
Abstract
Anaesthesia for caesarean section occurs commonly and places specific demands on anaesthetists. We analysed 469 narratives concerning anaesthesia for caesarean section, entered by Australian and New Zealand anaesthetists into the webAIRS incident reporting system between 2009 and 2022. As expected, compared with the remaining 8978 database entries, the 469 incidents were more likely to be emergency cases (relative risk (RR) 1.95), more likely to occur between 18:00 and 22:00 hours (RR 1.81) and between 22:00 and 07:59 hours (RR 4.40) and more likely to be undertaken using neuraxial anaesthesia (RR 9.18). Most incidents involved more than one event. The most commonly reported incidents included intraoperative neuraxial anaesthesia complications (180, 38%), medication errors or issues (136, 29%), equipment issues (49, 10%), obstetric haemorrhage (38, 8%), maternal cardiac arrests (28, 6%), endotracheal tube issues (28, 6%) and neonatal resuscitation (24, 5%). Inadequate neuraxial block, reported in 95 incidents, was the most common intraoperative neuraxial complication. Allergic reactions, reported in 30 incidents, were the most common medication issue, followed by 17 associated with oxytocin and 16 syringe swaps. Thirty-eight reports included significant maternal haemorrhage, with eight of those incidents including maternal cardiac arrest. There was one maternal death and eight incidents with neonatal deaths reported, affecting nine neonates. Problems with intraoperative neuraxial anaesthesia were the most commonly reported events. Implementation of specific strategies are encouraged to enhance preparation for conversion to general anaesthesia and to mitigate medication errors, particularly those relating to oxytocic use and neuraxial anaesthesia medications.
Keywords
Introduction
Providing anaesthesia for caesarean section (CS) is known for its complexities. Births occur 24 hours a day, ranging from elective to time-critical presentations. 1 Compared with other subspecialties, there are high rates of neuraxial anaesthesia use, 2 additional consideration of fetal wellbeing and frequently supporting persons within the operating theatre. Similar to other subspecialties, care involves a multidisciplinary team and increasingly comorbid patients, including pregnancy-specific conditions. 1
In 2020, Australian anaesthetists provided care for 108,000 women who gave birth by CS, 2 with 95% of those patients receiving neuraxial anaesthesia. Between 2009 and 2022, the webAIRS incident reporting system has recorded nearly 10,000 incidents, including those related to patients undergoing elective and emergency CS. We report here an overview of these incidents, to share the experiences of anaesthetists who have reported clinical challenges in providing anaesthesia to patients for CS. The features of these incidents were categorised, and characteristics compared with those of the remaining incidents in the database. The aim is to highlight factors that are specific to anaesthesia for CS and improve patient safety through the reporting of these incidents.
Materials and methods
The webAIRS reporting database is a voluntary reporting system available to anaesthesia clinicians registered with the Australian and New Zealand College of Anaesthetists, Australian Society of Anaesthetists and the New Zealand Society of Anaesthetists. Incidents have been entered into the database since September 2009 and some data we are presenting have been previously analysed and published. 3 , 4 Data relating to clinical incidents are entered into the database, with no identifying clinician or patient details. Incidents range from difficult cases, near misses and workload issues, to significant clinical incidents with patient harm or death. Due to the voluntary nature of reporting, the database can provide neither accurate numerator nor denominator data and therefore the analysis of these incidents does not suggest the frequency with which an outcome may occur in Australia and New Zealand. The database complies with the requirements of the National Health and Medical Research Council regarding the collection and use of de-identified data for quality assurance purposes, 5 and the data management processes have undergone ethical assessment (HREC/11/QRBW/311; HREC/12/NEPEAN/18; MEC/09/17/EXP). 6 , 7
An administration officer or data analyst of the Australian and New Zealand Tripartite Anaesthetic Data Committee removes duplicate, test or empty records as part of the routine data cleaning process. The narratives relating to the incidents in the cleaned database were searched for the term/fragments ‘Cesar, Caesar, LSCS, LUCS’. Incidents were also included if the ‘procedure’ or ‘sub-category’ was listed as ‘caesarean section’, then MDC and VAE analysed each record to determine inclusion. Incidents were included if they involved a CS procedure or an immediate postoperative complication of a CS. Incidents that focused on neonatal resuscitation as the primary event were only included if anaesthesia staff were required to undertake the resuscitation. In an iterative process, VAE read the narrative entry of each incident, applying categorisation which was agreed with MDC. The list of categories evolved as review of the narratives proceeded. Each incident was able to be assigned to more than one category when multiple events occurred. The ability to draw conclusions was limited to the information provided in the narrative by the entering clinician. When possible, definitions were applied. Incidents were defined as a cardiac arrest if they were coded as such by the reporter, or if the narrative described ventricular tachycardia, ventricular fibrillation, asystole, pulseless electrical activity, or when cardiopulmonary resuscitation (CPR) was commenced. If the narrative described near cardiac arrests in which neither CPR nor direct current counter shock were applied, they were categorised as ‘peri-arrests’. Neonatal resuscitation was categorised as primarily cardiac if CPR and/or asystole were documented, or primarily respiratory if intubation and/or other respiratory supports were documented. The frequency with which each category was reported was identified using structure query language (SQL) of the initial categorisation and presented as number (percentage) of the total number of CS reports. We calculated the proportion of overall incidents, with the numerator, the number of incidents meeting inclusion criteria and the denominator, the overall number of incidents in the webAIRS database, at the time of CS incident selection. Further detail (subcategorisation) of the categories that were assigned to over 5% of incidents was undertaken.
The final group of included incidents was compared with the remaining incidents in the webAIRS database according to patient, procedure and clinician characteristics; that is, the comparator group with which comparisons were made all had an incident. The dataset used by webAIRS is available to view online. 8 Procedure characteristics included: the urgency of the case (elective or emergency), the time of day of the incident (08:00 to 18:00 hours, 18:00 to 22:00 hours, 22:00 to 07:59 hours), and the use of neuraxial anaesthesia technique. When a case was started under neuraxial anaesthesia and was converted to general anaesthesia, both techniques could be recorded. Patient characteristics included: age in years, body mass index according to World Health Organization classification, 9 American Society of Anesthesiologists physical status (ASA PS) score of 1–5, 10 and the final outcome of incident (death, permanent disability, temporary disability, not affected by incident, not specified). Pregnancy was specifically identified as a score of 2 in the 2014 version of the scoring system. 11 Clinician characteristics included: seniority of the clinician making the entry (specialist, specialist (FANZCA), non-specialist, post-fellowship examination trainee, trainee year 1–2, trainee year 3–4); clinician hours on duty (0–<10, 10–<16, 16–<24, ≥24) and clinician ‘hours since an 8-hour break’ (0–<10, 10–<16, 16–<24, ≥24).
We calculated the relative risk (RR) for each of these characteristics as the proportion with that characteristic among the CS incidents, divided by the proportion with the characteristic occurring in the remaining incidents in the database, and included the 95% confidence interval (CI), as in previous webAIRS publications. 7 , 12 , 13 It is acknowledged that both the numerator and the denominator are subject to the voluntary nature of the reporting system. The RR refers only to whether or not the characteristic was more common in the CS incidents compared with other incidents unrelated to CS.
Results
A total of 500 incidents were identified during the initial search, with 469 meeting the criteria for inclusion (Figure 1). These were entered between 15 September 2009 and 4 January 2022, comprising 5% of the 9447 incidents within the database at that time. Over that 13-year period, the annual number of CS incidents reported to webAIRS increased from 24 in 2010, peaked at 71 in 2020, with 38 reported in 2021 (complete years reported only, Figure 2).
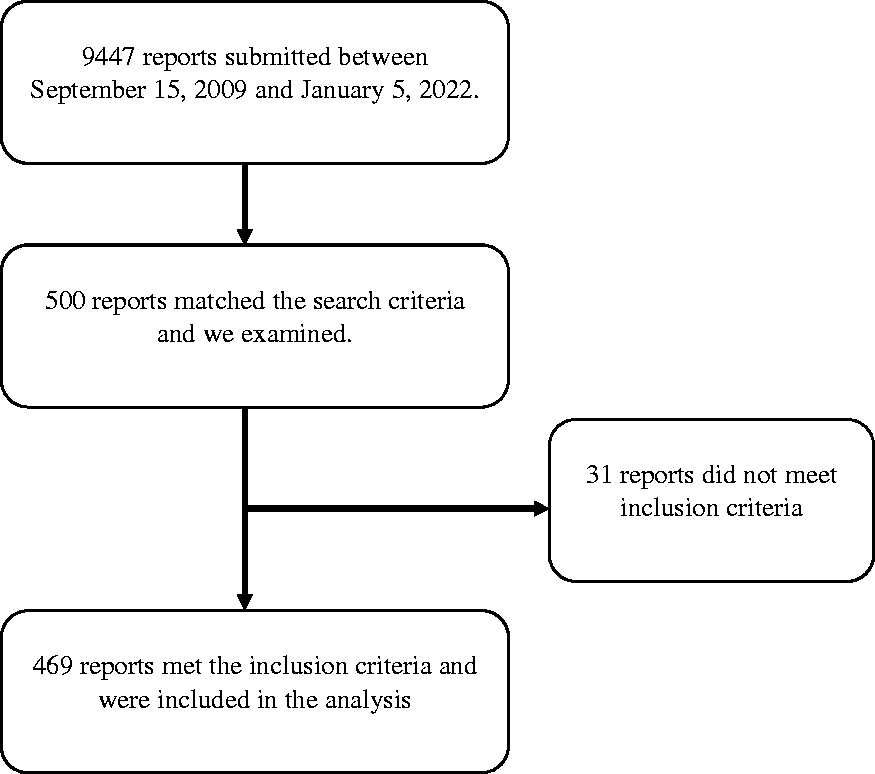
Strengthening the reporting of observational studies diagram.
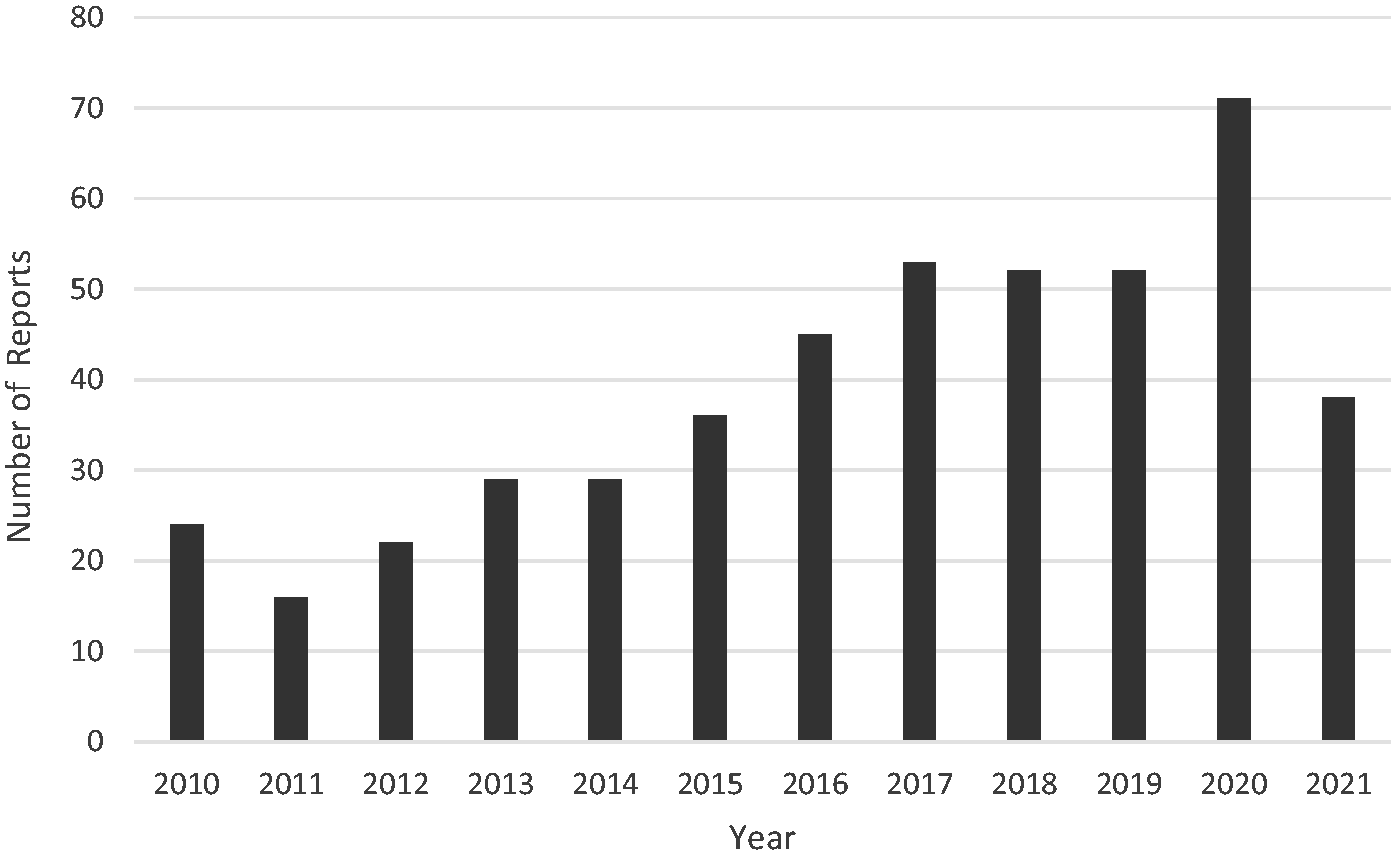
Number of reports, 2010 to 2021.
Of the 469 incidents, 302 (64%) were emergency cases and 291 (62%) were undertaken between 08:00 and 18:00 hours. Three hundred and forty-eight (74%) were undertaken using neuraxial anaesthesia and 178 (38%) under general anaesthesia. Four hundred and eighteen patients (89%) were aged between 17 and 39 years of age and 139 (30%) had a body mass index (BMI) greater than 30 kg/m2 (72 missing). There was one maternal death, in which the patient had a cardiac arrest on the ward and proceeded as a perimortem CS, with death of the neonate. There were eight incidents with neonatal deaths reported, affecting nine neonates. Of the reporting clinicians, 313 (67%) were specialists and 350 (75%) had been on duty for less than 10 hours.
The complete comparison of the 469 CS incidents with the remaining 8978 database reports is shown in Supplementary Tables 1–3. The age data were not compared, as we identified skewed data due to clinicians reporting the neonate’s age, rather than the maternal age. The 469 incidents included in our analysis were more likely to be emergency cases (RR 1.95), more likely to occur between 18:00 and 22:00 hours (RR 1.81) and between 22:00 and 07:59 hours (RR 4.40), and more likely to be undertaken using neuraxial anaesthesia (RR 9.18). There was no significant difference between the two groups in terms of BMI, while CS incidents were less likely to have an ASA score of 3 (RR 0.41) or 4 (RR 0.16) or a final outcome of death (RR 0.23) than other incidents. Compared with the other incidents, reporting clinicians were more likely to be trainee year 1–2 (RR 2.77) or trainee year 3–4 (RR 2.61) and were more likely to have worked continuously for 16–24 hours (RR 3.00).
Categorisation of incidents is shown in Table 1. Most incidents had more than one event. The most highly represented categories included intraoperative neuraxial anaesthesia complications (181, 39%) including problems with conversion to general anaesthesia in this setting, medication errors or issues (136, 29%), equipment issues (49, 10%), obstetric haemorrhage 38 (8%), endotracheal tube issues (28, 6%) and maternal arrests and peri-arrests (28, 6%). The remaining incidents were reported in 5% or less of the 469 reported incidents.
Categorisation of 469 anaesthesia incident reports during caesarean section, 2009–2022.
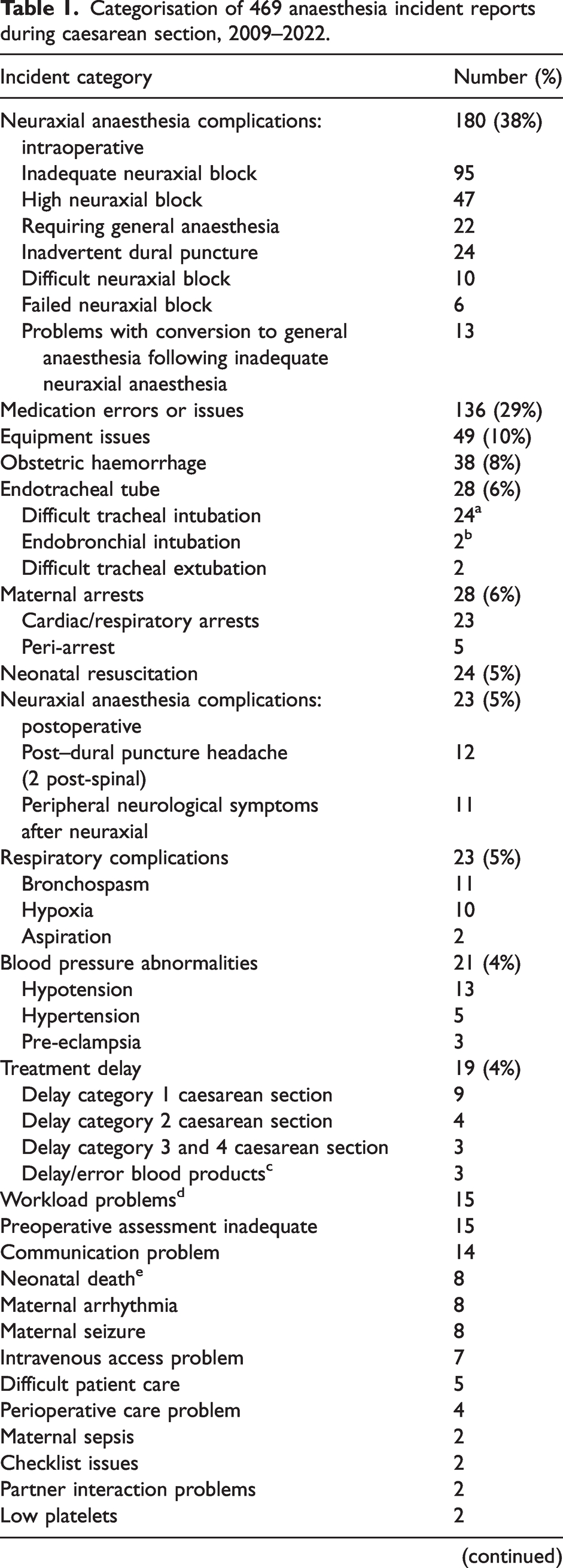
The main categories are reported as a percentage of 469, with more than one category being able to be allocated to each incident.
Nine of these are included in the ‘neuraxial anaesthesia complications: intraoperative’ category as ‘problems with conversion to general anaesthesia’.
One of these is included in the ‘neuraxial anaesthesia complications: intraoperative’ category as ‘problems with conversion to general anaesthesia’.
In one there was a delay receiving blood products, in one clinician unfamiliarity with local processes led to the delay, in one an incorrect unit was provided.
In these incidents the narrative described conflicting or additional clinical priorities that influenced the event reported; for example, two obstetric patients requiring urgent care or handover between clinicians.
Includes one set of twins (nine deaths).
Of the 95 patients with inadequate neuraxial anaesthesia, 65 (68%) required conversion to general anaesthesia. Of those 65, 13 (20%) had problems with conversion to general anaesthesia. Problems encountered included difficult intubation, bronchospasm, endobronchial intubation and difficult ventilation.
Of the 47 high neuraxial blocks, in 10 incidents the high block followed a single-shot spinal as the primary anaesthetic technique for CS, with two requiring conversion to general anaesthesia. In three, combined spinal/epidural (CSE) was the primary anaesthesia technique for CS and one of those required conversion to general anaesthesia. The remaining 34 incidents of high neuraxial block resulted from blocks that were initially inserted for labour analgesia (32 epidurals and two CSEs, 74%). In 10 of the 34 incidents the high block followed the use of spinal anaesthesia as a rescue following inadequate labour analgesia and/or unsuccessful epidural extension. In seven of the 34 incidents, the high block precipitated an urgent caesarean birth that was not otherwise indicated and five of those required general anaesthesia. Of all 34 high neuraxial blocks in which neuraxial labour analgesia was the primary technique, general anaesthesia was required in 19. In total, 22 (47%) of the patients with high neuraxial blocks required general anaesthesia. Nineteen of those 22 (86%) occurred in the context of insertion of an epidural for labour analgesia, or extension of an existing labour epidural for anaesthesia.
Subcategorisation of medication errors with examples is shown in Table 2. Allergic responses were the most commonly reported problem (30), followed by problems with oxytocin administration (17) and syringe swaps and/or wrong route administration. Four ‘near miss’ medication events were reported, in which ropivacaine was nearly administered intravenously, thiopentone was nearly administered to the epidural, a repeat dose of medication was intercepted prior to rectal administration, and pancuronium nearly prepared instead of suxamethonium. Of the 49 incidents involving equipment issues, 12 involved epidural or CSE kits or fixation devices and six involved difficulties with the anaesthesia machine, circuit or ventilator.
Medication problems reported more than once during caesarean section.
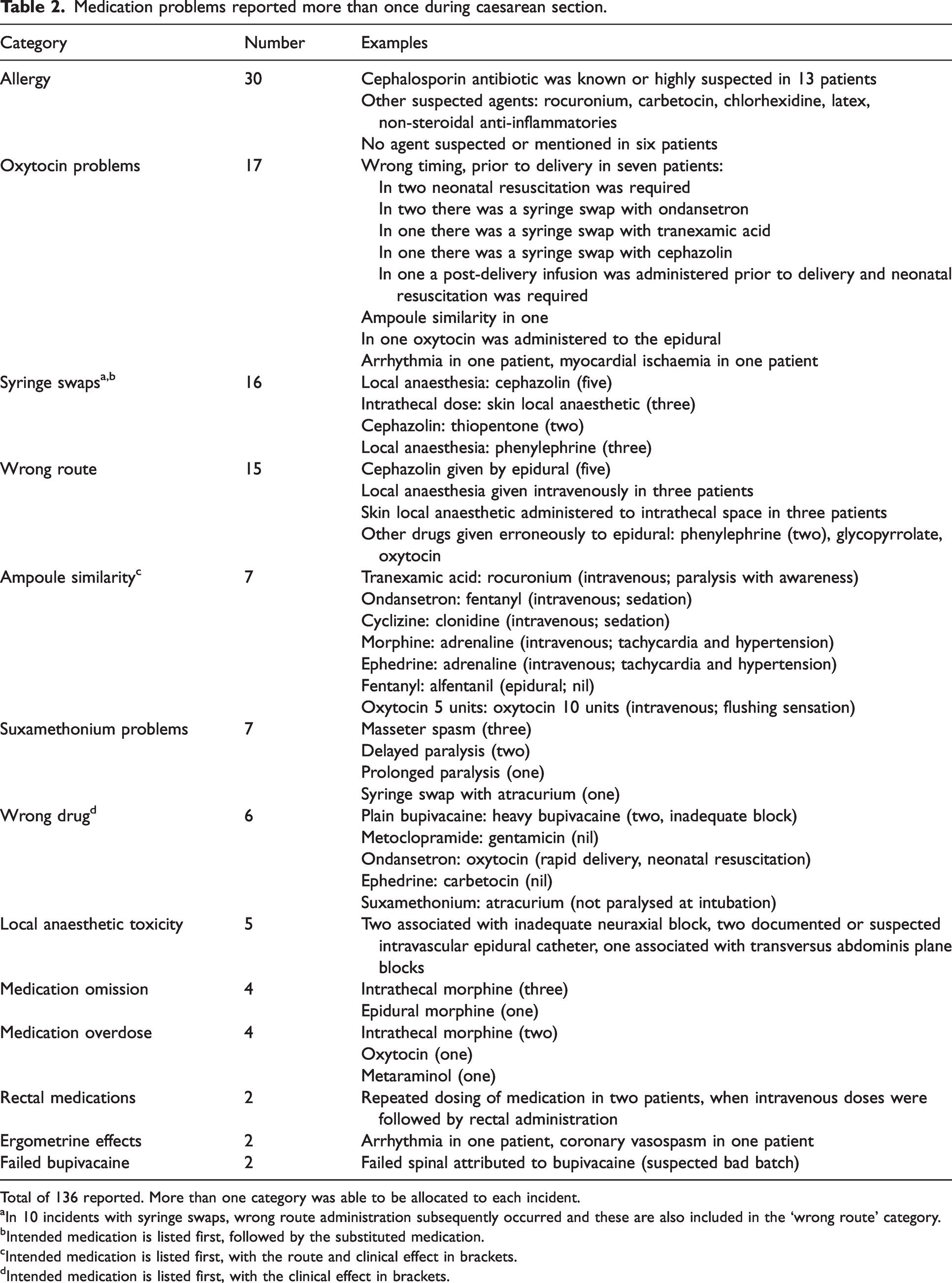
Total of 136 reported. More than one category was able to be allocated to each incident.
In 10 incidents with syringe swaps, wrong route administration subsequently occurred and these are also included in the ‘wrong route’ category.
Intended medication is listed first, followed by the substituted medication.
Intended medication is listed first, with the route and clinical effect in brackets.
Intended medication is listed first, with the clinical effect in brackets.
Thirty-eight reports included significant maternal haemorrhage, with eight incidents including maternal cardiac arrest and three involving blood bank delay (2) or error (1). There were 23 incidents with maternal cardiac or respiratory arrests and 24 neonates that required resuscitation (Table 3). In three incidents requiring neonatal resuscitation the reporting anaesthetist provided initial resuscitation and in four they provided assistance.
Conditions suspected or known to be associated with 23 incidents with maternal cardiac and respiratory arrests. Resuscitation details for 24 cases in which neonatal resuscitation was required.
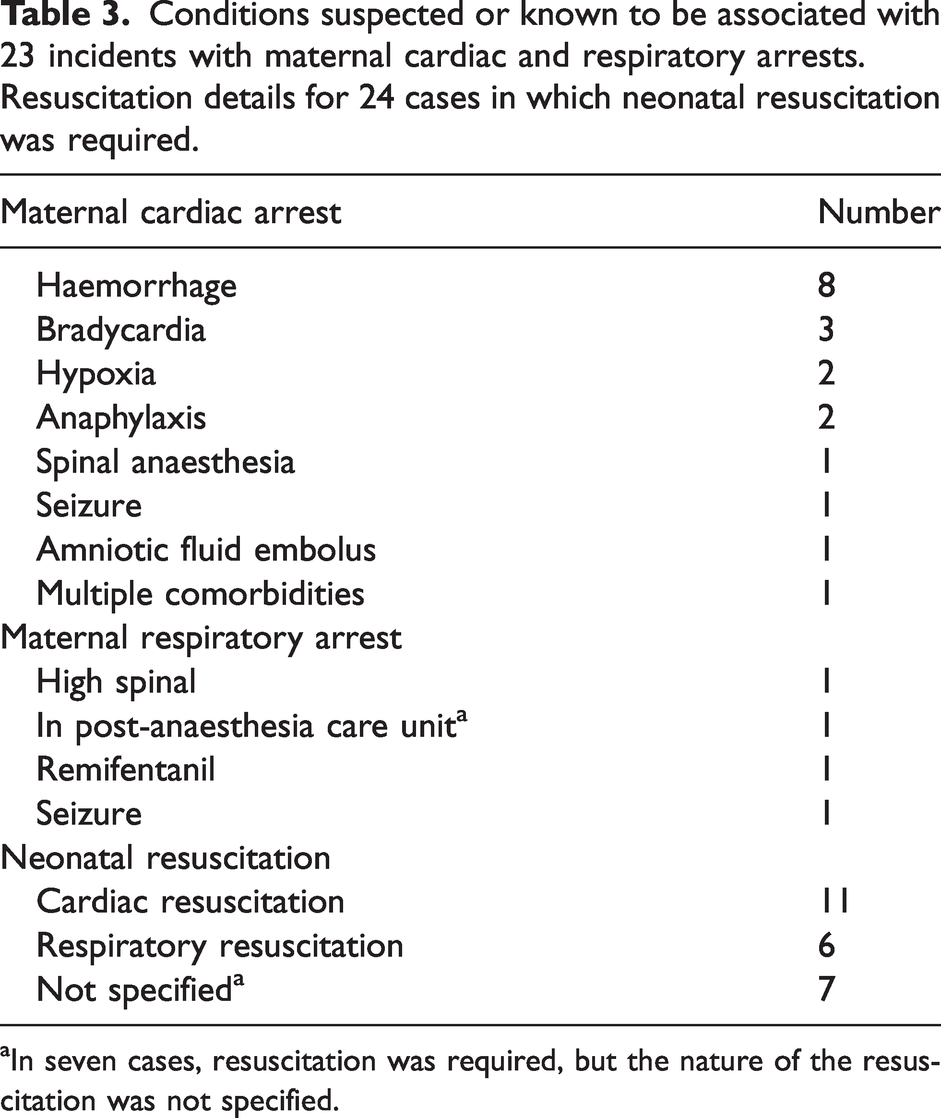
In seven cases, resuscitation was required, but the nature of the resuscitation was not specified.
Twenty-eight reports included problems with tracheal intubation or extubation. Of the 26 tracheal intubation problems, 24 were described as difficult, with one requiring a surgical airway. Two described endobronchial intubations, one associated with hypoxia. Of the 24 difficult tracheal intubations, nine were undertaken in the context of conversion to general anaesthesia for inadequate or failed neuraxial anaesthesia. In five, there were additional factors present that may have contributed to operator performance (cardiac arrest, laryngoscope light failed, masseter spasm, regurgitation and maternal haemorrhage).
Discussion
The incidents reported reflect the nature of obstetric anaesthesia. Compared with non-caesarean incidents, these incidents tended to occur more often after hours, for emergent indications, and in patients of ASA PS 1 or 2. They were also more likely to be reported by anaesthesia trainees. The most frequently reported incidents reflect the high rate of neuraxial anaesthesia used, with the well recognised problems of inadequate block or high block commonly reported. Reporting of CS incidents increased over time. The reason for markedly reduced numbers in 2021 is not known. No systemic failures in the incident reporting system were identified during 2021; however, we speculate that clinician fatigue during the COVID-19 pandemic may be implicated. If so, this may impact other reports from webAIRS during this period.
In 1999, when Sinclair et al. reported on 203 obstetric incidents in the Australian Incident Monitoring Study, their group (obstetric analgesia and anaesthesia) comprised 4.1% of reports and 33.5% involved neuraxial anaesthesia/analgesia. 14 While our set of incident reports included only CS incidents, this is similar to our proportions. In Australia, New Zealand and many other countries, the use of neuraxial anaesthesia is considered the standard of care and is widely accepted by our patients. However, failure or inadequacy of neuraxial anaesthesia necessitates an ever-ready ‘Plan B’ of general anaesthesia. A substantial fraction of the reported incidents involved general anaesthesia, despite only 5% of CS Australia-wide being undertaken using general anaesthesia. 2
Difficult tracheal intubation rates in obstetric anaesthesia are consistently reported to be higher than in the non-obstetric population. 15 Maternal, fetal, surgical and situational factors are likely to be contributory. 16 In this report, difficult tracheal intubation followed inadequate neuraxial anaesthesia in nine incidents and was accompanied by other significant clinical stressors in five others. Accurately assessing the adequacy of neuraxial anaesthesia requires knowledge, experience, excellent communication skills and a degree of humility. 17 Modelling of these attributes by consultant anaesthetists to anaesthesia trainees, combined with an environment that focuses on patient safety is essential. The ability safely to transition to general anaesthesia when required is an essential skill and one that may be enhanced with simulation-based teamwork training.
Clinician motor and cognitive skills are impacted by situational stress. 16 Added complexities in obstetric anaesthesia contribute to clinician stress, including the presence of an awake patient, their support person and a multidisciplinary team, who are all witnesses to the ‘failure’ of anaesthesia. Management of a high neuraxial block is another indication for urgent conversion to general anaesthesia. One-third of the high blocks reported here occurred when spinal anaesthesia was used as a secondary technique following inadequate epidural extension. Caution is recommended in this scenario and CSE may be a safe approach, administering a smaller spinal component and using the epidural to extend the block. Overall, nearly one in two people with high blocks required conversion to general anaesthesia. Prevention of conversion to general anaesthesia by avoiding high blocks is essential, particularly in the setting of a patient with a functioning or partially functioning epidural. When conversion to general anaesthesia is required, calm communication with the patient and support person is necessary, as well as knowledge, skill and confidence based on past experience and training. Insights from sports psychology may be useful in preparing for general anaesthesia in this situation, utilising metacognitive skills and performance enhancing routines. 18 While no difficult tracheal intubation events co-existed with an anaesthesia machine, circuit or ventilator problem, it is essential to ensure that the anaesthesia machine has been checked prior to all CS cases, even those commenced under regional anaesthesia.
Other contributors to clinician stress may include lack of on-site supervisory support after hours or long continuous hours of work. CS incidents were more likely to happen after hours and a substantial fraction of the reporting clinicians had worked for more than 10 continuous hours. ANZCA recognises the implications of fatigue for clinician performance and health, providing guidance to individuals and facilities to reduce the impact of fatigue on safe patient care and occupational health and safety, stating that ‘Anaesthetists should not work in excess of 16 hours in a 24-hour period.’ 19
Medications were implicated in many reports, due to clinician error or known physiological effects. Allergic reactions comprised the highest subcategory of medication problems, with a cephalosporin antibiotic being the suspected or confirmed agent in a third of incidents. Of note, there were no reports of allergic reactions in the analysis of AIMS data by Sinclair et al. 14 It is difficult to draw conclusions from this; however, the rates of allergic diseases in children and young adults are increasing in Australia 20 and across the world. 21 The current practice of prophylactic antibiotics being administered to all patients undergoing CS has evolved over the previous 10 years. Antibiotics are frequently cited as the most common cause of overall perioperative anaphylaxis, with the actual causative agent determined by local practice patterns. 22 , 23
Rectal administration of co-analgesics was previously common and we report incidents of repeat dosing and one near miss involving this practice. Oral and intravenous formulations are effective, readily available and the benefits of rectal administration are unlikely to outweigh the risks of this medication error. Another practice in decline is the use of thiopentone for induction of general anaesthesia for CS. Propofol is appropriate for use 24 and the colour provides an obvious visual signal that may prevent syringe swaps, such as those involving cephalosporin antibiotics and thiopentone. ‘Wrong route’ medication errors reported here included local anaesthetic administered by the intravenous route and several medications administered by the epidural route. The international standard covering neural connectors has currently been adopted by a small number of Australian and New Zealand institutions. 25 Despite the significant implementation challenges, more widespread adoption of this standard should reduce these wrong route errors. In the meantime, in addition to labelling and the use of other visual cues, a colleague or assistant should check all medication to be administered into the neuraxial space at the time of administration. Deaths and permanent paralysis can result from such errors. The accidental intrathecal administration of tranexamic acid, which is now commonly used in obstetric anaesthesia, has a mortality rate of 50%. 26
The report by Sinclair et al. included two cases in which oxytocin was given in error; in one the fetus required resuscitation and the outcome of the other case is unknown. 14 Similarly, we report seven incidents in which oxytocin was mistakenly administered prior to birth, with adverse neonatal effects noted in two, requiring rapid delivery and neonatal resuscitation. One of these involved the erroneous rapid administration of a one litre bag of fluid containing 40 units of oxytocin, intended for post-birth use. Others involved syringe swaps. Recognising the high cognitive load of performing anaesthesia for CS, these events will encourage anaesthetists to implement strategies to avoid inadvertent pre-birth administration of oxytocic medications.
With 19 maternal cardiac arrests reported, it is important for all clinicians to be aware of the special requirements for maternal cardiopulmonary resuscitation and peri-mortem CS. 27 The combination of obstetric haemorrhage and cardiac arrest was reported in eight incidents, a reminder of the rapidity with which blood loss occurs from the gravid uterus. Ready access to blood products, a massive transfusion protocol and mechanisms to increase staffing capacity acutely are important institutional processes in managing patients with rapid haemorrhage. Rapid volume resuscitation may be necessary prior to general or neuraxial anaesthesia in the presence of bleeding. Anaesthesia staff continue to provide neonatal resuscitation when required, a skill that is included in the ANZCA curriculum and intermittently adds to the cognitive load of this particular anaesthesia subspecialty.
As a voluntary reporting system, we cannot draw conclusions about the frequency with which these events occurred. As with all voluntary reporting systems, the accuracy of these data is dependent on the accuracy of those entering the incident information. We have not reported the gestation or parity of the patients, as the database does not provide for the routine reporting of these details. The ability to categorise the events was limited by the amount of detail provided in the narrative entry by the clinician, preventing the use of standardised definitions for conditions such as neonatal resuscitation, hypotension or haemorrhage. The analysis of CS incidents identified a unique limitation relating to data entry, in which clinicians entered the age and outcome of the neonate rather than the mother, when there was a clinical incident relating to the care or outcome of the neonate. This precluded accurate reporting of the maternal age. Clinical descriptions provided with the ASA scoring system have changed over time, and together with the subjective nature of the score this may have affected our results.
In summary, incidents reported to webAIRS regarding CS reflect modern obstetric anaesthesia practice, with complications of neuraxial anaesthesia being most commonly reported. During CS, our attention is divided between the patient, support persons and other clinicians. Strategies to avoid pre-birth administration of oxytocin are recommended, as is the adoption of the new standard for neural connectors. More data are needed to determine whether there is a problem with education and training in neuraxial analgesia and anaesthesia in pregnant people in order to prevent high neuraxial blocks. Transition from neuraxial anaesthesia to general anaesthesia is a high-risk time for complications. This transition may be practised, applying metacognitive skills in simulation-based teamwork training. The reporting and analysis of CS incidents to the webAIRS database will improve our understanding of how to prevent them from recurring.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X231196915 - Supplemental material for Analysis of anaesthesia incidents during caesarean section reported to webAIRS between 2009 and 2022
Supplemental material, sj-pdf-1-aic-10.1177_0310057X231196915 for Analysis of anaesthesia incidents during caesarean section reported to webAIRS between 2009 and 2022 by Victoria A Eley in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X231196915 - Supplemental material for Analysis of anaesthesia incidents during caesarean section reported to webAIRS between 2009 and 2022
Supplemental material, sj-pdf-2-aic-10.1177_0310057X231196915 for Analysis of anaesthesia incidents during caesarean section reported to webAIRS between 2009 and 2022 by Victoria A Eley in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-3-aic-10.1177_0310057X231196915 - Supplemental material for Analysis of anaesthesia incidents during caesarean section reported to webAIRS between 2009 and 2022
Supplemental material, sj-pdf-3-aic-10.1177_0310057X231196915 for Analysis of anaesthesia incidents during caesarean section reported to webAIRS between 2009 and 2022 by Victoria A Eley in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The authors would like to thank Heather Reynolds, ANZTADC data analyst, for assistance with data management and data cleansing and Ms Susan Considine, ANZTADC administration officer, for data cleansing.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest: Martin Culwick is the medical director of the Australian and New Zealand Tripartite Anaesthetic Data Committee. The other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.