
Abstract
There are few data on current trends in pain management for thoracic surgery in Australia and New Zealand. Several new regional analgesia techniques have been introduced for these operations in the past few years. Our survey aimed to assess current practice and perceptions towards various modalities of pain management for thoracic surgery among anaesthetists in Australia and New Zealand. A 22-question electronic survey was developed and distributed in 2020 with the assistance of the Australian and New Zealand College of Anaesthetists Cardiac Thoracic Vascular and Perfusion Special Interest Group. The survey focused on four key domains—demographics, general pain management, operative technique, and postoperative approach. Of the 696 invitations, 165 complete responses were obtained, for a response rate of 24%. Most respondents reported a trend away from the historical standard of thoracic epidural analgesia, with a preference towards non-neuraxial regional analgesia techniques. If representative of anaesthetists in Australia and New Zealand more widely, this trend may result in less exposure of junior anaesthetists to the insertion and management of thoracic epidurals, potentially resulting in reduced familiarity and confidence in the technique. Furthermore, it demonstrates a notable reliance on surgically or intraoperatively placed paravertebral catheters as the primary analgesic modality, and suggests the need for future studies assessing the optimal method of catheter insertion and perioperative management. It also gives some insight into the current opinion and practice of the respondents with regard to formalised enhanced recovery after surgery pathways, acute pain services, opioid-free anaesthesia, and current medication selection.
Keywords
Introduction
Thoracic surgery is associated with significant postoperative pain and has traditionally relied on thoracic epidural analgesia (TEA) and opioids for adequate management. 1 Effective management of acute postoperative pain is crucial as inadequate analgesia has been associated with persistent pain up to 6 months after surgery. 2 Persistent post-surgical pain has been shown to occur in approximately 56% of thoracotomy patients. 2 The increasing availability and use of ultrasonography has led to the development of several new fascial plane blocks. These new regional techniques have been adopted and incorporated into analgesic strategies with promising results. 3 Furthermore, there are concerns about a possible link between the use of opioids and an increase in cancer metastases. 4 This fact, along with the inherent adverse effects associated with opioids, has resulted in an apparent trend towards opioid-sparing and opioid-free anaesthesia (OFA), and subsequently a greater reliance on regional analgesia techniques.5,6 Despite the development of these new regional blocks, the impact of ultrasonography and perceptions of anaesthetists towards the use of regional analgesia in their practice has not been investigated in the field of thoracic anaesthesia.
Many earlier surveys into the perioperative analgesic practices in thoracic surgery were conducted more than a decade ago7–9 when thoracoscopic procedures were only beginning to find wider adoption.10,11 A more recent Canadian study from 2018 found TEA was being used by 93% of anaesthetists for open thoracotomy, but only by 40% for video-assisted thoracoscopic surgery (VATS)-assisted lobectomies. 12 A similar shift in practice was not noted by Defosse et al. in 2016, in their survey of German thoracic anaesthetic practice, nor in the recent European Society of Anaesthesiology thoracic survey from 2021.13,14
While a shift towards minimally invasive procedures in thoracic surgery throughout Australia has recently been documented by Wright, 15 there remain limited data on trends in analgesic management associated with this change in practice. The aims of this cross-sectional survey were to understand the current practice in this domain, preferred mode of analgesia, and the perception of anaesthetists towards various modalities of pain management for patients undergoing thoracic surgery in Australia and New Zealand.
Methods
The project was approved by our hospital human research ethics committee and was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12620001210965). The survey questionnaire was developed by the investigators using the Checkbox survey tool (Checkbox Survey Inc., MA, USA, https://www.checkbox.com) centrally supported by the University of Queensland, Brisbane, Australia. The initial draft version of the survey was pilot-tested among five thoracic anaesthetists within our department and circulated among the executive committee members of the Australian and New Zealand College of Anaesthetists (ANZCA) Cardiac Thoracic Vascular and Perfusion Special Interest Group (CTVP SIG) for content, relevance, and time required for completion. All suggestions were incorporated in the final version after discussion. This final version consisted of 22 questions with an estimated 10 minutes required for survey completion.
The final 22 questions, including free-text options, were divided into four sections within the survey (see online supplementary material). The first section (six questions) captured information on the demographics, including practice details of the respondents. The second section consisted of general questions on the pain management programme offered in their respective hospital(s), as well as the participants’ perceptions regarding OFA. Sections three and four were related to the techniques used for intraoperative and postoperative pain management practices. To streamline responses and permit objective interpretation, the responses to the frequency of performing the techniques that were the focus of the questions (questions 15–18, 21, 22) were categorised according to three groups: regular use/practice (always, almost always, most often), occasional use/practice (sometimes) or rare use/practice (often not, almost never and never). Duplicate entries and incomplete responses were removed prior to data analysis.
The survey was approved by ANZCA and a link along with a cover letter was emailed to all members of the CTVP SIG on two separate occasions, initially in December 2020, and again in January 2021. In addition, a final reminder was also sent out with the CTVP SIG newsletter in March 2021. The survey was open for a 4-month period and the last response was obtained on 25 March 2021. Consent to participate was implied by the voluntary completion of the survey. Data analysis was performed using Stata (v17; StataCorp, College Station, TX, USA). 16
Results
Of the total 696 invitations distributed to CTVP SIG members, 165 complete responses were obtained reflecting a response rate of 24%. Of the 165 respondents’ location of practice, 26% were from New South Wales (n = 42). The primary practice environment for the majority of the respondents was tertiary hospitals (n = 150, 91%). Most of the respondents were anaesthetists with over 10 years in clinical practice (n = 118, 72%) and nearly 40% of the participants (n = 65) had over 20 years of experience. Approximately 56% of respondents worked in public hospitals while 26% had a mix of public and private practices. Most respondents (n = 108, 65%) had either regular weekly or fortnightly thoracic surgical sessions, with a median of five (interquartile range (IQR) 3–8) cases handled per month overall (Table 1).
Demographics and practice profile of the survey respondents.
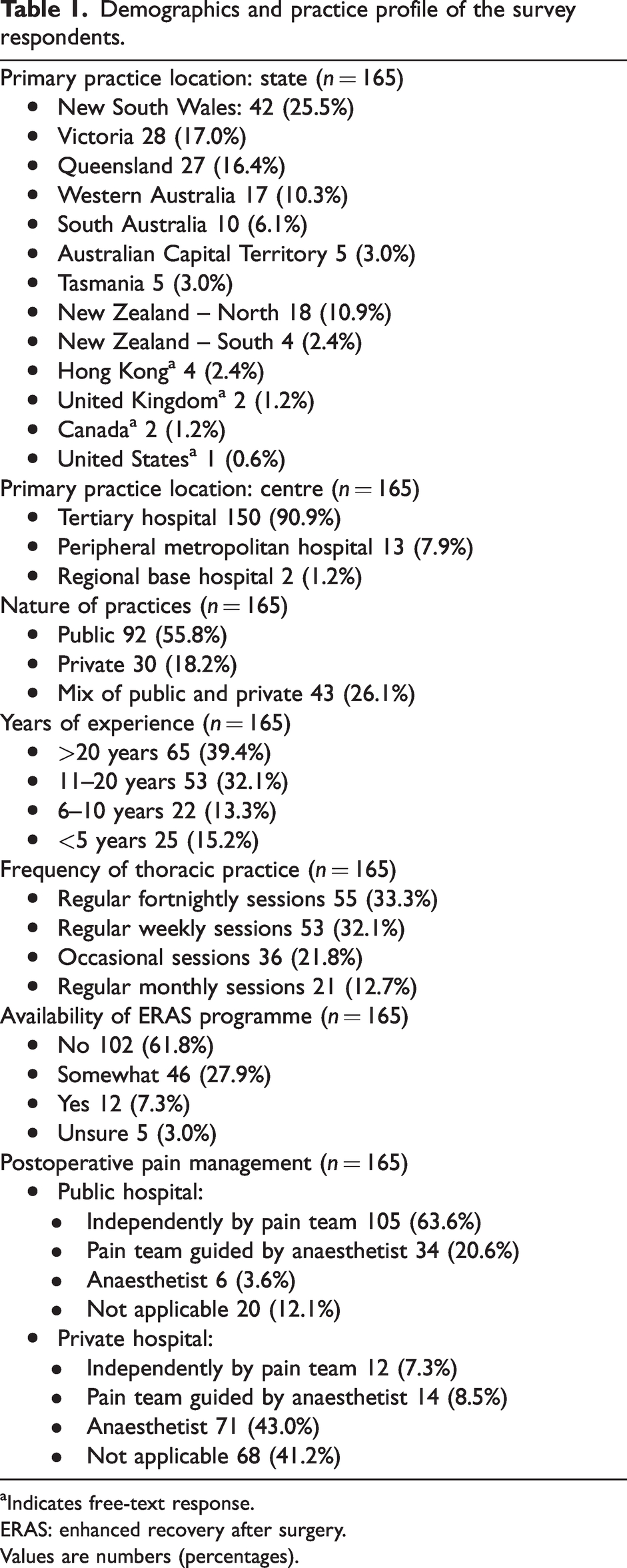
Indicates free-text response.
ERAS: enhanced recovery after surgery.
Values are numbers (percentages).
Practice location profile
Twelve participants (7%) indicated that their primary practice location currently had an enhanced recovery after surgery (ERAS) programme in place. Conversely, 102 (62%) did not have such a programme, while 46 (28%) indicated that some elements of ERAS were implemented at their place of practice. Public hospital systems had a dedicated pain management team overseeing postoperative pain management for the majority (139/145, 96%), in comparison with private hospitals where postoperative pain consultations were limited (26/97, 27%) (see Table 1).
Analgesic management for thoracic surgery
Of the 165 survey respondents, 158 participants identified themselves as regularly providing anaesthetic care for major thoracotomy operations including pneumonectomy. Among them, the most common primary method of intraoperative analgesia for this procedure was regional anaesthesia with or without opioid supplementation (n = 91, 58%). We found most thoracic anaesthetists now utilise non-neuraxial techniques in the management of pain following major thoracotomy, with only a quarter of respondents relying on the historic gold standard of thoracic epidural-based analgesia (n = 41/158, 26%) for pneumonectomies (see Table 2).
Primary method of intraoperative analgesia and the most common regional technique for thoracic surgical procedures (n = 165).

This did not include local infiltration by surgeons.
VATS: video-assisted thoracoscopic surgery.
Values are numbers (percentages).
A similar trend in analgesic practice was observed across other major thoracic procedures. Regional techniques with or without opioid supplementation were the most common analgesic plans for the anaesthetists regularly managing mini-thoracotomy (n = 114/161, 71%) and major VATS (n = 111/162, 69%).
Of the specific procedures assessed, the highest rate of TEA use was observed with lung volume reduction surgery (LVRS) at 35% (n = 24/69). However, only 40% of the survey participants (n = 69/165) were regularly involved with this procedure.
Analgesic management of VATS minor procedures demonstrated a wide variation in standard practice among respondents. Of the anaesthetists who regularly managed VATS minor procedures, non-neuraxial regional techniques were utilised for intraoperative analgesia by 56% (n = 92/162), while 43% of anaesthetists (n = 69/162) implemented an opioid-based analgesic plan without regional or neuraxial techniques. Only one respondent indicated TEA as their analgesic technique of choice for these procedures.
Preferred non-neuraxial regional techniques for analgesia
Among the study respondents whose regular practice included major thoracotomy (n = 158), surgically placed paravertebral/extra-pleural catheter was the most commonly utilised technique, followed by TEA (n = 41). The trend towards reliance on surgically placed regional catheters as the primary analgesic modality was consistent across most thoracic procedures assessed—including mini thoracotomy (n = 77), major thoracoscopic surgery (major VATS) (n = 73) and minor thoracoscopic surgery (minor VATS) (n = 46). In fact, the use of surgically placed catheters was the most common regional technique for all procedures assessed, with the exception of LVRS (n = 25) and sub-xiphoid procedures (n = 16), in which it ranked second (see Table 3).
Subgroup analysis of non-neuraxial regional techniques.
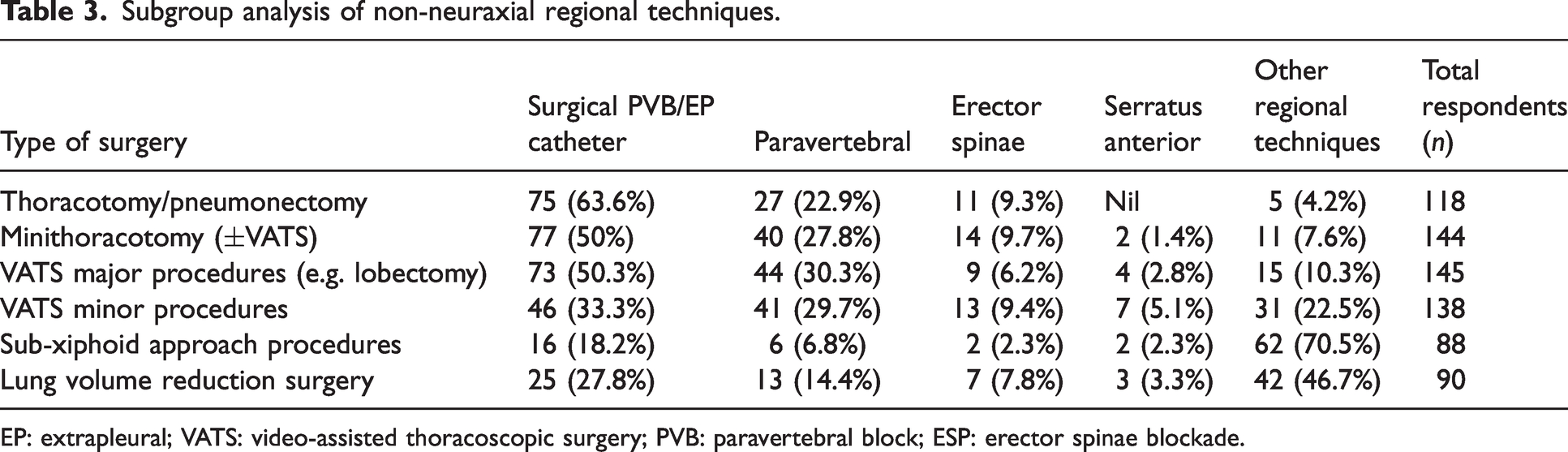
EP: extrapleural; VATS: video-assisted thoracoscopic surgery; PVB: paravertebral block; ESP: erector spinae blockade.
Of non-neuraxial regional techniques performed by anaesthetists for the management of major thoracotomy-related pain, paravertebral blockade (PVB), either single-shot or by continuous infusion through a catheter, was the most utilised method (n = 27), followed by erector spinae plane (ESP) blockade (single-shot or continuous, n = 11). For minor VATS procedures, PVB remained the most utilised technique overall (n = 87, 53%), with a nearly equal distribution between surgically versus anaesthetically placed blocks (28% vs. 25%, respectively).
Use of ultrasound imaging for guiding regional techniques
Among those anaesthetists who regularly perform regional anaesthesia, ultrasound utilisation was most common in the performance of ESP blocks and least common for TEA. The greatest variation in ultrasound use among responding anaesthetists was found with PVB in which approximately 41% (42/103) of proceduralists reported frequent use, 44% reported rare use (44/103) and 16% (17/107) stated only occasional use (see Table 4).
Frequency of participants use of ultrasound with various regional techniques (n = 165).
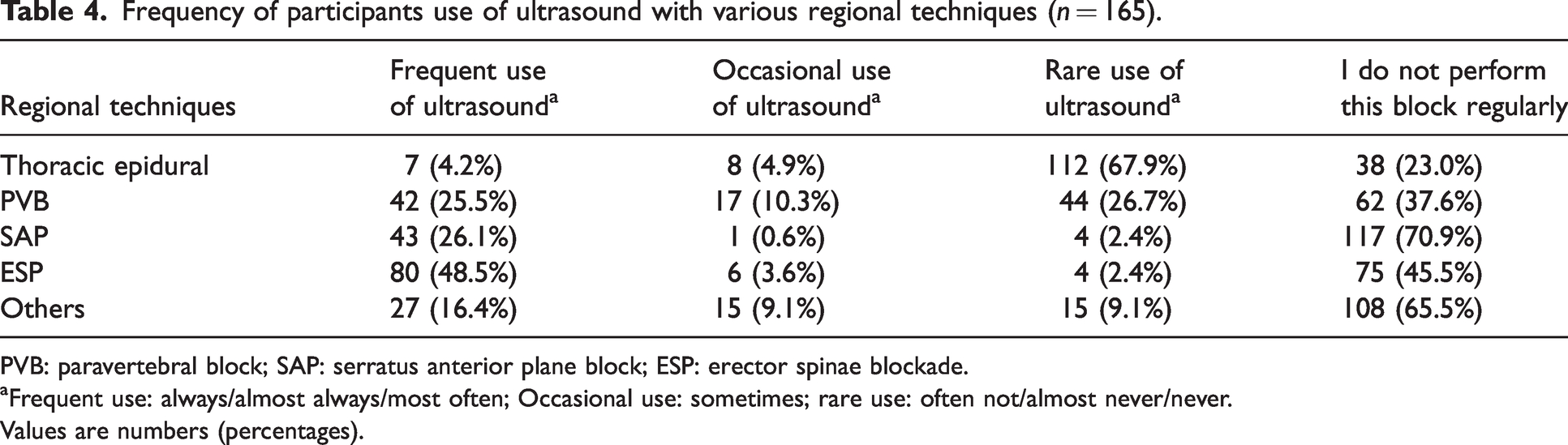
PVB: paravertebral block; SAP: serratus anterior plane block; ESP: erector spinae blockade.
Frequent use: always/almost always/most often; Occasional use: sometimes; rare use: often not/almost never/never.
Values are numbers (percentages).
Barriers to changing practice
Participants were asked whether, taking external factors into account, they would change their most common method of intraoperative analgesia for an alternative, or more preferred method, and to identify barriers to change. Of the 161 respondents, 86 (53%) stated that they would not change their current practice. Of the remaining 47% who stated that they would consider a change to an alternative analgesic plan, the most common external factors identified were time pressure (n = 25/161, 16%), the influence of surgical preference (n = 31/161, 19%) and the adequacy/availability of postoperative infrastructure (i.e. 24-hour pain service, skilled nursing and monitored care) (n = 23/161, 14.3%). Other less common responses were the availability of alternative equipment (n = 8/161, 5.0%), and restrictive local guidelines (n = 20/161, 12%). The free-text responses collated suggest the analgesic technique employed by respondents, in their opinion, is based on the latest evidence and pain outcomes.
Preferred systemic medication choices for intraoperative and postoperative analgesia
Opioids were the most used medication for intraoperative and postoperative analgesia, followed by paracetamol and anti-inflammatory medications in decreasing order. Adjuncts such as ketamine, alpha-agonists (clonidine and dexmedetomidine) and weak opioid agonists (tramadol and tapentadol) were occasionally used. Nearly 93% (n =154/165) stated they rarely use nitrous oxide. Interestingly, we noted that intraoperative magnesium and lidocaine were not popular among the responding thoracic anaesthetists, with around 60% reporting rare intraoperative use. Approximately 50% of the respondents indicated that they regularly used ketamine intraoperatively, while 40% stated they rarely used ketamine postoperatively. Other uncommonly utilised postoperative analgesics were intravenous lidocaine, clonidine, dexmedetomidine, and the gabapentinoids.
Most of the respondents (n = 113/165, 69%) indicated that they regularly used opioid intravenous patient-controlled analgesia to supplement regional or neuraxial techniques. A small number of respondents reported by free text the use of methadone, tricyclic antidepressants, intercostal nerve blocks and regional block catheters with local anaesthetics for postoperative analgesia (see Table 5).
Preferences on the intraoperative and postoperative pain medications in participants’ routine clinical practice for thoracic surgery (n = 165).
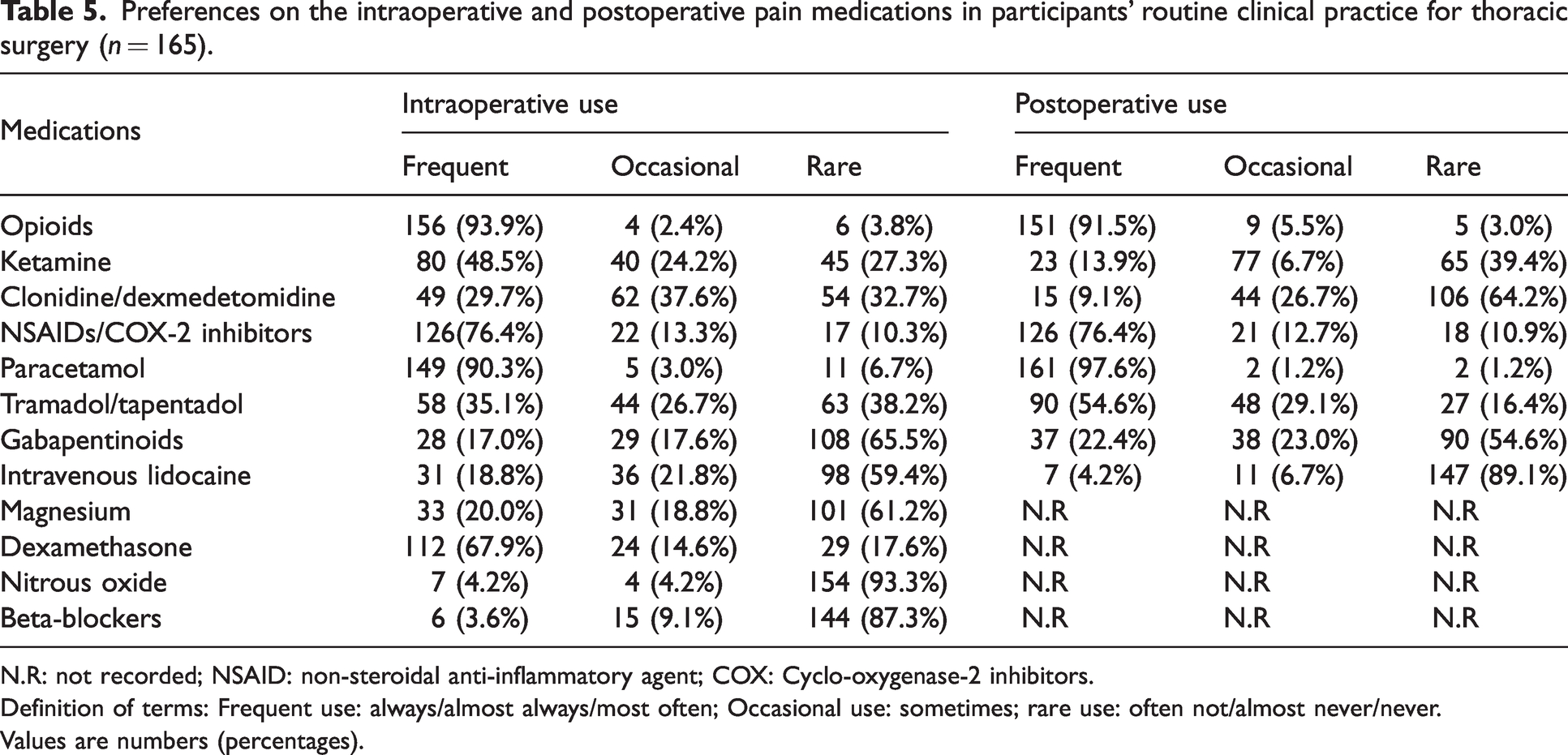
N.R: not recorded; NSAID: non-steroidal anti-inflammatory agent; COX: Cyclo-oxygenase-2 inhibitors.
Definition of terms: Frequent use: always/almost always/most often; Occasional use: sometimes; rare use: often not/almost never/never.
Values are numbers (percentages).
Practice of opioid-free anaesthesia
Most of the participants (146/165 (89%)) stated that they rarely practised OFA for thoracic procedures. When asked to preference reasons given for not adopting OFA, a lack of robust evidence to support the practice of OFA (n = 92) was the most selected answer, followed by the belief that OFA is impractical, as opiates are unavoidable during the perioperative period (n = 75). By way of a free-text response, several respondents indicated that they would prefer an opioid-sparing technique rather than OFA. The most commonly (84%) selected response for undertaking OFA was the avoidance of immediate complications and adverse effects associated with opioid use (see Table 6).
Perceptions towards OFA for thoracic procedures (n = 165).
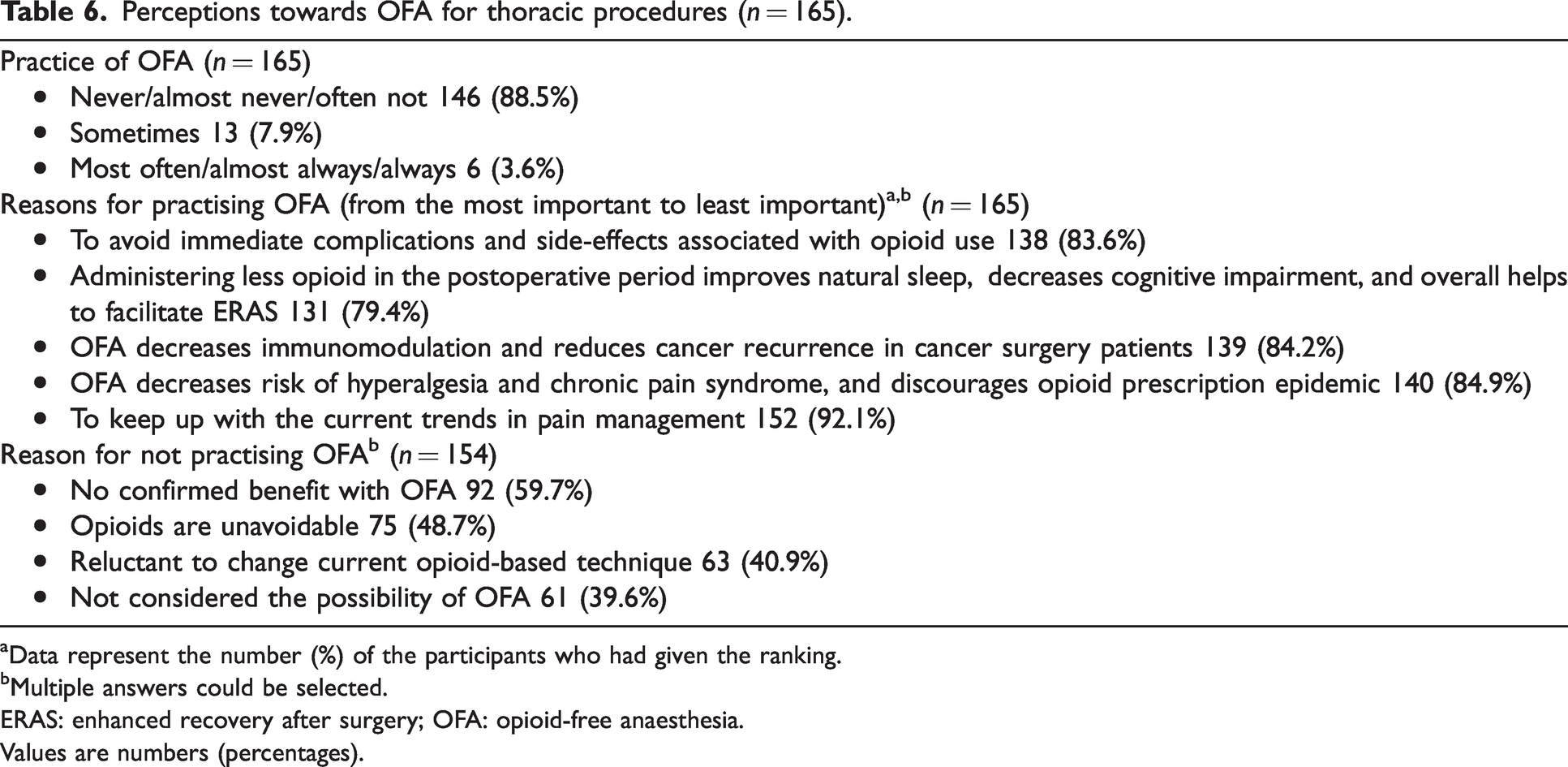
Data represent the number (%) of the participants who had given the ranking.
Multiple answers could be selected.
ERAS: enhanced recovery after surgery; OFA: opioid-free anaesthesia.
Values are numbers (percentages).
Phrenic nerve block and ipsilateral shoulder pain
The performance of phrenic nerve blockade by the surgeons was observed to be a rare practice as indicated by most of the participants (145/165 (88%)). Of the 165 respondents, 141 (86%) were unsure of the effectiveness of phrenic nerve block in preventing or reducing postoperative ipsilateral shoulder pain (ISP). Of the 136 who responded, 77 (57%) reported that they do not face difficulties in treating ISP with alternative analgesic modalities.
Discussion
Our survey of thoracic anaesthetists from Australia and New Zealand highlights a considerable shift in the pattern of pain management practices among respondents, compared with those documented in previous surveys.7–9 This study is the first survey in the past 25 years of anaesthetists in Australia and New Zealand regarding analgesic management of pain related to thoracic surgery. The survey response rate of 24% (165 of 696 invitations), however, falls below the calculated sample size for categorical data of 249 required for a type I margin of error of 0.05 outlined by Bartlett et al. 17 It also cannot exclude the possibility of responder bias, which is not taken into consideration in the estimation of Bartlett et al. 17 Nevertheless, it is larger than the previous work by Cook and Riley, 7 which recorded a sample size of only 24 in the last published survey of Australian practice in this field dating back to 1997. As a result of the low response rate, interpretation and extrapolation of the trends represented in our data must, however, be done with caution.
Thoracic epidural analgesia
Historically, TEA has always been considered the gold standard for its effective analgesia, and its positive effect on respiratory mechanics that decreases the likelihood of mechanical ventilation and respiratory complication rates following major thoracotomy. 18 Our study noted an overall reduction in the administration of TEA for major thoracic operations among survey respondents, with only a 35% utilisation for LVRS and an even lower rate of 25% for thoracotomy. Conversely, regional techniques with or without opioids were preferred to thoracic epidural for major thoracic surgery, thoracotomy or thoracoscopic procedures. This is in contrast to the last survey of Australian thoracic anaesthetists by Cook and Riley in 1997, which documented TEA as the most common post-thoracotomy analgesia technique. 7
Similar low rates of epidural use were also noted in a recent survey of Australian anaesthetists managing major abdominal surgery. 19 If these two findings are representative of a greater shift in practice throughout Australia and New Zealand there may be significant implications, especially for young or trainee anaesthetists. Overall reduced exposure to TEA may result in reduced proficiency or confidence in the technical skills required for placement and the knowledge necessary for safe ongoing postoperative management. These implications would extend beyond the anaesthetic team directly, and onto nursing and critical care staff typically involved in the perioperative monitoring and management of patients receiving TEA.
The recently released PROSPECT guidelines for VATS reflect a similar shift away from TEA. 20 While previous guidelines had advocated for consideration of all regional anaesthetic options,21,22 the current PROSPECT guidelines recommend against the use of TEA. Therefore, ongoing monitoring of current practice in this area in response to such a recommendation would appear essential.
Internationally, TEA use remains prominent, with a 2010 survey of cardiothoracic anaesthetists in the UK identifying TEA as the most popular analgesic option for thoracic surgery. 9 Approximately 60% of respondents preferred TEA, compared with one-third preferring PVB for lobectomy or pneumonectomy. 9 Consistent with this finding, another UK-based survey found TEA to be the main technique for open thoracic procedures; however, PVB with intravenous patient-controlled analgesia morphine was the most common regional technique for VATS lobectomy. 8 While this may be explained by the higher number of open thoracotomy procedures (vs. VATS) in the past, a more recent UK single-centre audit from 2017 reported a 95% (289/306) epidural rate among thoracotomy patients. 2 Furthermore, high rates of TEA utilisation (83%) were also reported in the recent 2021 European Society of Anaesthesiology and Intensive Care (ESAIC) survey of more than 500 respondents. 14
Surgically placed paravertebral catheters
PVB has previously been demonstrated to be as effective as TEA for relief of postoperative pain following thoracotomy, but with a more favourable safety profile especially with difficult anatomy and coagulation disturbances.23,24 Among our survey respondents, PVB was rated as the most preferred among the regional analgesic techniques for intraoperative pain management. This trend is a notable departure from the historic data collected by Cook and Riley in 1997 that noted paravertebral and interpleural blockade was used ‘never/rarely’ in all but two of the 26 Australian hospitals surveyed. 7 Similar trends were not demonstrated in the 2018 survey of Canadian anaesthetists, nor the 2021 ESAIC survey which reported rates of PVB catheter use of less than 5% and 15.3%, respectively.12,14
Interestingly, we found that surgical placement of PVB catheters was more common than PVBs performed by the anaesthetists (46% vs. 16%). This practice is consistent with previous reports from both the UK and Canada, where preference towards surgical placement was reported to be as high as 90%.8,9,12 Surgical placement of PVB catheters may be associated with a lower rate of complications as placement is done under direct vision, and it also provides the option for placement at the end of surgery once the scope of the operative intervention is known.12,25 As has previously been noted elsewhere, 21 there is a lack of evidence comparing the efficacy of these insertion techniques for non-inferiority, which would appear warranted if the trends illustrated by our survey responses are representative.
Phrenic nerve infiltration for ipsilateral shoulder pain
In an Australian single-centre study, the incidence of significant ISP following thoracotomy was observed to be 16% despite phrenic nerve infiltration. 26 The same study reported no episodes of significant ISP in patients who underwent VATS with the use of phrenic nerve infiltration, but the overall sample size was low (n = 7). Our survey indicated that the practice of phrenic nerve infiltration as a prophylaxis for ISP was not common.
Ultrasound guidance for regional anaesthesia
Even though there is consistent evidence to suggest that neuraxial ultrasound is superior to palpation of surface anatomical landmarks for the identification of intervertebral levels 27 most survey respondents indicated rare use during thoracic epidural placement. The utilisation of ultrasound for non-neuraxial techniques was much higher, with frequent use being reported by more than 40% of respondents for all techniques assessed. Interestingly, the availability of equipment (including ultrasound machines) was cited by a minority as one of the factors influencing their intraoperative analgesic management plan. In line with this, a recent Canadian survey from 2019 also found the lack of ultrasound machines to be a major impediment to increased utilisation by anaesthetists performing regional anaesthesia. 28
Opioid-related adverse effects including respiratory depression, opioid misuse, opioid-induced hyperalgesia, and potential association with cancer progression have all been identified as possible limitations to their use in perioperative medicine. 29 As opioid-related adverse effects are multifactorial and dose dependent, there is conflicting evidence on the ideal safe alternative. To this end, OFA remains a therapeutic dilemma and a concept which is still ill-defined.29–31 Hence, unsurprisingly, despite the appreciation of the need to reduce opioid-related side-effects, most of our participants (81%) did not advocate the use of OFA. However, OFA is being trialled as an emerging technique in thoracic surgery with some promising results. 6
Considering that the previous Australian survey was nearly a quarter of a century ago, our survey reflects the current analgesic practice patterns for thoracic surgery among the anaesthetists from Australia and New Zealand. It also identifies salient differences in analgesic management as compared with current practice throughout Europe and the UK. Given the increasing prevalence of ultrasonography and trends towards limiting opioid use with multimodal analgesia, our findings may act as a benchmark for future studies.
Limitations
As previously mentioned, there are several notable limitations to the present survey, primarily associated with the overall low response rate of 24%. This low sample size may be associated with a non-response bias, wherein a systematic difference in characteristics between responders and non-responders exists. 32 Therefore, we are limited in our ability to extrapolate the data presented above, and perform more inferential analysis.
Furthermore, incomplete responses did not contribute to the final data pool, as we could not be confident to identify and exclude duplicate entries that would result from repeated attempts at the online survey. This fact was a consequence of our method of distribution and the decision to collect our survey responses in a de-identified manner. Published response options were determined based on consensus—after discussion among the investigators and in consultation with expert opinion. As the list of options may not have been exhaustive, the option for free-text responses was included.
In addition, the survey design required mandatory completion of all questions in order to submit. This in some areas may have influenced the response pattern of individuals—with respondents contributing data to procedures with which they are not familiar or do not currently practise (e.g. question 14).
Future directions
We hope that our survey results will create a reference point to track changes in the practice of thoracic anaesthesia throughout Australia and New Zealand. In particular, it will be interesting to monitor the use of neuraxial anaesthesia compared with the now prominent surgically placed paravertebral catheters over time.
In addition, future iterations could seek to analyse regional differences in practice, or the effect that clinical experience has on survey responses, by grouping answers according to these key demographics. Monitoring the use and utilisation of ultrasound with regional techniques will also be of interest as ultrasound machines become more easily and widely available.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X231172787 - Supplemental material for Perioperative pain management in thoracic surgery: A survey of practices in Australia and New Zealand
Supplemental material, sj-pdf-1-aic-10.1177_0310057X231172787 for Perioperative pain management in thoracic surgery: A survey of practices in Australia and New Zealand by Michael J Busser, Shakeel M Kunju and Usha Gurunathan in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The authors would like to thank Dr Stephanie Yerkovich, Ms Sarah Chezhan, Ms Karen Goulding and members of ANZCA CTVP SIG executive committee for their assistance and support during this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.