
Abstract
In 2023, a Diploma of Rural Generalist Anaesthesia (DipRGA) was implemented across Australia. Developed collaboratively by the Australian and New Zealand College of Anaesthetists (ANZCA), the Australian College of Rural and Remote Medicine (ACRRM) and the Royal Australian College of General Practitioners (RACGP), the 12-month qualification is completed during or following ACRRM or RACGP Rural Generalist Fellowship training. Focused on the needs of rural and remote communities for elective and emergency surgery, maternity care, resuscitative care for medical illness or injury, and stabilisation for retrieval, the DipRGA supports rural generalist anaesthetists working within collaborative teams in geographically isolated settings. The goal is a graduate who can anaesthetise American Society of Anesthesiologists physical status class 1, 2 and stable 3 patients for elective surgery, provide obstetric anaesthesia and analgesia, anaesthetise paediatric patients and undertake advanced crisis care within their scope of practice. Crucially, they also recognise both limitations of their skills and local resources available when considering whether to provide care, defer, refer or transfer patients. DipRGA curriculum design commenced by adapting the ANZCA specialist training curriculum with consideration of the training approach of both the ACRRM and the RACGP, particularly the rural and remote context. Curriculum content is addressed in seven entrustable professional activities supported by workplace-based assessments and multisource feedback. Trainees are supervised by rural generalist anaesthetists and specialist anaesthetists, and complete flexible learning activities to accommodate geographical dispersion. Standardised summative assessments include an early test of knowledge and an examination, adapted from the ACRRM structured assessment using multiple patient scenarios.
Keywords
Introduction
Just over one in four Australians (28%) live in rural and remote areas. 1 These seven million Australians, which include Aboriginal and Torres Strait Islander peoples, have a greater burden of disease and injury, reduced access to healthcare, higher age-standardised mortality ratios and increased likelihood of dying from potentially preventable causes than do those in metropolitan areas. 2 Rural and remote communities require health practitioners and models of care that address their context, including generalists with extended scopes of practice and special skills, working collaboratively in teams to provide elective and emergency services. 3
Rural generalists are medical practitioners ‘trained to meet the specific current and future health needs of Australian rural and remote communities, in a sustainable and cost-effective way, by providing comprehensive general practice and emergency care, and required components of other medical specialist care in hospital and community settings as part of a rural healthcare team.’ 4 Importantly, in rural areas there is a ‘fragility’ of services, with heightened interdependence between those in the rural healthcare team. The loss of one local practitioner potentially causes a ‘domino effect’ leading to loss of others, leaving communities with a depleted service quite quickly. 5 Rural and remote communities rely on rural generalist anaesthetists (RGAs) for access to services including elective surgery, maternity care, emergency management of injury and severe acute illness and retrieval.6 –10
Despite their crucial role, the absence of formal recognition within the health system means there are few data available that characterise RGAs and the work they undertake. The best available dataset estimates 680 RGAs actively practice in Australia (Dr Greg Coates, personal communciation). Ninety per cent work in Modified Monash Model 3 to 7 regions, ranging from large rural towns like Albany, Western Australia, to very remote communities such as Thursday Island, Queensland. 11
In 2023, a new diploma of rural generalist anaesthesia (DipRGA) was implemented in Australia. This qualification was developed collaboratively by the Australian College of Rural and Remote Medicine (ACRRM), the Royal Australian College of General Practitioners (RACGP) and the Australian and New Zealand College of Anaesthetists (ANZCA). The diploma is completed within primary fellowship training with ACRRM or the RACGP, as an advanced skills component of which anaesthesia is one option.
This paper overviews the new diploma programme, including drivers for its design. The Defined Criteria To Report INnovations in Education (DoCTRINE) guidelines for reporting educational innovations in curriculum development were used to identify criteria to include. 12
Need for the new curriculum
From 1994, training for what is now termed rural generalist anaesthesia (previously general practice anaesthesia), was delivered by the Joint Consultative Committee of Anaesthesia (JCCA), a collaborative initiative of the three colleges. In the past, the term general practice anaesthetist (GPA) was commonly used but over the past decade this has changed in most contexts to rural generalist anaesthetist (RGA); the latter is used throughout this document, except when referring to historical circumstances. Twelve months of full-time equivalent training occurred in ANZCA or JCCA-accredited anaesthesia departments and supervision was provided by both specialist anaesthetists and RGAs. There was a dedicated curriculum and an exit examination. 13
Since its inception, there were calls from various quarters to enhance JCCA training. This included from the Australian Society of Anaesthetists General Practitioner Anaesthetists Committee (GPAC), and from GPA supervisors, other members and trainees of all three colleges. A key concern was the limited assurance of national minimum standards for training delivery. While there was a well-established training and assessment programme, the JCCA did not confer its graduates with a qualification, curriculum implementation varied across training sites, the examination was locally run and not nationally standardised, and there was limited monitoring and evaluation of training outcomes. Obstetric epidural skills and paediatric caseload were recommended but not mandated.
In addition, although the JCCA curriculum was regularly updated, educational practice and standards for postgraduate medical education have changed significantly since the training was first introduced. 14 Key developments in the postgraduate medical education sector include broader focus across all the roles of a specialist, not just medical expertise, 15 and use of workplace-based assessment to promote regular feedback on clinical performance for learning and as part of a portfolio of assessments of learning. 16
Curriculum
Redesign governance
From 2018 to 2021, curriculum development was undertaken by a Curriculum Development Working Group (CDWG), chaired by an independent medical education consultant (JA), with representation from RGAs, specialist anaesthetists, assessment experts, and college education and training staff. The group reviewed relevant literature and published curricula to ensure an evidence-based approach was applied. Informal consultation pathways through social media, JCCA logbook data and site data on procedural numbers also informed the work.
In 2021, the three colleges signed a memorandum of understanding for the DipRGA and finalised terms of reference for the Tripartite Committee of Rural Generalist Anaesthesia (TCRGA). TCRGA membership includes fellows of all three colleges, a rural consumer representative and a recent DipRGA graduate (until sufficient time has passed for this position to be filled by a recent DipRGA graduate, it is currently a doctor who has recently completed JCCA training). In early 2022, the TCRGA endorsed the finalised DipRGA curriculum document. 17
Purpose
The diploma is designed as an optional advanced skills training (AST) component of a primary rural generalist fellowship either through the ACRRM or the RACGP. The overall aim is to produce DipRGA graduates who can deliver safe anaesthesia and perioperative care in rural and remote settings for patients who are American Society of Anesthesiologists (ASA) physical status classification 1, 2 and stable 3 undergoing elective surgery, including for paediatric and obstetric patients within scope of practice. In addition, graduates may be required to work at the limit of their scope to provide necessary care in emergency situations. Most importantly, graduates need to recognise the extent of their expertise, balance all the risks of the clinical setting and other contextual factors and determine whether the patient should be transferred or referred to a larger centre. 18 The DipRGA curriculum also provides the basis for lifelong learning through continuing professional development.
The CDWG used the ANZCA anaesthesia training programme curriculum learning outcomes as the basis for the DipRGA curriculum, with reference to the current JCCA curriculum and relevant learning objectives from the ACRRM and the RACGP curricula.13,19,20 The overall DipRGA structure includes the roles in practice (CanMEDS roles adapted with permission), 15 clinical fundamentals (e.g. airway management, general anaesthesia, regional anaesthesia) and selected specialised study units (paediatric anaesthesia and obstetric anaesthesia and analgesia). 21
The group considered the need for vertical integration of curricula, the time constraints of a 12-month programme, and the strengths and practice philosophy which general practitioner and rural generalist trainees bring from their respective primary fellowships. Consequently, the DipRGA roles in practice emphasise the application of all the CanMEDS roles to perioperative medicine in rural and remote contexts. For medical expertise, competencies were selected pragmatically and amended to focus on the required breadth and depth of practice for a RGA, clinical application and the need for knowledge and skills to manage anaesthetic emergencies in resource-limited and geographically isolated rural locations.
The DipRGA curriculum is primarily designed to be delivered in accredited anaesthetic departments in metropolitan tertiary and medium-sized regional hospitals. This ensures appropriate caseload and case-mix during training and reflects JCCA accredited training sites. Provision is made for each trainee to spend up to 4 weeks of their training time in a rural location under the supervision of experienced RGAs. Daily supervision, mentoring and bedside teaching are provided by anaesthetic department supervisors of training (SOTs). The ANZCA training programme supervision framework is used (four levels of supervision from level 1 ‘the trainee needs the supervisor to be able to intervene immediately’ to level 4 ‘the trainee can manage the case with the supervisor off-site’). 21 SOTs within each Australian training region (state or territory) are supported by a state support officer who coordinates training and education within that region, and liaises with the central administration of ANZCA. Trainees are also encouraged to have a RGA mentor to support them as they prepare for rural practice.
Teaching and learning
This geographically distributed cohort needs flexible delivery options for teaching and learning activities. An accredited advanced life support course must be completed in the year prior to the diploma and courses on ‘can’t intubate, can’t oxygenate’, cardiac arrest, paediatric life support and neonatal resuscitation are mandated training requirements. For each of the courses, standards stipulate the learning required, regardless of how the trainee engages in the experience. Trainees can elect to complete an external course, a workshop which may be delivered at a conference or nearby hospital, an internal teaching session run by another department or even a one-on-one session with their SOT. Online modules to acquire knowledge are also highly recommended, including the management of anaphylaxis and major haemorrhage. JCCA teaching initiatives continue to be encouraged, including weekly tutorials, online case discussions with consultants sharing strategies for managing patients in the context of rural and remote resource limitations.
Within their electronic training portfolio's, DipRGA trainees must keep a logbook to demonstrate exposure to the breadth of cases and procedures required for progressively independent practice. A specific caseload is required for both paediatric anaesthesia and obstetric epidural analgesia. 17 The scope and volume of practice for paediatrics was guided by the Anaesthesia Practice in Children Observational Trial (APRICOT) study.22,23 After reviewing the literature on cumulative sum analysis in determining when anaesthesia trainees are expected to perform epidural analgesia independently24,25 and JCCA trainee logbook data, it was determined that 30 epidurals would be sufficient and feasible to ensure proficiency, if logged after the trainee has achieved competence. Competence is confirmed by successful completion of the EPA 3 (provision of obstetric epidural analgesia to patients with low-risk pregnancies).
Assessment
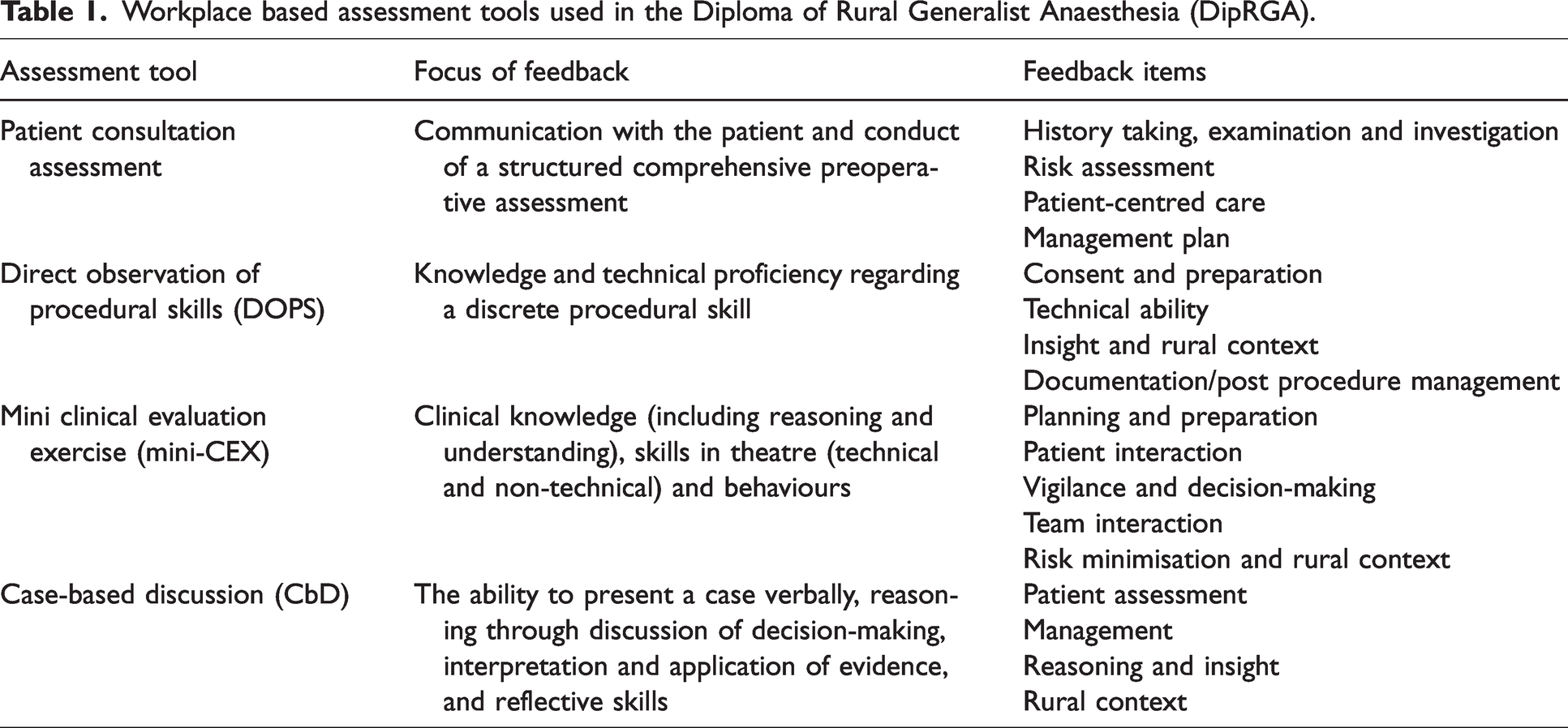
Consistent with current medical education best practice, a programmatic approach to assessment has been adopted, 26 which includes both assessment for learning and assessment of learning. To compensate for the shortcomings of any one assessment technique, 27 a combination of methods is used. Four bespoke workplace-based assessment tools drive learning (refer to Table 1). Each tool contains a criterion-referenced global scale based on level of supervision required for effective patient-centred care. 28 Items on the forms, mapped to learning outcomes, prompt assessors to comment on the trainee’s integration of CanMEDS roles and their ability to consider patient, facility and surgical factors that may influence planning or delivery in a rural and remote context. At the end of each form, the assessor is requested to document examples of what was done well and areas that need improvement. Trainees are encouraged to consider the feedback provided, reflect on their learning, and document an action plan. In the programme, multiple assessors, their expert judgement, and diverse perspectives are valued. 29 Multisource feedback is undertaken at least once, during the first 6 months of training, with input from at least seven team members, with results collated by the SOT and feedback provided to the trainee.
Workplace based assessment tools used in the Diploma of Rural Generalist Anaesthesia (DipRGA).
Entrustable professional activities (EPAs) represent discrete units of clinical work that require simultaneous integration of knowledge, skill and attitude competencies. 30 As the term implies, entrustment involves assigning responsibility to a trainee to undertake a relevant clinical activity (e.g. providing epidural analgesia for a patient in labour). 31 EPAs can be entrusted to a trainee for unsupervised execution when the required level of competence has been reached. 32 EPAs are now utilised for anaesthesia training as part of competency-based education frameworks in the United Kingdom and Canada.33,34 Increasingly, they are being implemented in postgraduate medical education and training in Australia and New Zealand also.35,36
Seven EPAs cover the breadth of the DipRGA curriculum and guide each trainee’s journey to becoming a diplomate. Each EPA has prescribed work-based assessments (WBAs) which must be used as evidence of successful completion. In some instances, other training requirements must also be achieved prior to entrustment (e.g., education on anaesthetic crises for EPA 3) and some EPAs are required before the trainee can move on to more advanced clinical activities (e.g. EPA 2 on providing obstetric epidural analgesia must be completed prior to commencing EPA 7 on providing obstetric anaesthesia and analgesia).
The diploma provides guidance as to when trainees are expected to achieve competence in the various EPAs (refer to Figure 1). If trainees are unable to achieve these timings, this may signal the need for additional support. Ongoing assessment and comprehensive periodic review at 3-monthly meetings between each trainee and their SOT ensure continued progress and an opportunity to discuss barriers which may impede trainee achievement. 37
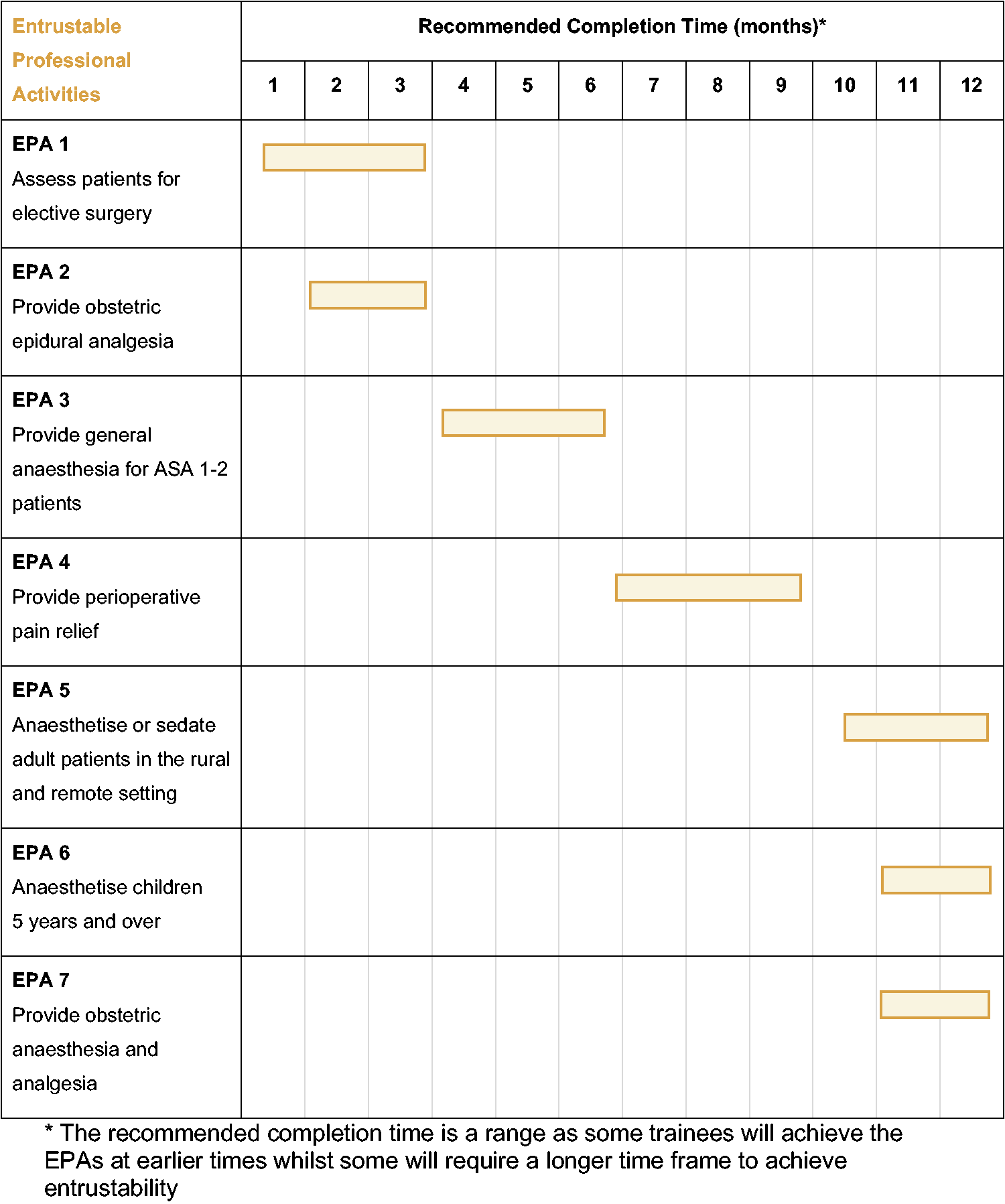
Entrustable activities (EPAs) to be completed and recommended timing during the Diploma of Rural Generalist Anaesthesia. *The recommended completion time is a range as some trainees will achieve the EPAs at earlier times while some will require a longer time frame to achieve entrustability.
Standardised summative assessment is included early in and towards the end of the diploma training. To drive learning in foundation concepts and safety, trainees have up to three attempts to pass a multiple choice (MCQ) examination in the first few months of training. This MCQ exam is benchmarked to the standard required of the ANZCA initial assessment of anaesthetic competence. 21 After approximately 10 months of training, DipRGA trainees will be assessed by a nationally delivered standardised structured scenario-based assessment (DRGASSSA), adapted from the ACRRM specialist training programme structured assessment using multiple patient scenarios (StAMPS) assessment. 38 The DRGASSSA assesses clinical reasoning in a highly contextualised (rural facility) framework. Prior to presenting to the DRGASSSA, trainees must have completed a minimum of 26 weeks full-time equivalent of clinical anaesthesia time and EPAs 1 to 4, as well as having made progress with the three remaining EPAs. Development work for both the MCQ and DRGASSSA examinations, including standard setting processes, is ongoing.
Implementation resources
Implementation of the DipRGA curriculum is supported by a training handbook 39 and training regulation. 40 Teaching and learning resources, including examination preparation resources, are adapted from existing training resources developed by the three colleges. An electronic training portfolio system, accessible to trainees, their SOTs and assessors, facilitates case logging, workplace-based assessments, formal training reviews, and tracking of trainee progress, locally by the trainee and their supervisor and also centrally.
There is a supervisor guide for identifying and supporting trainees who are not meeting training milestones or who experience other personal or professional difficulties that impact on their training. 41 This includes triggers that raise concerns, based on the Milton Keynes traffic light system, 42 risk assessment for immediate danger to the trainee or patient safety, and resources to support both the trainee and their supervisor, monitor progress and resolve the issue. While the administration of the DipRGA is through the ANZCA training and assessment unit, there is an integrated pathway for college support ensuring that the primary college (the ACRRM or the RACGP) is notified and involved according to defined thresholds of concern.
Accreditation for training
It is estimated that the programme will continue to train approximately 50 graduates each year. Anaesthesia departments accredited by the JCCA at the start of 2023 remain accredited for the new DipRGA training. The accreditation process beyond 2024 is in development. 39 It is possible that more departments will be accredited in the future, expanding capacity to train RGAs.
Evaluation plans
In line with best practice, implementation of the new curriculum will be monitored and evaluated. The electronic training portfolio system will support monitoring both process and outcome measures to ensure all trainees can access required experiences, to evolve the programme continually and to ensure comparability of implementation across training sites. Wider consultation will be required to ensure that other stakeholder perspectives on the programme are considered and to evaluate whether the diploma is producing sufficient graduates who meet community needs.
Discussion
We describe the development of a 12-month RGA training programme embedded within primary fellowship training for rural practice. It introduces a more programmatic and standardised assessment approach, involving workplace-based assessments and entrustable professional activities, with clear progress expectations across the training year and specific triggers for instituting additional trainee support. Greater consistency of curriculum implementation across training sites is facilitated by supervisor and examiner training, the introduction of state support officers, and enhanced central college oversight and support.
The design process identified and adapted quality education and training practices from within each college’s existing programmes. It also considered criteria for good assessment, 43 and published work on competency-based medical education and workplace-based assessment in anaesthesia training.44,45 Learning outcomes from the existing ANZCA specialist anaesthesia training programme were refined with the crucial lens of rurality, informed by ACRRM and RACGP training approaches, to ensure graduates consider patient factors, site-specific resources and geography in their decision making.
The workplace assessment tools are modified from those used in the ANZCA training programme and are thus familiar to specialist anaesthetist supervisors of DipRGA trainees. 16 These WBA tools have been adapted to include assessment domains specific to rural practice, with triggers to remind supervisors to consider relevant contextual issues in the assessment of trainee decision making and performance. The national viva-style assessment is modified from the ACRRM structured assessment using multiple patient scenarios (StAMPS). 38 The new electronic portfolio system streamlines trainee, supervisor and college understanding of progress through training and identification of those needing greater support. In future, it will facilitate data-driven training site accreditation and central monitoring of training processes and outcomes. 46
At the heart of this redesigned programme is improved support for high quality health services that serve the needs of rural and remote communities and improve health outcomes. Mandating obstetric epidural skills acquisition and anaesthesia for children aged 5 years and above drives a reliable new level of service for rural communities. The colleges are in the early stages of developing an advanced certificate of paediatric anaesthesia, with a focus on additional training and assessment to achieve competence in providing care for children aged 3 and 4 years.
Australia has particular challenges in healthcare access for its geographically dispersed population, with many services concentrated in coastal and capital cities. 2 Other affluent countries like Canada and the United States have similar geographical challenges. 7 Since 1974, South Africa has had a diploma in anaesthetics (DA (SA)), run by the College of Anaesthetists of South Africa. 47 The curriculum includes knowledge and skills under 10 clinical domains acquired over 6 months of supervised training with two centralised examinations and no WBAs. 48 In Canada, family medicine practitioners complete a 12-month residency in family practice anaesthesia with a structured curriculum (priority topics and key features for assessment), with a certificate of added competence on completion. 49 This is similar to the pre-2023 JCCA certification in Australia. However, most of the 500 family physician anaesthetists practise in a limited number of provinces. 50 The integration of the DipRGA into primary fellowship training is a unique aspect of this new qualification.
The implementation of the new DipRGA curriculum is occurring in the context of other Australian health system developments and policy drivers that support improved healthcare access and equity for those living and working in rural and remote areas. The Australian National Medical Workforce Strategy 2021–2031 notes the declining number of non-general practitioner specialists with increasing rurality and lower numbers of general practitioners in small rural towns and remote communities. 51 This strategy recognises the need to optimise the medical workforce to serve these communities, through the pillars of rebalancing supply and distribution, training reform and increasing generalist capabilities. The DipRGA supports these pillars, reflecting the accountability of the three colleges to rural and remote communities.
Australia is at the forefront of developments internationally with the appointment of a National Rural Health Commissioner in 2017 and introduction of the National Rural Generalist Pathway in 2021. 52 The Australian Federal Government has committed funding for improved organisation of rural generalist training, including coordination units in each Australian state and territory, along with expanded prevocational and vocational posts in rural and regional areas, and support for the ACRRM and RACGP application to the Medical Board of Australia for recognition of rural generalism as a ‘distinct field of general practice’ under the Australian Health Practitioner Regulation National Law. 52
Bringing three organisations with their own perspectives and visions together, especially during a global pandemic, has had its challenges. Maintaining focus on the overarching purpose of serving rural and remote communities and their needs for high quality and accessible RGA care has facilitated collaborative work. The CDWG was fortunate in developing and consolidating relationships through face-to-face meetings prior to the onset of COVID-19. The bonds developed as a result of these early meetings facilitated collaborative work once meetings were confined to videoconferencing.
A limitation of the diploma development process was a lack of similar curricula internationally to draw on for comparison and benchmarking. Coupled with scarce data about current RGA practice across the country, and no formal ways systematically to communicate with these practitioners, the development group was reliant on its representative expertise and informal consultation mechanisms.
Optimally, educational developments are informed by rich datasets. This new curriculum was informed by the limited data available through JCCA trainee logbooks and information on procedures from training sites. Ongoing curriculum evolution will be enhanced by the extensive data that will be collected as trainees complete the redesigned programme. This is facilitated by recording in the electronic training portfolio system.
In future, an earlier and broader consultation process would include input from consumers and communities, including those living in rural and remote areas and Aboriginal and Torres Strait Islander peoples to ensure we are addressing their needs. This would include relevant representatives on the curriculum revision group and iterative consultation about health needs. In addition, the already established tripartite governance structure will faciliate planning and effective management of future curriculum evaluation and review.
Conclusions
The new DipRGA replaces and enhances the prior JCCA training curriculum which has underpinned anaesthesia services to Australian rural and remote communities for nearly 30 years. It is being implemented in the context of significant health system changes aimed at strengthening health equity, access and outcomes for this large group of Australians. It was developed collaboratively with a focus on strengthened educational quality and integration with the outcomes and philosophies of primary fellowship training with the ACRRM and the RACGP.
Footnotes
Author Contribution(s)
Acknowledgements
The authors acknowledge the contributions of all those from the three colleges who were involved in DipRGA development, fellow and staff support from the ACRRM and the RACGP, and project and educational funding provided by ANZCA.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LR is an ANZCA staff member and JA was contracted by ANZCA to lead the curriculum design work. Each contributed to the development of this manuscript in her own time.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.