
Abstract
Objective
Manipulating the instruments during uniportal video-assisted thoracoscopic surgery (U-VATS) bullectomy requires a relatively large incision. This study aimed to investigate the feasibility of next-day discharge following U-VATS bullectomy using an anchoring suture.
Methods
A stapler and a scope were inserted through a single incision in the anchoring group. The bullae were retracted by the suture, which was inserted from outside of the chest wall into the thorax, and then bullectomy was performed. For those in the control group, resection of the bullae was performed with the assistance of a grasping forceps.
Results
The length of the incision of the patients in the anchoring group ([13.2 ± 2.2] mm) was significantly smaller than in the control group ([26.2 ± 3.9] mm). In addition, the number of staplers used in the anchoring group was significantly less than in the control group ([1.2 ± 0.4] vs. [1.4 ± 0.5]). Furthermore, 36 (92.3%) cases in the anchoring group were uneventfully discharged within 24 hours after bullectomy.
Conclusion
Next-day discharge after U-VATS bullectomy through a small incision assisted with an anchoring suture is safe and feasible.
Keywords
Introduction
Uniportal video-assisted thoracoscopic surgery (U-VATS) bullectomy has been utilized widely for primary spontaneous pneumothorax (PSP). However, the major concern of this procedure is the collision between the surgical instruments and the thoracoscope, which usually requires a large incision (>20 mm). Therefore, a modified technique for minimally invasive resection of bullae is needed.
The reported method for retraction of the target bullae for resection using an anchoring suture was used, 1 and a small access (with a mean length about 15 mm) was created for U-VATS bullectomy in our hospital starting in August 2015. Most of the patients were discharged uneventfully from the hospital within 24 hours after the surgery. The aim of this study was to evaluate the effectiveness and the potential advantages of next-day discharge after U-VATS bullectomy assisted with an anchoring suture.
Patients and methods
Patient selection
We retrospectively reviewed patients who underwent a U-VATS bullectomy with or without an anchoring suture by the same surgeon between August 2015 and December 2018. Inclusion criteria included the following: (1) recurrent pneumothorax after prior medical treatment; (2) patients whose lung collapse exceeded 30% estimated by chest x-ray, and obvious bullae were identified on computed tomography (CT) images; (3) persistent air leak longer than 1 month after chest tube drainage; (4) patients with normal hematology, electrolytes, and liver and kidney function; (5) patients understood the risk of U-VATS such as conversion and bleeding, and voluntarily provided written informed consent. Exclusion criteria were as follows: (1) patients were afraid of the potential risks and refused U-VATS; (2) estimated severe pleural adhesion due to history of thoracic surgery; (3) spontaneous pneumothorax secondary to diffuse emphysema, asthma, fibrosis, thoracic injury, 2 tuberculosis, and malignancy; (4) no significant bullae on CT images, and the chest tube drainage with or without medical pleurodesis was effective; (5) inability of the patients to provide informed consent. This study was approved by the Ethics Committee and Institutional Review Board of Shaoxing People’s Hospital (SXPH-ZJ-20190701-014, July 21, 2015). Informed written consent was obtained from every patient or their parents or caregivers before the surgical treatment.
Surgical technique
All of the patients enrolled for bullectomy underwent a CT scan to identify the location and size of the bullae, which were not adequately visible on chest x-ray. The surgery was performed step-by-step. For the patients in the anchoring group, a small incision of about 15 mm was created. The bullae were identified using a 30°, 5-mm-diameter thoracoscope through the incision, and a 1-0 silk suture was passed from outside of the chest wall into the thorax for bidirectional traction of the bullae (Figure 1). Next, the bullae were lifted by pulling the suture to create an angle, and then a surgical stapler (Ethicon, Cincinnati, OH, USA) was inserted and fired to complete the bullectomy. Conversion to two-port/three-port VATS or extension of the surgical incision was considered if there was a severe pleural adhesion.

The operative technique of U-VATS bullectomy assisted with an anchoring suture. (a) A silk suture was passed from outside of the chest wall into the thorax through the third or fourth intercostal space, and the target bullae for resection were located and retracted by the anchoring silk. Then the needle was pulled out through the surgical incision. (b) The bullae were lifted by pulling the suture on the side of the chest wall and the surgical incision to create a resection angle, and then a wedge resection was performed using the endo-staplers. (c) The bullae located in the apex of the lung were retracted using an anchoring silk by the assistant surgeon. U-VATS, uniportal video-assisted thoracoscopic surgery.
In addition, mechanical pleurodesis was performed by pleural abrasion using sterile gauze from the apex of the thorax to the sixth rib for some patients, without standard criteria for patient selection. Finally, the wound was closed after the insertion of a 14-French chest tube through this incision into the pleural cavity, 3 and the incision length was measured.
For the patients in the control group, the grasping forceps were used instead of an anchoring suture for retraction of the bullae, which resulted in a larger surgical incision for the insertion of the instruments and thoracoscope.
Moreover, ultrasound-guided serratus anterior plane block (SAPB) was performed for postoperative pain control after closure of the surgical incision 4 using 0.2% bupivacaine (Marcaine, AstraZeneca, UK) at a dosage of 0.3 mL/kg of body weight.
The visual analog scale for pain
The postoperative pain of the patients was evaluated using the visual analog scale (VAS) score in a range of 0 to 10, with 0 representing no pain and 10 representing unbearable pain. In case of discharge within 3 days, the patients’ pain VAS was obtained by remote interview using a smart phone.
The operative time, estimated blood loss during surgery, duration and total volume of postoperative chest drainage, surgery-related complications, pain VAS on postoperative day (POD) 1 to 3, and postoperative hospital stay of the patients in the two groups were compared.
Statistics
Descriptive continuous variables were recorded as means and standard deviations (SD) and were analyzed using Student’s unpaired t-test and one-way analysis of variance (ANOVA) as appropriate. The pain VAS between the groups was compared using repeated-measures ANOVA. Categorical variables were assessed by Fisher’s exact test and Pearson Chi-square test. The statistical analysis was performed using SPSS version 19 (IBM Corp., Armonk, NY, USA). A p-value less than 0.05 was considered statistically significant.
Results
Seventy-nine PSP patients were enrolled and were divided into the control group (40 cases) and the anchoring group (39 patents). The two groups had similar baseline characteristics except for age distribution (Table 1).
Baseline characteristics of the patients.

Note: Age was shown as the mean ± standard deviation (SD). n, number.
The surgical outcomes are shown in Table 2. Conversion to thoracotomy, perioperative mortality, hemothorax, and recurrence were not observed in this cohort. Two patients in the control group were converted to multi-port VATS, while there was no patient in the anchoring group that needed an additional surgical incision. The incision length of the patients in the anchoring group ([13.2 ± 2.2] mm) was significantly shorter than in the control group ([26.2 ± 3.9] mm, p < 0.05). Moreover, the number of staplers used in the anchoring group was significantly less than in the control group ([1.2 ± 0.4] vs [1.4 ± 0.5], p < 0.05).
Perioperative parameters of the patients who underwent U-VATS bullectomy.

U-VATS, uniportal video-assisted thoracoscopic surgery; n, number; VAS, visual analog scale.
In addition, 36 (92.3%) cases in the anchoring group and one (2.5%) patient in the control group were discharged within 24 hours after the operation. The chest tube duration of the patients in the anchoring group was noticeably shorter than in the control group ([1.6 ± 2.1] days vs. [3.2 ± 1.7] days, p < 0.05). Moreover, the total drainage volume of the patients in the anchoring group was also significantly less than in the control group ([110.8 ± 161.1] mL vs. [276.3 ± 133.5] mL, p < 0.05).
The patients’ VAS of pain in the anchoring and the control group on POD 1, 2, and 3 were ([2.6 ± 0.8] vs. [2.9 ± 1.1]), ([2.1 ± 0.9] vs. [2.4 ± 0.9]), and ([2.4 ± 0.9] vs. [2.7 ±0.7]), respectively, with a statistical difference between the two groups (p < 0.05). Furthermore, the patients did not have a difference in terms of the operative time, estimated intraoperative blood loss, or the incidence of surgery-related complications.
Discussion
U-VATS bullectomy through a small incision assisted with an anchoring suture in 39 patients was successfully performed in this cohort study, of which 36 (92.3%) were discharged uneventfully on POD 1.
Surgical resection of the bullae is recommended for patients with recurrent or complicated pneumothorax. 5 Additionally, it may be the standard of care when high-resolution CT reveals significant bullae ≥2 cm in size. 6 A review indicates that wedge resection is favored for the management of PSP, while an additional pleural abrasion or chemical pleurodesis could be considered to potentially decrease the risk of recurrence after surgery. 7 However, surgery should also be selected strictly based on the risk factors and the patients' wishes to avoid overtreatment. 8
U-VATS may have advantages over a multiport procedure in terms of postoperative pain,9,10 but high-quality evidence is still lacking. The major concern of U-VATS is the collision of the instruments through a single port, necessitating a relatively long skin incision (at least >20 mm). To minimize the collisions between the surgical instruments within a shortened incision during bullectomy, an anchoring suture instead of a grasper for pulling of the bullae has been utilized, the previous reports of which are listed in Table 3. This procedure demonstrated some merits such as comfort of manipulation and cosmetic advantages. 12 Moreover, an anchoring suture for two-directional traction of the bullae is helpful to avoid the collisions between the instruments. U-VATS through a small (<20 mm) incision assisted with a bidirectional anchoring suture yielded acceptable outcomes. 13 Furthermore, the utilization of two anchoring sutures that facilitate the small incision U-VATS for the treatment of multiple or comprehensive bullae could be considered. 14
Previous reports of U-VATS pulmonary wedge resection using anchoring sutures.
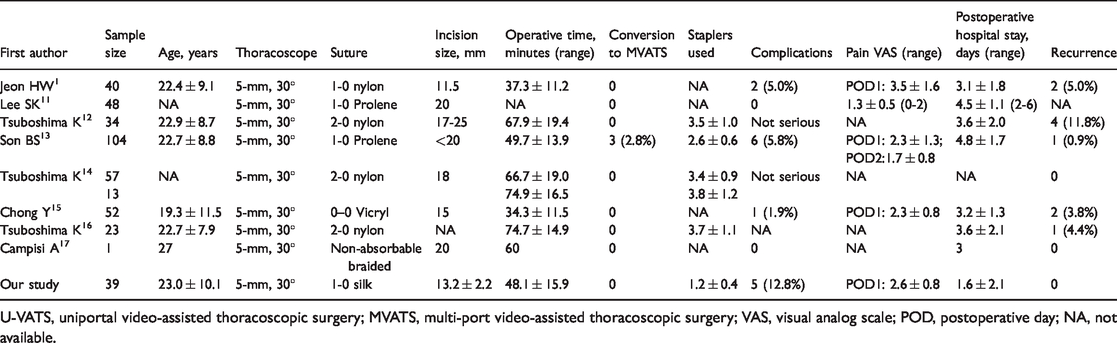
U-VATS, uniportal video-assisted thoracoscopic surgery; MVATS, multi-port video-assisted thoracoscopic surgery; VAS, visual analog scale; POD, postoperative day; NA, not available.
It is noteworthy that the incidence of 30-day unplanned readmission in PSP patients is reported to be 13.6%, and middle age and history of cancer are two independent risk factors for readmission. 18 Mechanical pleurodesis is widely used with the aim to decrease the risk of postoperative recurrence of PSP after bullectomy, while there is little evidence of this to date. A trial showed that the application of mechanical pleurodesis did not significantly decrease the incidence of PSP recurrence compared with simple wedge resection. 19 Hong et al. 20 reported that staple line coverage with a polyglycolic acid patch and fibrin glue, instead of pleural abrasion, may reduce the recurrence rate of PSP after bullectomy.
Furthermore, a retrospective review showed that appropriately identified patients could safely be discharged on POD 1 after lobectomy without an increase in 30-day unplanned readmission, morbidity, or mortality. 21 In our study, most patients in the anchoring group were discharged uneventfully on POD 1.
Conclusions
Next-day discharge after small incision (<20 mm) U-VATS bullectomy assisted with an anchoring suture is safe and feasible for selected patients. However, high-quality trials are warranted to verify our findings.
Research Data
Research Data for Next-day discharge following small uniportal thoracoscopic bullectomy assisted with an anchoring suture
Research Data, for Next-day discharge following small uniportal thoracoscopic bullectomy assisted with an anchoring suture by Chu Zhang, Miao Zhang, Haiyong Wang, Zhifeng Ma, Yuanlin Wu, Linhai Fu, Ting Zhu and Guangmao Yu in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by Zhejiang Medical and Health Research Fund Project (No. 2018KY171).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.