
Abstract
The goals of care (GOC) framework (2014) is an illness phase categorisation system that enables limitations of medical treatment (LOMT) to be documented and communicated within a healthcare system. It incorporates a clinical assessment of illness phase and GOC discussion on aims and LOMT for an episode of care. Together, this results in documentation of a GOC category that guides treatment escalation decisions during episodes of patient deterioration. Confusion exists about incorporating this framework into the perioperative period, particularly management of treatment escalation required for patient survival during surgery that is at variance with agreed goals and limitations. A historical tendency for automatic and unilateral suspension of limitations during surgery may be susceptible to ethical or medicolegal challenge. This article highlights the difference between the GOC framework and ‘not for resuscitation’ framework, considers the unique considerations of the perioperative period and addresses misconceptions of the GOC framework in patients undergoing surgery. Finally, it provides an approach to the GOC framework for patients considered for surgery by emphasising illness phase assessment and the need for the GOC category to accurately reflect the clinical situation throughout the perioperative period, guiding treatment escalation intraoperatively and postoperatively.
Keywords
Introduction
The growing acknowledgement that surgery is being performed in patients at the end of life culminated in a multi-college guideline in Australia and New Zealand, released in 2021 as a pilot document. 1 Recommendations include identifying patients at the end of life, shared decision-making and advance care planning (ACP), consideration of advance care directives (ACDs) and proactive goals of care (GOC) setting when planning surgery in this cohort. GOC are the aims of treatment, focusing on the patient’s current health condition, within an episode of care as agreed to between the patient, family, carers and healthcare team.2–5 The GOC framework is a clinical directive document to communicate aims and limitations of medical treatment (LOMT) based on an illness phase categorisation system. 6 In hospitals across Australia, it replaces the previous ‘not for resuscitation’ (NFR) framework.4,6,7 Although literature exists regarding shared decision-making,8–10 ACP11,12 and LOMT13–15 perioperatively, how to incorporate the GOC framework into the perioperative period has been only briefly addressed. 11 In this article, we present our approach to the GOC framework in the perioperative period through the utilisation of the information documented, particularly illness phase assessment, for patients presenting for surgery. This practical approach is based on our clinical and educational experience in anaesthesia and palliative medicine managing patients at the end of life who are offered surgery. Collectively, we have been involved in devising the GOC framework, 6 providing expert guidance regarding care for patients at the end of life considered for surgery 1 and contributing to university education in this area.
The GOC framework
Proactive GOC setting is a key recommendation from the guidelines for patients at the end of life considered for surgery. 1 GOC are the aims of treatment within an episode of care as agreed to between the patient, family, carers and healthcare team.2,5 GOC focus on the patient’s current health condition and change with transitions in illness phase.3–5 The GOC framework is an illness phase categorisation system that documents aims and LOMT, consistent with a patient’s condition and wishes, and communicates that within a healthcare setting. It was first reported in 2014, after preliminary experience in several Australian hospitals, and replaced the inadequate and binary NFR framework.2,6,7 The GOC framework encompasses a discussion on GOC and LOMT together with an illness phase assessment, resulting in a clinical directive document that records a ‘GOC category’. It has a dual purpose to both respect patient autonomy and avoid the use of non-beneficial treatment.
The GOC framework is a distinct document from an ACD, although clinicians can confuse them for each other.16,17 An ACD is a document expressing a person’s preferences and values, and has either common law or statutory force, so legal obligations vary by jurisdiction.18,19 In contrast, the GOC framework is a clinical directive document, completed by clinicians to record and reflect aims and LOMT during hospital admission consistent with a person’s wishes and condition. It may also form the basis of care planning after discharge or transfer to other care locations, including community care, depending on local policies. If a patient has an ACD, the GOC framework should accurately reflect the instructions or preferences within the ACD. 17 Similarly, GOC discussions focus on aims of treatment in the current episode whereas ACP discussions focus on future healthcare planning if decision-making capacity is lost.2,3,17 Setting GOC and completing the GOC framework is particularly important in emergency surgery, as ACP discussions are not possible if the patient lacks decision-making capacity.
To complete the GOC framework on hospital admission, clinicians first assess the patient’s diagnoses and prognoses to determine the illness phase as either curative (normal life expectancy), palliative (limited life expectancy) or terminal (imminent death). The illness phase is the vital clinical assessment in the GOC framework because GOC and LOMT are considered within this context (Table 1). A discussion then occurs regarding the aims of treatment, which establishes the direction of management during hospital admission. Discussions should occur with patients who have decision-making capacity and their families. Legally appointed substitute decision-makers (SDMs), guided by ACDs (if present), speak for the patient who has lost decision-making capacity.1,16,17 Finally, LOMT, which may be patient wishes to refuse treatment or clinician decisions to withhold non-beneficial treatment, are established. Timely and sensitive communication is key in all aspects of these discussions. The combination of illness phase, aims, and LOMT results in a ‘GOC category’ which is used to guide clinicians during episodes of patient deterioration (Table 2). The GOC framework differs from the previous NFR framework in two principal ways. First, clinical assessment on illness phase provides the context for aims and LOMT. Second, the NFR framework documented only a binary yes/no ‘NFR’ decision as to whether full cardiopulmonary resuscitation (CPR) would be undertaken for a future cardiac arrest. The GOC framework allows other LOMT that are consistent with the patient’s wishes and their medical condition to be documented. There are many other medical interventions (such as medical emergency team calls, intensive care unit (ICU) admission, dialysis, inotropes, etc.) that are inappropriate toward the end of life. This graded GOC approach can also be safely and effectively deployed during the perioperative period.
Misconceptions about the GOC framework in the perioperative period
As patients have their GOC framework completed at the beginning of hospital admission, they can present for surgery with a GOC category assigned. The presence of LOMT within a GOC category can cause confusion amongst anaesthetists and surgeons, who are unsure of how to manage LOMT perioperatively.13,20,21 Patients, including those in the palliative phase, may present with acute conditions that are potentially treatable with surgery; however, the GOC category and LOMT may seem to contradict such invasive treatment.11,22 The perioperative period is one of acute physiological disturbance routinely requiring advanced, invasive techniques that would be considered resuscitative outside this context.13,14,21 Distinguishing between patient or iatrogenic factors causing intraoperative deterioration may be difficult due to the reversible effects of anaesthesia and the rapid management of complications (e.g. bleeding).21,23,24 Death during surgery is considered a sentinel event and the burden of iatrogenic harm weighs on surgeons and anaesthetists.20,21,24,25 CPR is more successful during surgery contributing to the desire to proceed without LOMT.20,21,26,27 ICU admission to prevent or mitigate the iatrogenic burden of anaesthesia and surgery may be seen as justified to successfully reach the intended outcome of surgery. 25
Arising from these unique considerations, there are three intertwined misconceptions about the GOC framework in the perioperative period:
The GOC framework is irrelevant to the perioperative period and can be ignored. For surgery to be performed, the GOC category should be changed to one that has no LOMT. Patients assigned a GOC category with LOMT cannot be resuscitated perioperatively.
The first misconception is an after-effect from the previous NFR framework. It was believed that NFR orders related to ward management and were irrelevant to the perioperative period for the reasons above. Subsequently, the automatic and unilateral suspension of NFR orders was commonplace, until legislation and guidance from professional societies emphasised patient autonomy.13,28,29 In Australia, ignoring the GOC category and the LOMT documented may be subject to both ethical and medicolegal challenge, particularly as legislation across jurisdictions protects the patient’s right to refuse treatment, even critical and life-saving treatment.18,19
The second misconception reveals a backwards logic in the application of the GOC category. The clinician believes that to facilitate specific techniques (e.g. intubation and ventilation) required for safe surgery and anaesthesia, they must assign a GOC category with no LOMT. However, placing undue emphasis on LOMT to assign a GOC category may miscategorise the patient’s illness phase (e.g. from palliative to curative), potentially leading to inappropriate treatment escalation intraoperatively and postoperatively. 30
The final misconception ignores the need to ensure that a patient’s wishes and survival during surgery are transparently balanced. Survival is an important patient-centred outcome, even for those in the palliative phase. 8 Moreover, intraoperative resuscitation may achieve preferred patient-centred outcomes (such as a peaceful death postoperatively, surrounded by family), with subsequent enhanced family satisfaction in the bereavement phase if intraoperative complications arise. This final misconception may also lead to denying surgery to patients with LOMT, depriving them of potential benefit. 25
A practical approach to the GOC framework perioperatively
An understanding of illness phases provides the basis for management in the perioperative period using the GOC category as a guide (Figure 1). Before the offer of surgery, the GOC framework should be completed as outlined earlier. Illness phase (curative, palliative or terminal) assessment should consider both the surgical condition and the patient’s chronic comorbidities. Over 60% of patients who die in an acute hospital setting receive active interventions in the last 48 h of life, demonstrating the importance of distinguishing between the palliative and terminal phases.
31
This distinction is crucial as it is inappropriate to offer surgery to patients in the terminal phase when comfort, dignity and preparation for a peaceful death are the only priorities.1,5,6 Assignment of the GOC category, to communicate discussed GOC and LOMT consistent with the illness phase, completes the GOC framework. If surgery is considered, clinicians should ask:
Is the intent of surgery consistent with the illness phase and the aims of medical treatment in the GOC category? Do the LOMT in the GOC category interfere with my ability to facilitate surgery that is consistent with the illness phase?
Patients in the palliative phase should still be considered for surgery, particularly if the aim of surgery is for symptom relief or prevention.26,32 Curative intent surgery may also be appropriate dependent on the patient’s underlying life expectancy and the effect of an acute illness on this. For patients in the palliative phase, and high-risk patients in the curative phase, shared decision-making discussions will assist in determining preferred patient-centred outcomes and the realistic ability to meet these with surgery.1,11,12 Addressing the likelihood of recovery from both the burden of anaesthesia and surgery, and the appropriate escalation of postoperative treatment, including intensity and duration of ICU management, is also critical. 33 Collaboration of the perioperative decision-making team (including surgeons, anaesthetists, intensivists and perioperative physicians) in high-risk patients is warranted as these specialties have a skilled understanding of these issues.1,12,33,34 The GOC category can be used to guide discussions around demands for non-beneficial treatment and consensus should be reached prior to undertaking surgery. If conflict arises, reconsideration of surgery is appropriate with review of the intent of surgery, patient-centred outcomes, and clinician concerns. Seeking further expertise from another specialty team or a formal review process may assist with resolution.11,22 If the answer to the first question is no, then surgery should be reconsidered and other management options contemplated. The GOC category should not be changed as doing so may misclassify the illness phase.
If the answer to both questions is yes, then suspension or modification of the LOMT is considered whilst leaving the GOC category unchanged. Strategies to manage LOMT perioperatively are previously described for the older NFR framework;13,14,29,33,35 however, the GOC category provides valuable information to guide the anaesthetist to the best strategy. Determining the most appropriate management for LOMT will depend on the patient’s illness phase, intent of surgery, GOC, values and preferences, likely recovery from anaesthesia and surgery and extent of LOMT documented. Discussion should occur with patients who have decision-making capacity, and an SDM for patients who do not. If an ACD is present, clinicians should seek further advice about their medicolegal obligations as these change by jurisdiction.
For patients in the curative phase or when surgery is performed with curative or restorative intent, suspension (all LOMT are reversed) may be considered. If suspension is chosen, clinicians must clearly explain what treatment might be provided, the circumstances that may require this provision and the extent and intensity of treatment. This discussion provides the basis for patients to consider treatment refusal (e.g. chest compressions, mechanical ventilation after surgery) when suspension occurs instead of clinicians assuming buy-in and patients assuming that their wishes are known.25,36 A prospective decision on when LOMT will be re-instituted should also be made when selecting suspension. This may be based on location (once the patient leaves the post-anaesthesia care unit) or duration (if ICU admission is anticipated).1,14,29,34
For patients in the palliative phase or having surgery for symptom relief or prevention, modification of LOMT may be preferable. Modification may be techniques-based or values-based. Techniques-based modification allows for routine techniques that are required to administer safe anaesthesia and surgery (e.g. intubation, mechanical ventilation) but may prohibit resuscitative measures (e.g. chest compressions, defibrillation).1,14,29 As not all events in surgery can be predicted, the anaesthetist and surgeon may feel restricted by techniques-based modifications during intraoperative management, particularly if complications arise that are iatrogenic or unanticipated.20,24 However, techniques-based modification may be preferred by the patient, including those in the curative phase, if they have strong preferences about withholding specific treatment under all circumstances, for example, blood transfusions.
Values-based modification allows the perioperative team to use clinical judgement to achieve preferred patient-centred outcomes.1,29 Values-based modification requires an understanding of the patient as a person. It focuses discussions regarding resuscitation on patient outcomes instead of clinical risk, which may be more meaningful to patients.9,11 Patients in the curative phase may also consider this option, depending on their values and preferences. Although this is the authors’ preference regarding the management of limitations perioperatively, we acknowledge that it may be difficult to predict outcomes accurately during periods of sudden intraoperative deterioration. However, whilst resuscitative measures may commence in these periods of uncertainty, knowledge of the patient’s values and preferred outcomes can guide the length and intensity of intraoperative and postoperative management should unexpected or iatrogenic complications occur. Patient-centred outcomes to consider may be the potential reversibility of complications that would lead to an acceptable quality of life in the palliative phase, or the rapid transfer of patients from the operating room to ICU or the ward for family to be present if the patient progresses to the terminal phase.
In some cases, continuation of LOMT during surgery may be possible. Examples include a minor procedure under local anaesthesia or where LOMT do not interfere with routine perioperative management (e.g. limitation on chest compressions only).1,14 When continuation occurs, LOMT should be clarified to ensure a shared understanding of expectations during surgery. If a patient insists on continuation and the anaesthetist and surgeon believe that this would be unacceptably hazardous, it would be reasonable to reconsider surgery. 14
Regardless of strategy, the GOC category is not changed for the purpose of surgery, rather the LOMT within the GOC category is suspended or modified, to facilitate surgery that is consistent with the illness phase. This way the illness phase still accurately reflects the patient’s clinical situation and can be used to guide treatment escalation postoperatively. If the patient deteriorates postoperatively, and their illness phase changes (e.g. from palliative to terminal), the GOC category should be changed to reflect this. From there, aims and LOMT should be consistent with the new illness phase. The entire perioperative team should be informed of the patient’s GOC category and decisions regarding LOMT in the intraoperative and postoperative period.
Conclusion
Incorporating the GOC framework into the perioperative period is an important consideration for all anaesthetists, surgeons, intensivists and perioperative physicians. The GOC category provides the opportunity to understand the illness phase, ensure alignment between the aims of treatment and the intention of surgery, and guide the perioperative management of LOMT. The GOC category should be established before the consideration of surgery and an understanding of the illness phases of curative, palliative and terminal is vital. Intent of surgery offered should be consistent with the illness phase and aims of medical treatment of the GOC category assigned. Particular consideration should be given to the acute physiological disturbance that occurs during surgery and anaesthesia, potential to recover from episodes of intraoperative deterioration and the duration and intensity of postoperative support that would benefit the patient with respect to their wishes and illness phase. If surgery proceeds, LOMT applied by the GOC category should be managed within the perioperative context. LOMT options are suspension, modification, or continuation, with the final decision dependent on the illness phase, GOC, intent of surgery, decision-making capacity of the patient, availability of an SDM and/or the presence of instructions in an ACD. Communication of how LOMT will be managed perioperatively should be discussed with the patient, SDM and family as well as the perioperative clinical team.
GOC framework definitions and examples.
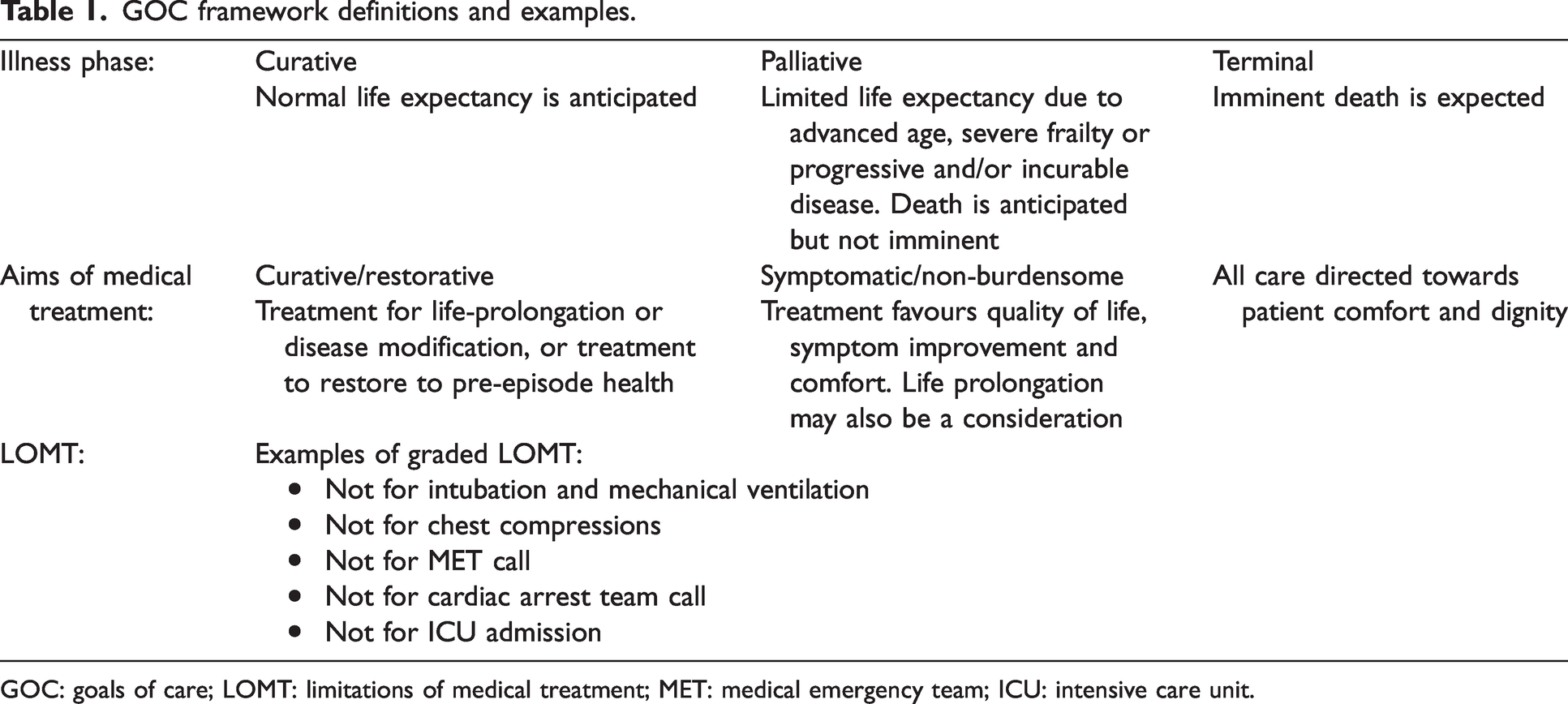
GOC: goals of care; LOMT: limitations of medical treatment; MET: medical emergency team; ICU: intensive care unit.
An example of GOC categories based on the GOC framework.
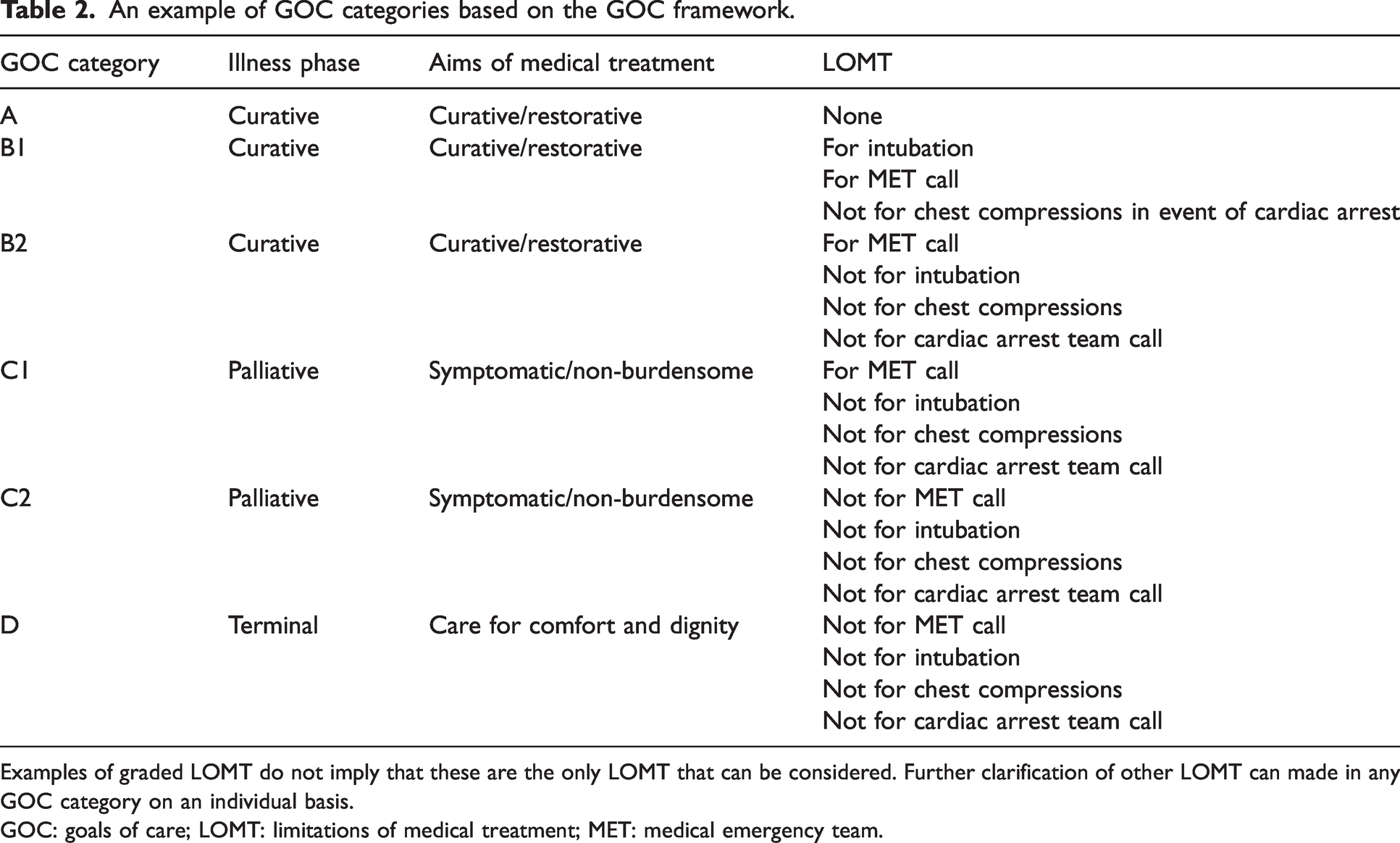
Examples of graded LOMT do not imply that these are the only LOMT that can be considered. Further clarification of other LOMT can made in any GOC category on an individual basis.
GOC: goals of care; LOMT: limitations of medical treatment; MET: medical emergency team.
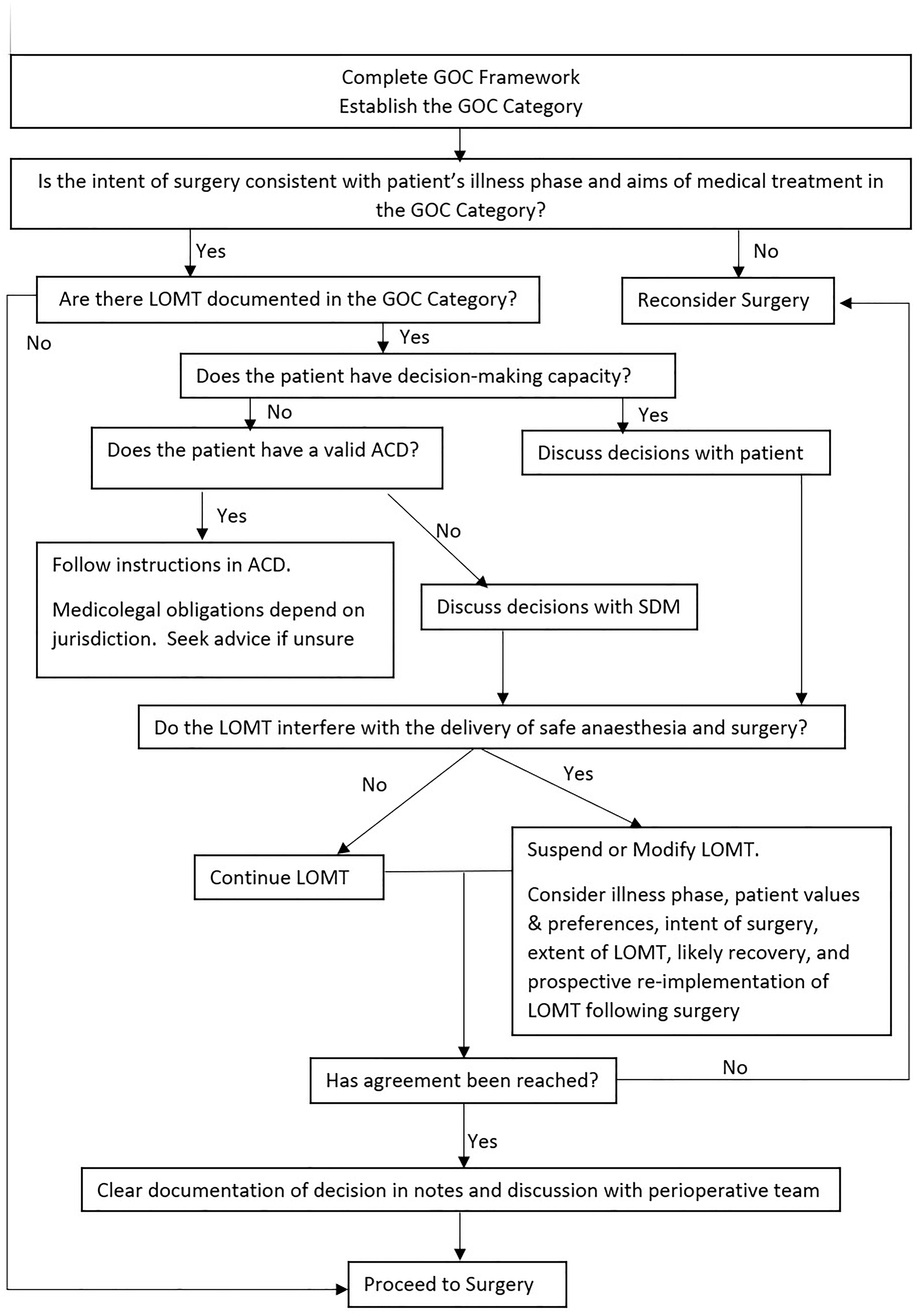
Decision-making flow chart to approach the GOC framework in the perioperative period.
Footnotes
Author Contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.