21,23,24,31
While adrenaline could theoretically be implicated, the majority of RAO cases did not involve adrenaline-containing local anaesthetic. In one study, retrobulbar block with 4.5 ml of adrenaline-containing local anaesthetic resulted in a 50% reduction in ophthalmic artery pulse pressure. 58 Intraocular irrigation solution containing adrenaline (typical concentration 1 µg/ml) has been widely used during cataract surgery to maintain mydriasis. Complicated cataract operations also required additional intracameral adrenaline. 41
Clinical studies have demonstrated that a significant decrease in ocular pulse amplitude (pulsatile flow) occurred after retrobulbar, peribulbar or sub-Tenon’s block, often in the absence of an IOP elevation.59 –61 This could be minimised by using a smaller volume of local anaesthetic. 62 Large local anaesthetic volumes (retrobulbar block ≥5 ml; peribulbar block ≥10 ml; or sub-Tenon’s block ≥6 ml) were used for only 14 cases of RAO. Vasoconstriction induced by local anaesthetic has been postulated as the mechanism for the reduction in pulsatile ocular blood flow, although the exact effect of local anaesthetic on retinal vessels is currently unknown. Local anaesthetic toxicity to the retina is unlikely, as the safety of intracameral preservative-free lidocaine and bupivacaine has been established. 63 Hyaluronidase, an adjuvant to the local anaesthetic, may offer partial protection against the reduction of pulsatile ocular blood flow. 64 It causes reversible polymerisation of hyaluronic acid to a tetrasaccharide in the interstitial cells, thus increasing membrane permeability, tissue diffusion and the resorption rate of excess fluid. 65
Prolonged raised IOP (from any cause) has been postulated as a mechanism for RAO. IOP during and after surgery was unknown. In addition, IOP was often not elevated at the time of presentation. A localised compartment syndrome (local anaesthetic injectate forms a loculated ‘cyst’ that compresses one or more of the retinal arteries) has been postulated as another possible explanation.13,28 Ocular compression, with a Honan’s balloon at 30 mmHg for 10 min, could effectively reduce the raised IOP and the decrease in ocular blood flow after an ophthalmic block.66,67 We believe that external compression, however, effectively further reduces ocular perfusion during the compression period, and could be potentially dangerous if the device is inadvertently left for an extended period.
Tappeiner and Garweg reported six cases (incidence of 4.3%) of RAO in patients given parahydroxybenzoate-containing mepivacaine retrobulbar blockade, compared with no cases using preservative-free mepivacaine, 25 suggesting possible toxic effects from the preservative. The manufacturer has since included vaso-occlusion as a potential risk and contraindication in its retrobulbar application. 25 There were two other reported cases of RAO associated with preservative-containing local anaesthetic in another study. 28
Within a 2-month period, 14 patients with CRAO following cataract surgery complicated with anterior vitrectomy under peribulbar block were reported. 41 The vitrectomy probes were sterilised by ethylene oxide and left for 12 h aeration before use, in accordance with the manufacturer’s recommendations. The authors postulated that the toxic effect from residual ethylene oxide was responsible for their CRAO. 41 The local protocol has since been modified with an increased aeration period to 48 h and rinsing the instrument thoroughly before use, and no further cases of CRAO were diagnosed in the following 6 months.
There was one case of CRAO reported on a healthy 60-year-old patient following pneumatic Descemetopexy (Descemet membrane reposition by intracameral air) after cataract surgery one day earlier. 50 The intracameral air bubble was partially released after 2 h. There were no reported signs of raised IOP (e.g. headache, eye pain, nausea or vomiting) during the immediate postoperative period. Both procedures were performed under topical proparacaine. The authors postulated that the cause of CRAO was most likely related to intracameral air causing pupillary block leading to a sudden IOP elevation and was unrelated to the anaesthesia.
Some ophthalmic operations are at higher risk of transient IOP spikes, in particular when gas, air or viscoelastic is retained in the eye. Ten cases of RAO, unrelated to regional anaesthesia, were reported in patients undergoing ophthalmic operations, including cataract, vitrectomy and scleral buckle surgery, over a 20-year period. 68 Every patient except one had at least one pre-existing risk factor. All cases involved general anaesthesia with well-controlled blood pressure during their procedures, and more importantly, no ophthalmic block was administered. The authors postulated that surgical manipulations caused elevation in IOP and a decrease in ocular perfusion, and in the presence of pre-existing risk factors, led to ocular vascular occlusion.
Presentations
The diagnosis of RAO was recognised on the same day of surgery in 13 patients,8,26,67 on postoperative day one in 54 cases,16,18,22,24 –27,29 –42,44 –46,48,51 and delayed (range 2–30 days after surgery) in 28 patients.7,21,23,25,27,41,46 Most RAO cases were recognised on postoperative day one as fundus examination is not routinely performed in most ophthalmic operations. There are many possible explanations for the longer delayed presentation (>1 day). Patients might not recognise their own symptoms as some practices used telephone consultation for immediate follow-up, and transient blurred vision was common after certain ophthalmic operations. 69 Toxic effects, rather than vasospasm or direct injury, might also account for some delayed presentations.25,41 Back pressure from initial central retinal vein occlusion leading to secondary CRAO has also been postulated for delayed presentation. 23
Diagnosis
The diagnosis of RAO is primarily based on clinical findings and the characteristic appearance of the retina. The typical fundoscopic findings are retinal whitening (retinal oedema) and a cherry red spot (preserved choroidal circulation underlying the fovea that is surrounded by pale, ischaemic retina). Fundus fluorescein angiography often shows sluggish or no flow in the affected retinal arteries, 70 while optical coherence tomography may reveal a thickening of the inner retinal layer. 71 B-scan ocular ultrasonography, computer tomography and magnetic resonance imaging may help in diagnosing the cause of injury. In addition, these patients should undergo a thorough evaluation of general risk factors, including cardiac, neurological and other medical comorbidities.2,70 These screening tests may assist in the management and prevention of future episodes if RAO is coincidental and not related to regional anaesthesia.
Management of retinal artery occlusion
An ophthalmologist experienced in managing RAO should be consulted immediately for timely intervention and management of RAO, aiming to restore blood flow to the affected retina, alleviate symptoms, and minimise long-term visual damage. Gentle massage of the globe and digital pressure on the closed eyelids may dislodge an embolus causing the blockage and restore blood flow. However, these manoeuvres may not be possible if there is an unsutured wound. Wound burping via paracentesis would be a useful immediate option to reduce anterior chamber pressure. Further, lowering IOP by topical carbonic anhydrase inhibitors, hyperosmotic agents, beta-blockers, prostaglandin analogues etc. may improve blood flow to the retina.2,8,72
Anticoagulant or antiplatelet agents may be useful if thrombosis or embolism is suspected. Hyperbaric oxygen therapy may increase oxygen delivery to the ischaemic retina and minimise retinal damage.2,8,72 More advanced interventions such as intra-arterial thrombolysis and retrobulbar acetylcholine injection have been trialled. Current therapeutic options, however, are likely to be ineffective as the majority of RAO cases were diagnosed well beyond the potential reversible period of retinal ischaemia.2,11
Visual outcome
It is worth noting that the severity and permanence of visual loss in RAO can vary. Early intervention is crucial to restore blood flow and minimise retinal damage. However, even with prompt treatment, some cases may result in permanent vision loss. Among the 97 reported cases, 73 patients were ‘legally blind’ (defined as visual acuity 6/60 or worse) in their affected eyes.
Suggestions to minimise the risk of retinal artery occlusion following ophthalmic surgery under regional anaesthesia
There were no definitive risk factors identified in our review for RAO following ophthalmic surgery under regional anaesthesia. We are therefore unable to offer specific recommendations to minimise this catastrophic complication. As this complication is extremely rare and there is a lack of definite causation, any departure from the current routine safe practice may not be warranted. Based on our literature review and our personal experience, we provide a rationale for and propose the following general recommendations in relation to RAO.
Use a shorter needle for needle-based blocks (length ≤25 mm). There were 19 cases of RAO involved using a long needle of 35–38 mm while only two cases involved using a shorter needle of 22–25 mm. The shorter needle would potentially reduce the incidence of RAO as well as other complications such as globe perforation and optic nerve injury. Posterior cannula placement in sub-Tenon’s block should be avoided. The equator on average is 12 mm from the corneal apex. The cannula tip should be advanced until it just passes the equator of the globe. Very posterior placement of the cannula could potentially pierce the optic nerve sheath, damage the short posterior ciliary arteries, or induce vasospasm by touching. Avoid adrenaline or preservative-containing local anaesthetic agents. Adrenaline induces vasospasm while its preservative has been implicated as the cause of RAO. Hyaluronidase may offer partial protection. It has been shown to minimise the reduction in pulsatile ocular blood flow. Stop injection if unusual resistance or difficulty is encountered! This may indicate that the needle tip is within the optic nerve sheath or inside the globe. Limit the local anaesthetic volume. Use a lower but effective volume for the surgery concerned. Larger volumes cause a higher IOP, which may lead to impairment of ocular perfusion and extrusion of ocular content during intraocular surgery. Limit the pressure (≤20 mmHg) and duration (≤3 min) of ocular compression applied. Repeat, if necessary, after at least one min to allow ocular perfusion. In our experience, one minute or less compression is often sufficient to ‘soften’ the globe for surgery after an ophthalmic block. High pressure and prolonged ocular compression can, in theory, impair ocular perfusion. IOP should be checked after surgery in high-risk cases. Wound burping provides temporary IOP reduction that lasts 15 min. Oral acetazolamide and intravenous mannitol should be considered if there is sustained high IOP (≥40 mmHg).
Anaesthetic considerations for fellow eye in patients who have had RAO
After a second retrobulbar block, recurrent RAO has been reported in two patients without a proved cause determined.13,14 We believe that it is, therefore, prudent that ophthalmic block, either the same or another type, is not used again for the fellow eye. The patient’s cardiac status should be optimised. Topical anaesthesia or general anaesthesia may be more appropriate because it may minimise the potential medicolegal issues if RAO recurs on the fellow eye. In addition, both these anaesthetic options have little to no local effect on the orbital structures, and they allow early postoperative visual assessment. IOP should be checked and monitored up to 2 h after surgery. Prophylactic acetazolamide should be considered to prevent postoperative IOP spikes. We have successfully used topical anaesthesia for one of our patients for cataract surgery in his fellow eye.
Conclusion
The exact mechanism of RAO after ophthalmic surgery under regional anaesthesia remains unclear in most reported cases. It is likely to be multifactorial due to patient, surgical and anaesthetic risk factors, especially in those with compromised retinal circulation. The final visual acuity is often significantly impaired. It is, therefore, of paramount importance to continue to explore, understand, and hopefully minimise this catastrophic outcome.
Footnotes
Acknowledgements
The author(s) wish to thank Mr Eugene Mak, Sydney, for his assistance with the illustration.
Author Contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the search, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.