
Abstract
There is a paucity of literature describing the research productivity among trainees in intensive care medicine. We sought to examine the occurrence and determinants of successful publication outcomes associated with intensive care training. The study cohort consisted of all individuals admitted to fellowship of the College of Intensive Care Medicine of Australia and New Zealand (CICM) from 2012 to 2019. The primary outcome measure of this study was manuscripts indexed on PubMed within one year after and four years prior to admittance to CICM fellowship. Four hundred and eighty-five fellows were identified of whom 216 (45%) had at least one publication; 129 (27%) had one, 34 (7%) had two, 21 (4%) had three and 32 (7%) had four or more publications. Overall 138 (28%) fellows had at least one publication that was likely associated with their mandatory CICM training project for which they were first (n = 110; 80%) and/or corresponding (n = 72; 52%) author in the majority of cases. Overall 107 different senior/mentor authors were identified, with 13 individuals supporting more than one publication. Although gender and location at the time of fellowship award were not associated, location of receipt of medical degree, shorter time period between medical school graduation and fellowship award, more recent year of award, and completion of medical degree/fellowship in the same geographical region were associated with project publication. A minority of CICM fellows have PubMed-indexed publications related to their training. Further efforts are warranted to better define the determinants of successful project publication to optimise future opportunities.
Keywords
Introduction
Conduct of research is considered an integral component of clinical training and its performance may enhance critical appraisal skills, expand career opportunities and improve patient outcomes.1 –4 While acquisition of funding, development of protocols, and conduct of research are highly valuable scholarly activities, publication in an indexed peer-reviewed journal remains the most widely recognised outcome metric of research productivity.5,6 A recent structured review examining graduate medical trainee (i.e. training post medical school) research found that productivity was generally associated with individual characteristics of male gender, prior research experience, and pursuit of a higher research degree, as well as programmatic aspects not limited to mentorship and work environment. 7
An ability to understand and apply research is an important aspect of intensive care medicine, and many training programs, including the College of Intensive Care Medicine of Australia and New Zealand (CICM), mandate its successful performance as a requirement for certification. 8 Although there is an evolving body of literature predominantly from North America regarding research productivity among graduate medical trainees, there is a paucity of information surrounding the research productivity of individuals undertaking intensive care medicine training. 7 The objective of this study was therefore to examine the rate of, and factors associated with, publication success among CICM trainees.
Methods
Study subjects and design
We used a retrospective cohort design. The study cohort consisted of all individuals admitted to fellowship of CICM from 2012 to 2019. Although the pathway to CICM fellowship has a minimum of six years of training, it varies among individuals, with duration of training influenced by factors not limited to prior experience, concomitant training in other specialties, part-time scheduling, and variable duration in preparation for and success in examinations. Generally speaking, medical school graduates complete a year of internship followed by an approximate three-year period of residency training whereby trainees gain broad experience prior to pursuit of formal critical care training. Registrar trainees then rotate through different intensive care units (ICUs) over an approximate four-year period to gain clinical experience and undergo a minimum of one year of anaesthesia training. Trainees are required to successfully pass written and clinical examinations and complete and present the results of a novel research project prior to being eligible for CICM fellowship. 8 Publication is not a requirement. One year of transition experience has been required for those entering the training program as of 2014.
The primary outcome measure was published articles indexed within PubMed. Given that this study involved an analysis of publicly available information, ethics approval was neither sought nor required.
Study protocol
All individuals admitted to fellowship were identified through annual reports publicly available from CICM. 9 The year of admittance, name and location (state, territory and/or country) at fellowship award were abstracted for all subjects. Gender, and year and location of medical degree award was obtained from The Australian Health Practitioner Regulation Agency (Ahpra) Register of Practitioners and the New Zealand Medical Council Register of Doctors.10,11 Ad hoc internet searches were performed for those fellows not listed within these sites.
Publications authored by identified fellows were then searched for using the PubMed database. Searches were conducted independently by two reviewers. Reports were limited to a five-year period encompassing four years prior to, and one year post, award of fellowship. This period was defined a priori. The fellow’s first and last names were initially searched. If there were no retrievals then the author’s last name and first initial was searched. If no citations were identified, zero publications were recorded. In the event that one or more publications were identified, author lists and abstracts and selected full length reports were reviewed to assess whether the study subject and listed author represented the same individual. Where it was unclear or where there were multiple potential authors with the same name, articles were attributed to the author based on an individual assessment that included one or more of: the location of study, topic area related to critical illness, co-author’s affiliation with Australasian ICUs, and ad hoc internet searches.
Among the overall reference list compiled, we further aimed to identify articles compatible with a candidate’s published CICM project. 8 Presumptive project publications were those where the author had a prominent role in the primary authorship (i.e. first, second, third or corresponding author) and/or where contributor declaration statements indicated a significant role. Narrative reviews, editorials, correspondence and abstracts were excluded based on CICM project requirements. 8 In addition, publications were also excluded where fellows were listed within a large corporate group of authorship. In the event that subjects had more than one potential publication related to a CICM project, the most relevant was chosen with first author reports prioritised where all else was equal.
Full-text articles were then obtained for all presumptive CICM project publications and data were abstracted for the following variables: year of publication, position of authorship, number of authors, corresponding author (i.e. author contact information listed for publication-related queries), journal name, location of primary study (city, state), mentor/senior author name, and study type. Mentor/senior authors were defined as those individuals who were the corresponding author (if not the trainee) and/or in the last author position in the author order. Study types were classified as described previously. 7
Statistical analysis
Statistical analysis was performed using Stata 17.0 (College Station, TX, USA) and was primarily descriptive. Prior to analysis, continuous variables were assessed for their underlying distribution using histograms. Medians with interquartile ranges (IQRs) were used to describe skewed continuous variables. Grouped medians were compared using the Wilcoxon–Mann–Whitney test and Cuzick’s test was used when these groups were ordered. Categorical data were reported as proportions (%) and groups were compared using Fisher’s exact test. Where missing values were present these were not replaced, and analysis was reported with reduced number (n). Unadjusted P-values less than 0.05 were deemed to represent statistical significance.
Results
Demographics
A total of 485 fellows were identified during the study period of which 346 (72%) were male, 134 (28%) female and two (<1%) were not classified. One-half (n = 242; 50%) were international medical graduates (i.e. other than Australia and New Zealand). The median time between medical school graduation and admittance to fellowship of CICM was 12 (IQR 10–15; n = 462) years. The location registered at receipt of fellowship award was New South Wales (n = 123, 25%), Victoria (n = 112, 23%), Queensland (n = 92, 19%), Western Australia (n = 45, 9%), other Australia (n = 41, 8%), New Zealand (n = 42, 9%) and international (n = 17, 4%).
Number and type of publications
A total of 544 publications were identified among the study cohort. Two hundred and sixteen (45%) fellows had at least one publication, of whom 129 had one (27%), 34 (7%) had two, 21 (4%) had three and 32 (7%) had four or more publications. There were 138 (28%) fellows who had at least one publication compatible with a CICM training project. There were 78 fellows who had had at least one publication, but none were determined to be likely CICM projects according to our pre-established criteria. Of these publications, 24 (31%) were case reports, 14 (18%) were narrative reviews, seven (9%) were correspondence or letters to the editor, one was COVID19-related (onset after fellowship completion) and in 19 (24%) and 13 (17%) of cases the fellow was ranked either low in primary or listed solely within a large corporate authorship, respectively.
Authorship
Among the 138 presumptive CICM project publications, the median number of authors was five (IQR 3–7), with the fellow as the first author in most (n = 110, 80%) cases. The fellow was second or third author in 21 (15%) and five (4%) of cases, respectively, with the remaining two being senior authors (i.e. last and corresponding). Overall, among the 138 presumptive project publications the fellow was corresponding author in 72 (52%) cases.
Study design
Most of the 138 presumptive CICM projects were classified as cohort studies (n = 80, 58%), with 17 (12%) as case series, 14 (10%) systematic reviews, nine (7%) diagnostic investigations, seven (5%) cross-sectional, six (4%) basic science/translational, two (1%) clinical trials and three (2%) other. Although the median study sample size was 123 (IQR 49–583; n = 125), this ranged widely from a case series of three patients to a large registry-based study including 710,535 subjects.
Study location and mentoring
The primary location of the 138 presumptive CICM projects was VIC (n = 34, 25%), QLD (n = 27, 20%), NSW (n = 25, 18%), WA (n = 1, 9%), South Australia (n = 6, 4%), other Australia (n = 10, 7%; including three each in Northern Territory, Australian Capital Territory, and Tasmania), New Zealand (n = 9, 7%) and international (n = 14, 10%). Overall 107 different mentor/senior authors were identified with three, six and four individuals listed in four, three and two publications each, respectively.
Publication journals
Reports of presumptive CICM projects were published in 78 different journals with the most common being Critical Care and Resuscitation (n = 22, 16%), Resuscitation (n = 7, 5%), Critical Care Medicine (n = 5, 4%), Journal of Critical Care (n = 5, 4%), Anaesthesia and Intensive Care (n = 4, 3%), Emergency Medicine Australasia (n = 4, 3%), Intensive Care Medicine (n = 4, 3%) and Journal of Paediatrics and Child Health (n = 4, 3%).
Determinants of publication
Among the cohort of 485 fellows, no significant differences in publication rates were observed between males and females or where the fellow was located at the time of CICM award, as shown in Table 1. However, there were significant differences according to medical school graduation location, with the lowest rates observed among those with international and New Zealand degrees (Table 1). Of the 242 international medical graduates, the most common medical degree locations were India (n = 84, 35%), the United Kingdom (n = 64, 26%), South Africa (n = 16, 7%), Ireland (n = 10, 4%) and Hong Kong (n = 8, 3%); publication rates were 23% (19/84), 16% (10/64), 31% (5/16), 40% (4/10) and 50% (4/8), respectively.
Factors associated with publishing a fellowship project associated with intensive care medicine training.
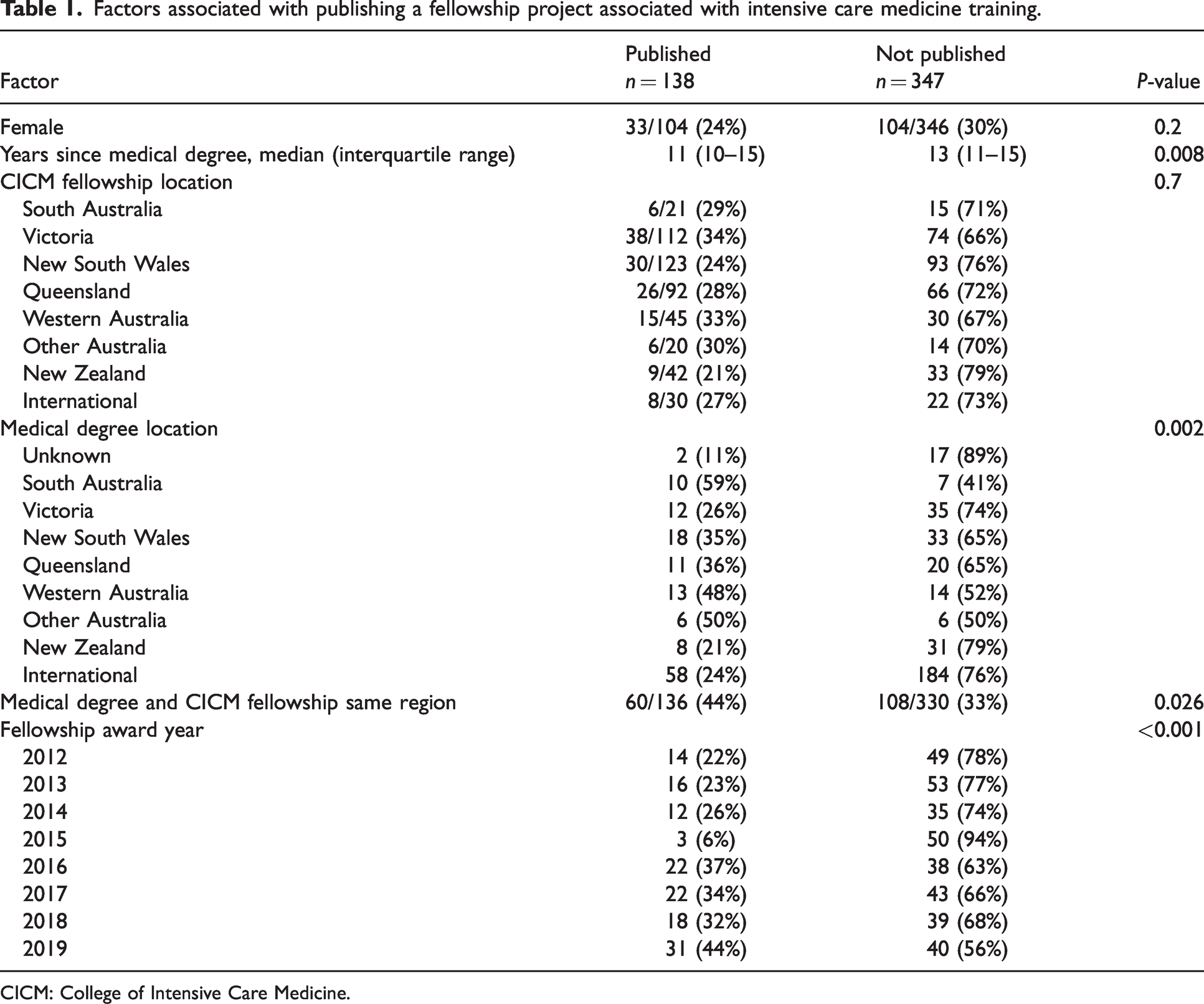
CICM: College of Intensive Care Medicine.
The median time from medical school graduation to fellowship award was less for those who had a published project, with one-half of those completing fellowship within eight years, as shown in Figure 1. Although the proportion of fellows publishing a CICM project varied significantly by year and increased over time, the annual number of publications among fellows who did and did not have at least one CICM publication were relatively constant with the exception of 2019 (skewed by four individuals with a combined 82 publications), as shown in Figure 2.
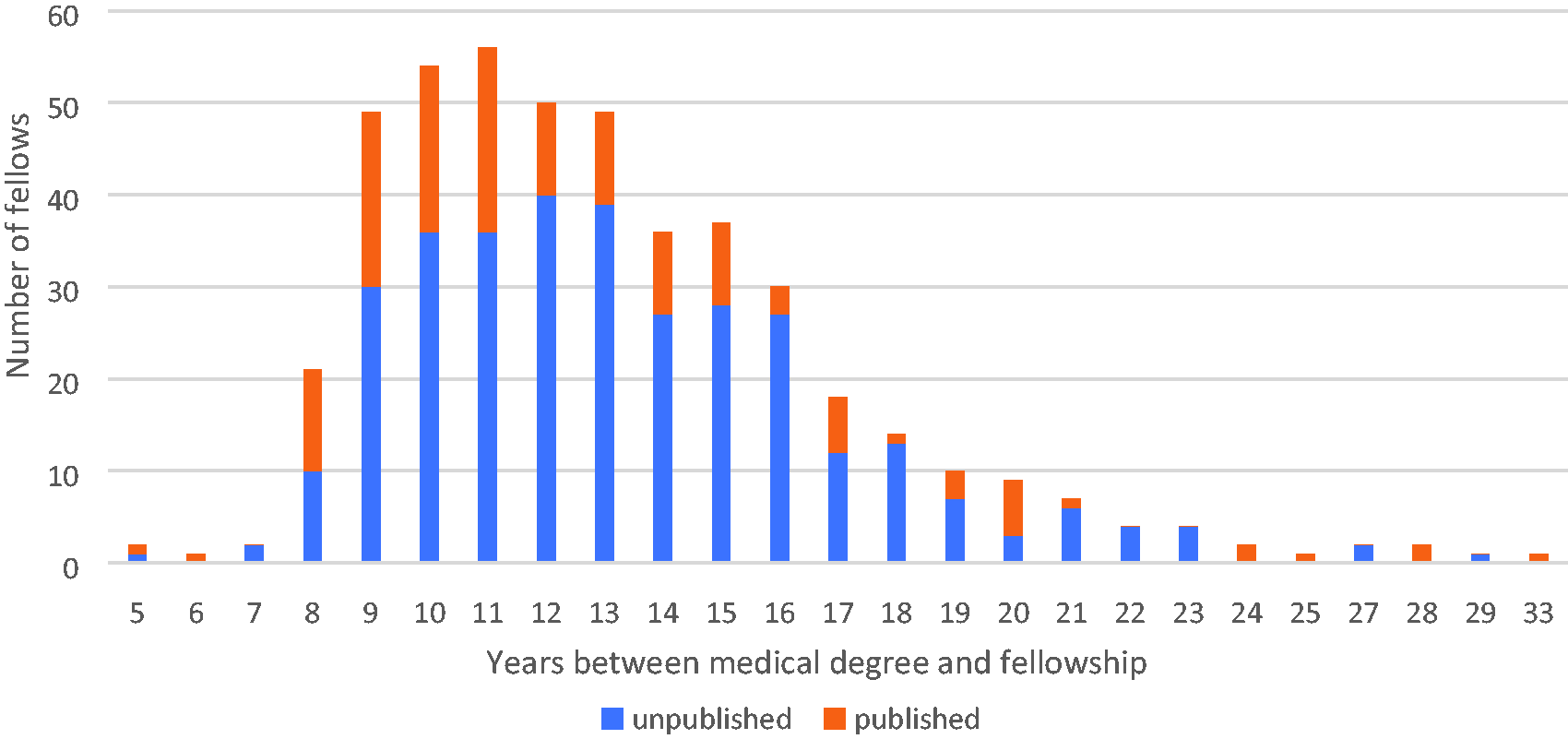
Publication outcome according to time between medical school graduation and fellowship award.
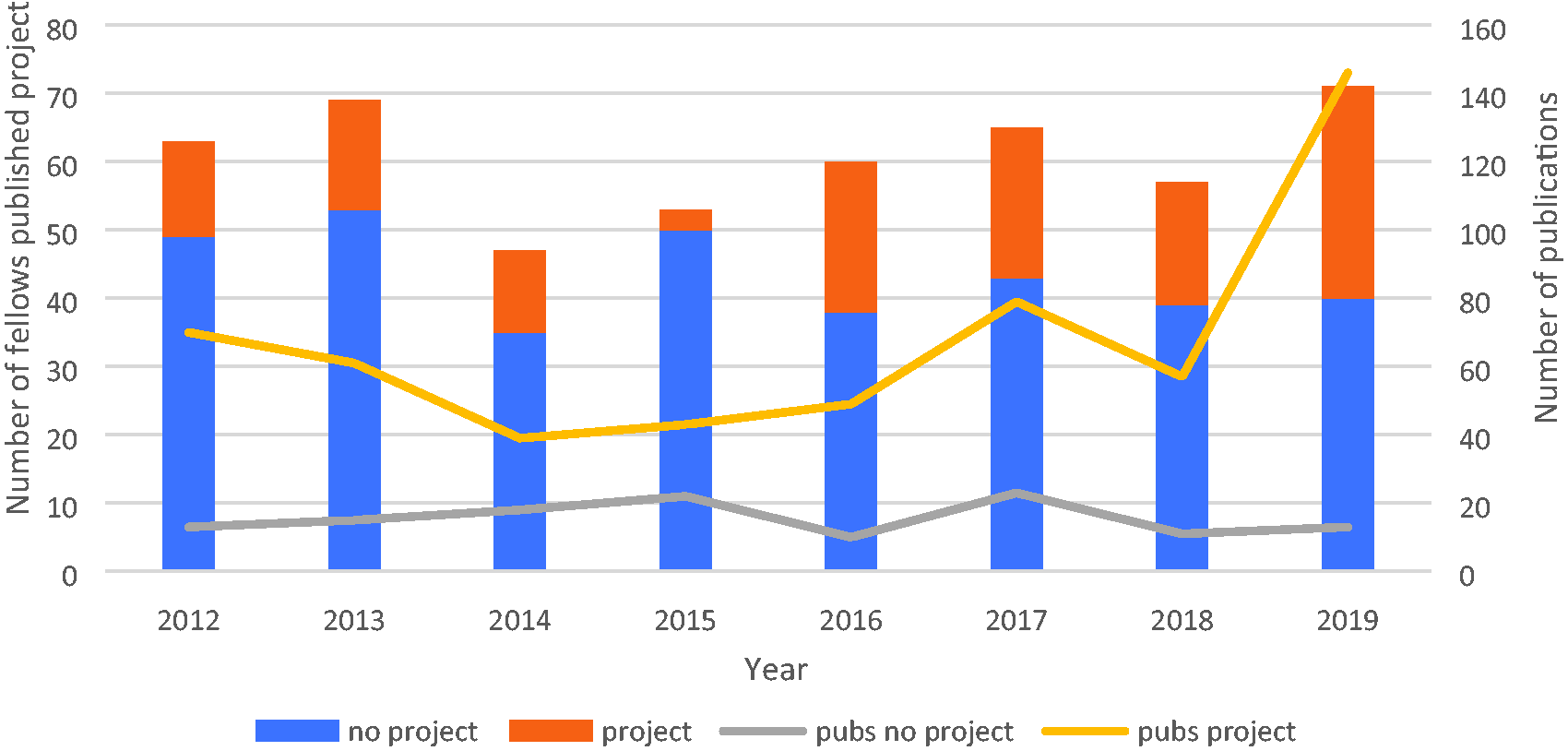
Number of fellows with published projects and total publications by fellowship year (bars represent the number of fellows who had none (blue) or at least one (orange) published (Pubs) project; lines represent total publications by fellows without (grey) or with (yellow) a published project).
Discussion
In this study we report on the research productivity associated with ICU training and found that while there is an average of more than one publication per trainee, less than one-half of individuals have at least one publication associated with CICM fellowship training. In addition, just over one-quarter of trainees have publications that are likely related to the mandatory CICM research project. Furthermore, we identified a number of determinants related to publication output. This study provides novel information about intensive care medicine trainees from Australia and New Zealand and adds to the limited body of knowledge surrounding graduate medical trainee research productivity outside of North American settings.
We observed wide variability in publication productivity associated with CICM fellowship, with most having zero but some with many (e.g. 10 individuals had 10 or more publications). We were unable to compare this productivity with trainees in other regions worldwide due to a paucity of published literature related to intensive care medicine. 7 It is important to note (and shown in Figure 1) that while the majority of CICM fellowships are awarded after a period of postgraduate training that follows medical school graduation, other routes to fellowship may include later career (re)training or ‘grandparenting’ of more senior individuals with recognised foreign credentials who move to Australasia to practise. While ideally all CICM trainees would enjoy success in publishing their research projects, the wide variability observed among trainee productivity is a true reflection of actual eventual practice as they enter clinical careers that may or may not include active research participation.
Although gender and location at the time of fellowship award were not associated, location of receipt of medical degree, shorter time period between medical school graduation and award of fellowship, more recent year of award, and completion of medical degree/fellowship in the same geographical region were associated with project publication. Although previous studies are limited, most that have observed gender differences found that male trainees have higher publication productivity during graduate medical education.12 –17 We did not observe any significant gender differences in our study. It is notable that we observed that both the location of medical school graduation and whether the region of medical school and CICM fellowship were congruent were associated with the research productivity during CICM training (Table 1). Other studies have found that research productivity in medical school and graduation from domestic as compared with foreign medical schools relate to productivity during later postgraduate training.18,19 While we do not have the data to further explore these aspects, we hypothesise that different medical school experiences are influential, and that individuals who remain in a given region over time may have greater opportunities to develop mentoring relationships that in turn lead to research productivity.
The availability of a supportive research environment and access to an experienced mentor is an important determinant of graduate medical trainee research productivity. 7 While the CICM project has specific requirements for its conduct, there are no specified research qualifications that supervisors of these projects are required to have. 8 There is no standardised process for identification and matching of trainees with mentors, and this is variable according to training sites. Further, although mentorship availability has been identified as an issue, we are unaware of any efforts to specifically investigate this issue for CICM trainees.2,20 We observed that most of the senior/mentoring authors of published CICM projects were unique, with a relatively small number of individuals, all of whom were male, that were identified on multiple instances. To our knowledge there are no published articles aimed at defining optimal mentoring opportunities for CICM trainees in Australia and New Zealand.
While this study presents novel information on research productivity among intensive care trainees in Australia and New Zealand, there are some methodological limitations that merit discussion. First, we used only PubMed to identify publications, and as a result productivity assessment is limited to journals that are indexed within its database. Second, we used publications solely as our outcome metric, and accordingly we did not attempt to measure other potentially valuable activities related to the experience of research participation. In addition, we did not evaluate the quality or merit of the individual reports. Third, while we searched for publications in duplicate in an effort to minimise false negatives, we may have failed to ascertain relevant publications as a result of name changes or use of alternate names, or if authors were not included in practitioner registries. Fourth, we elected to use a five-year literature search period and the possibility exists that true CICM project-related publications could have been missed. To address this concern, we performed a post hoc repeat search of all fellows in 2015 to include up to three years of post-fellowship publications and found only one additional potential project in that cohort. Fifth, we did not specifically document papers that may have had more than one CICM trainee as co-authors. Finally, we did not have details on all CICM projects including mentors and study designs such that without this denominator data we were not able to quantify whether these factors were determinants of successful publication.
Conclusion
In this study we report on the research productivity of newly admitted CICM fellows and found that a minority have PubMed-indexed training-associated publications. In addition, we observed that a number of determinants, including location of medical school and fellowship training site, are associated with publication productivity. Further efforts are warranted to better define the determinants of successful project publication in order to optimise future opportunities.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.