
Abstract
A 19-year-old woman with known maple syrup urine disease presented to hospital with metabolic crisis in the setting of influenza type A infection and intractable vomiting, rapidly progressing to acute cerebral oedema manifesting as refractory seizures and decreased level of consciousness needing emergency intubation and mechanical ventilation, continuous veno-venous haemodiafiltration and thiopentone coma. A computed tomography scan and magnetic resonance imaging of the brain demonstrated classic signs of cerebral oedema secondary to a metabolic crisis from the metabolic disorder. Her management posed multiple challenges to all teams involved due to lack of familiarity and experience in managing this clinical scenario in the adult intensive care setting.
Keywords
Introduction
Maple syrup urine disease (MSUD) is an autosomal recessive disorder characterised by deficiency of the alpha-ketoacid dehydrogenase enzyme complex resulting in impaired breakdown of the branched-chain amino acids (BCAAs) that include leucine, isoleucine, and valine. This results in elevated levels of alpha-ketoacids which are toxic protein metabolites, with leucine being highly neurotoxic. Any precipitating factor causing elevation in the levels of these BCAAs can lead to a metabolic crisis. Long-term treatment requires careful manipulation of calories, restriction of dietary BCAAs, and nutritional supplementation with a BCAA-free mixture to provide other essential amino acids thus preventing the breakdown of intrinsic muscle. 1 , 2 We report this patient with MSUD who presented with a severe metabolic crisis leading to refractory cerebral oedema. Management of this patient posed a significant challenge for the adult intensive care unit (ICU) team and the metabolic disorders team due to the unknown and unfamiliar nature of this scenario, and unfamiliarity with MSUD and its metabolic complications in the adult ICU world.
This patient has provided written consent to publish this report.
Case report and management
The patient was diagnosed with MSUD in the first week of her life by routine newborn screening and required 36 hours of continuous veno-venous haemodiafiltration (CVVHDF) for encephalopathy at the time. She was subsequently commenced on a protein-restricted diet with MSUD supplements and had few minor metabolic decompensations in the initial years of her life. She is otherwise fit and healthy and has a plan in place for making dietary changes when unwell.
She presented to a tertiary hospital in early May 2022 with ongoing nausea, vomiting and poor oral intake, secondary to an influenza type A respiratory infection, requiring admission to the hospital for nutritional management. Her dry blood spot (DBS) BCAA test at the time showed leucine levels of 1131 μmol/litre (DBS leucine reference range 53–227 μmol/litre). She was discharged home after 4 days and re-presented to the emergency department within 12 hours with intractable vomiting and intermittent abdominal pain. Her clinical examination was unremarkable, vital signs stable, and abdomen was not peritonitic. She was admitted to a medical ward under the adult metabolic disorders team for closer monitoring and management of her nutritional needs. Insertion of a nasogastric tube was recommended to provide her with the required nutritional support which she initially refused, thus leading to a delay in instituting the appropriate nutrition that was vitally important for her care. She then developed frequent generalised seizures requiring admission to the ICU. Management of ongoing seizures and encephalopathy required emergency intubation within a few hours of ICU admission, and she was noted to have fixed dilated pupils immediately post intubation. This responded to a bolus dose of 10 ml of 23.4% sodium chloride and sedation with strict neuroprotective measures. Adjunct antiepileptic medications were also commenced for management of the seizures. An urgent computed tomography scan of the brain and subsequent magnetic resonance imaging of the brain were suggestive of generalised cerebral oedema classically seen in metabolic crisis secondary to MSUD (see online supplementary material for images and description).
Other acute issues within the first 24 hours of ICU admission included stress-induced cardiomyopathy causing neurogenic pulmonary oedema and a troponin leak of 1652 ng/mL (normal level <17 ng/mL). Initial levels of BCAAs were leucine 1002 μmol/litre (normal range 53–227 μmol/L), isoleucine 493 μmol/litre (normal range 29–125 μmol/L), valine 170 μmol/litre (normal range 93–384 μmol/L) and ammonia 107 μmol/litre (normal level <49 μmol/L).
Key aspects of her management
Management of cerebral oedema and refractory intracranial hypertension
Large doses of sedation, including a thiopentone coma aiming for burst suppression on electroencephalogram, were required. As the cerebral oedema is due to the neurotoxicity associated with accumulation of the ketoacids and leucine, CVVHDF was commenced on day 3 to assist with clearance of these metabolites.3 –8
Nutritional management
The patient’s baseline weight (53 kg) and height (1.51 m) were in the normal range (body mass index 23 kg/m2). Dietetic management consisted of enteral feeds of BCAA-free formulas with supplementary valine and isoleucine along with intravenous dextrose and lipids to provide adequate calories to enable anabolism. Nutrition management was reviewed daily in response to results of DBS BCAA levels, targeting leucine levels of less than 300 μmol/L and isoleucine and valine levels of 200–600 μmol/L.
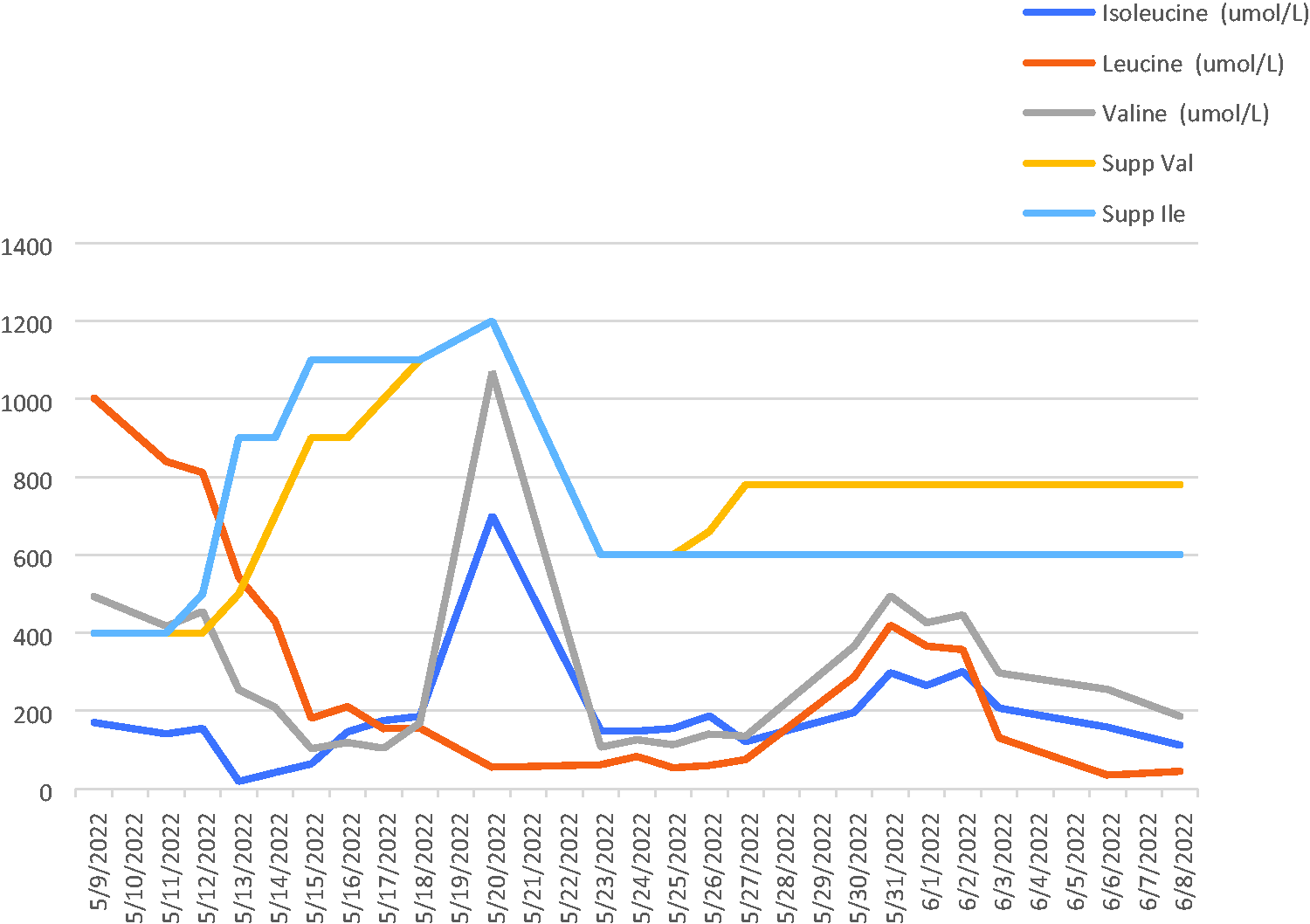
Branched-chain amino acid supplementation versus measured branched-chain amino acid levels during the hospital stay. Supp: nutritional supplementation; Val: valine; Ile: isoleucine.
Dietetic challenges included significant gastric stasis over the first 10 days of ICU admission which limited enteral absorption of nutrients, and blockage of the nasogastric tube by the BCAA-free amino acid formulas. Formulas were switched from MSUD Maximum (a BCAA-free formula) to MSUD Lophlex (a low volume BCAA-free formula) on day 7 to enable better enteral delivery via the nasogastric tube. Both these formulas are specially made to meet the nutritional requirements of teens and adults with MSUD and are supplied by Nutricia Metabolics (a global supplier). Despite changes in the enteral feeding formulas, there were problems with gastric stasis and diarrhoea requiring institution of parenteral nutrition with SMOF lipid (fish oil rich in omega 3 acids, medium chain triglycerides, olive oil and soya oil).3 –5,9 –11 Natural protein was excluded until ICU day 14 and it was re-introduced starting at 3 g daily.
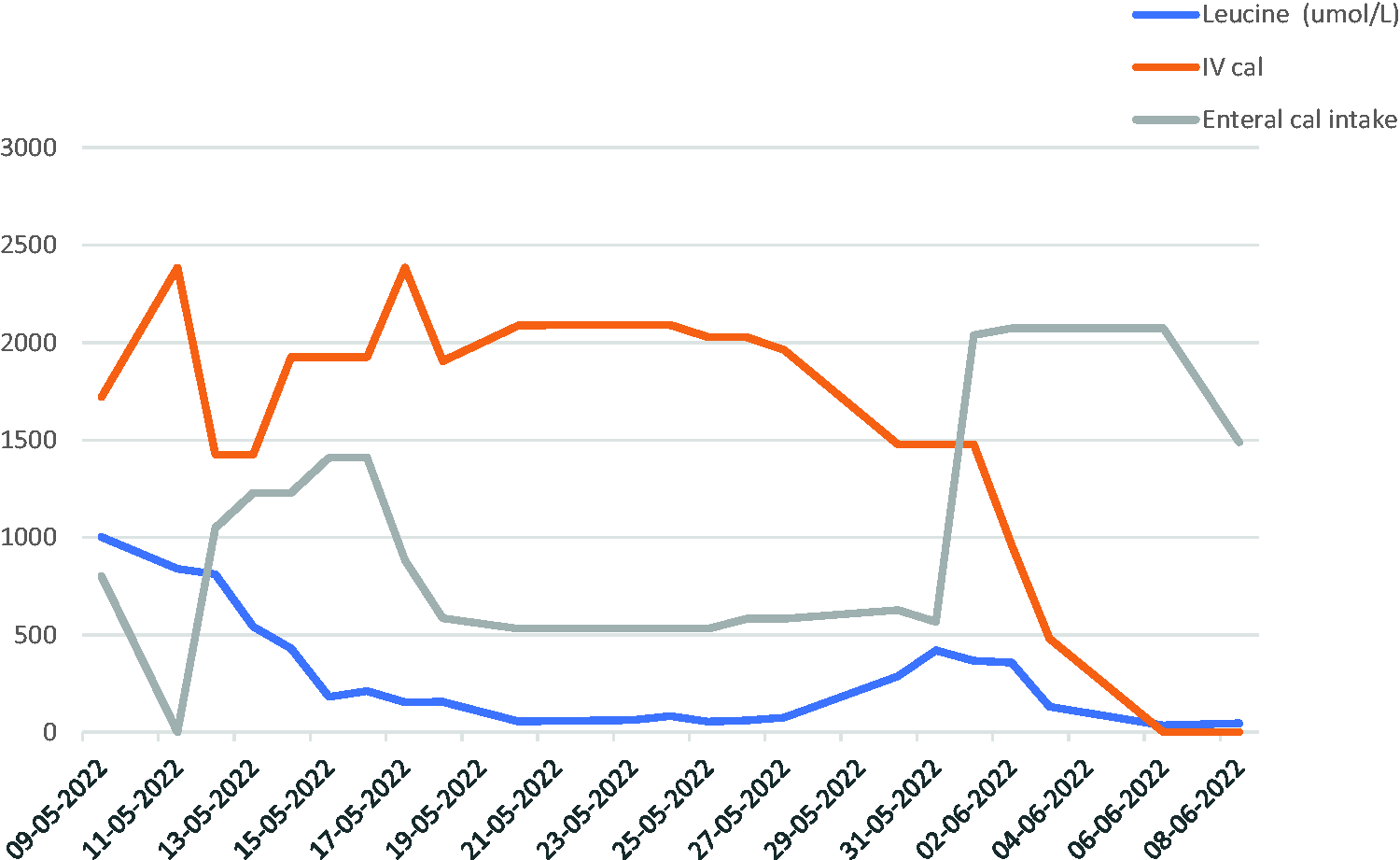
Daily calories provided both enterally and parenterally versus measured leucine levels on a dry blood spot test. IV: intravenous; cal: calories.
Discussion
MSUD is a rare genetic disorder and is part of the spectrum of neurometabolic diseases. Although metabolic decompensations are common, such an extreme form in adults is not encountered commonly. Metabolic crisis can be precipitated by any intercurrent illness that can upset the nutritional balance in the person and these episodes need special attention and diet plans created to prevent a crisis.
Neurometabolic diseases are a group of individually rare but numerous and heterogeneous genetic diseases. The more recently reported adult forms may present with phenotypes strikingly different from paediatric ones and may mimic other more common neurological disorders in adults. Unlike most neurogenetic disorders, neurometabolic disorders can be treated with conventional and more recent novel therapies. However, the phenotypical complexity of this group of diseases and the increasing number of specialised biochemical tools needed can account for significant diagnostic delay and underdiagnosis. 12 ,13 These disorders while rare, should be considered in the differential diagnoses of sudden unexplained encephalopathy in an adult patient who is known to have an underlying metabolic disorder.
With limited experience in managing an acute metabolic crisis in an adult patient with MSUD, the management of this patient was challenging in many ways.
Providing enteral nutrition was confounded by the development of a prolonged ileus precluding establishment of effective gastric feeding and inconsistent absorption of the formula being provided. Total parenteral nutrition was required to provide nutrition while waiting for her ileus to resolve.
The biggest challenge we faced was in managing the neurological manifestations which presented as seizures at the outset but then progressed to the development of diffuse cerebral oedema with intracranial hypertension that was extremely difficult to treat. Conventional sedation and judicious use of muscle relaxants was followed by induction of a thiopentone coma. 14 The evidence for the use of thiopentone in this setting is limited; however, it was used as a rescue therapy to achieve burst suppression. CVVHDF was commenced to clear the toxic ketoacids and metabolites as it is well reported as a treatment modality for such cases in the paediatric world. CVVHDF is effective in clearing non-protein bound low molecular weight molecules by using both convection and haemofiltration. As BCAAs are low molecular weight molecules, use of CVVHDF in this scenario can be beneficial.3 –8
A major confounding factor in instituting and titrating the effect of treatment was a discrepancy in the daily leucine level compared with the clinical manifestations observed. It was noted that despite the leucine levels decreasing exponentially, her clinical signs did not show any significant improvement that should have occurred for the levels measured as per the guidelines and evidence known to us. When we initiated CVVHDF, her leucine levels were not deemed to be in the critical range that would continue to cause ongoing cerebral oedema; however, her clinical signs suggested otherwise. There was clearly a delay in the response to treatment compared with the rate of decline in leucine levels. This was by far the most challenging aspect of her management as it was a new area for the adult ICU and required ongoing collaborative multidisciplinary discussions and literature review to provide the best care for this patient. 15
Managing expectations of her family was also challenging as this was their first contact with the adult hospital environment, and the unfamiliarity and extremely slow progress made it difficult for her parents to develop trust in the adult team physicians. This was managed well by ongoing daily communication with her parents by the ICU and the metabolic teams.
She improved gradually and was extubated on day 17 of her ICU stay. Severe critical illness polyneuromyopathy delayed discharge from ICU and to home.
She was discharged from hospital after 4 weeks of admission. On recent outpatient follow-up she has been able to resume activities of daily life.
Conclusion
MSUD is a rare metabolic disorder, well described in the paediatric world. Metabolic crisis can occur in adults with this condition and may necessitate intensive care support. Unfamiliarity with this disorder and its complications in the adult world can pose significant challenges in the management of an acute crisis in the adult population.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X231183981 - Supplemental material for Metabolic crisis in maple syrup urine disease: an unusual complication of a rare disease: a case report
Supplemental material, sj-pdf-1-aic-10.1177_0310057X231183981 for Metabolic crisis in maple syrup urine disease: an unusual complication of a rare disease: a case report by Hemang P Doshi, Hemal H Vachharajani, Michael C Tchan, Mohamed A Nasreddine and Kate E Billmore in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The authors would like to acknowledge the Department of Genetic Medicine, A/Prof Vineet Nayyar and the Department of Intensive Care Services, Westmead Hospital, Sydney, and Dr Andrew Henderson, neurologist, Westmead Hospital, Sydney for their assistance in management of the case.
Declaration of conflicting interests
The authors declare no conflict of interest with respect to the research, authorship and/or publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.