
Abstract
Published reports of uvular necrosis are uncommon and it is possibly an under-reported complication of oropharyngeal manipulation. Uvular necrosis is thought to develop due to ischaemia secondary to mechanical compression of the uvula from oropharyngeal devices. Patients typically present with symptoms of a sore throat within 48 hours postoperatively. It is unclear whether there are any preventable factors, or any specific management strategies that might reduce this complication. Treatment is most commonly conservative management, including observation and simple analgesia. We present 13 cases of uvular injury that were reported to a web-based anaesthesia incident reporting system (webAIRS), a voluntary de-identified anaesthesia incident reporting system in Australia and New Zealand. While the postoperative findings varied, sore throat was the most frequent symptom. Most of the cases resolved spontaneously; the remainder with supportive treatment only. The findings suggest that patients who sustain a uvular injury can be reassured, but they should be advised to seek review early if sore throat persists or any difficulty with breathing develops.
Keywords
Introduction
Iatrogenic uvular injury, which might be followed by uvular necrosis, is an uncommon complication that presents from one hour to two days postoperatively and typically resolves by two weeks. Patients will initially develop uvular ischaemia, which can appear as a swollen, erythematous uvula with a necrotic or sloughy tip, and they may describe symptoms of a sore throat or dysphagia. An extreme case of ischaemia during prolonged intubation of one month has resulted in soft palate necrosis. 1 Ischaemia is thought to be a result of mechanical compression of the blood supply of the uvula against the hard palate by an oropharyngeal device (e.g. endotracheal tubes (ETTs), laryngeal masks, upper gastrointestinal endoscopy, transoesophageal echocardiogram, aggressive oropharyngeal suction).2,3
A brief literature search (including PubMed, CINAHL Complete, Embase) found a total of 53 reported cases of uvular necrosis worldwide, with the first report published in 1978.3,4 Men represented three-quarters of all reported cases but there were no other associations reported with the type or length of procedure, or the type or size of oropharyngeal airway. 3 The largest study included ten patients, and reported an incidence of 0.034% over four years at a single tertiary centre. 5 It is unclear whether there are any specific preventable factors, or any specific management strategies that might reduce this complication. Treatment of uvular necrosis has most commonly been conservative (observation and analgesia), while some cases have been treated with steroids to reduce airway swelling or antibiotics to prevent secondary infection. 3 It has been suggested that prevention of uvular necrosis might be possible by placing any oropharyngeal devices away from the midline, avoiding blind suctioning and lowering the power of suction devices. 3
The objective of this case series was to determine if there were any identifiable risk factors from individuals who experienced postoperative uvular injury and to document the treatment they received.
Methods
WebAIRS (web-based anaesthesia incident reporting system) is a voluntary de-identified anaesthesia incident reporting system, which was introduced in Australia and New Zealand in September 2009. 6 The methodology of the system has been described in previous articles. 6 WebAIRS is owned, managed and funded by three organisations: the Australian and New Zealand College of Anaesthetists, the Australian Society of Anaesthetists and the New Zealand Society of Anaesthetists. Registered anaesthetists across Australia and New Zealand have been invited to report anaesthetic incidents by way of the webpage www.anztadc.net from 2009 onwards. Data describing the incidents can be entered by non-mandatory data input web controls, and in the form of text allowing the reporters to describe the incident and enter their reflections regarding contributing and alleviating factors.
An overview of the first 4000 incidents was published in 2017, in which the methods of the de-identified data collection were described. 6 Data were collected in compliance with the National Health and Medical Research Council 2014 recommendations for de-identified quality assurance data. 7 As de-identified data are no longer personal data, explicit patient consent is not required. In order to ensure that the project meets the requirements for de-identification, multicentre ethics approval is maintained at the Royal Brisbane and Women's Hospital human research ethics committee (HREC/11/QRBW/311) and the Nepean Blue Mountains local health district (HREC/12/NEPEAN/18). In New Zealand, ethics approval has been obtained from the health and disability ethics committee (MEC/09/17/EXP). These additional ethics approvals all agree that an exemption for the requirement for explicit patient consent is justified on the basis that the data specified reach an acceptable level of de-identification in the opinion of these ethics committees. All ethics committees suggested that the data collected for age and procedure duration be grouped rather than an actual age or procedure duration to reduce the chance of surrogate identification.
A narrative search using structure query language (SQL) was performed on the first 8000 reports to webAIRS to identify events that might have involved the uvula. The SQL search was designed to return reports that contained the words uvula, uvular, uvulas, uvulae, uvulitis, or similar matching words. These reports were reviewed by the authors and separated into those which matched the selection criteria (analysis group) and those that matched the search criteria but did not meet the selection criteria (excluded group). Data were extracted from the database for the analysis group, which included patient demographics, information about the surgical procedure (urgency, timing, specialty, procedure duration, and the type of surgical procedure), as well as information regarding the anaesthesia administered (anaesthetic technique, airway manipulation and airway device(s) selected).
Results
Twenty reports were identified by the SQL search.
Of the 20 case reports identified that involved the uvula, four cases were not related to trauma or swelling and were excluded. These four cases included operations on the uvula or an unrelated event at the level of the uvula (e.g. ETT kinked at level of the uvula). Of the remaining 16 cases, three cases reported uvular swelling, which may have resulted from anaphylaxis, angioneurotic oedema or oedema secondary to a neck haematoma, respectively. These three cases were excluded, leaving 13 cases of uvular injury to be analysed. In this group there were eight cases of observed uvular swelling, four cases with evidence of necrosis, three cases of uvular elongation, two of erythema and one case each of bleeding, enlargement, a split uvula and unspecified trauma. This gave 21 findings in the 13 reports.
A summary of the 13 cases is shown in Table 1, while a description of each case can be found below.
A summary of cases of uvular injury related to airway instrumentation, from the WebAIRS database.
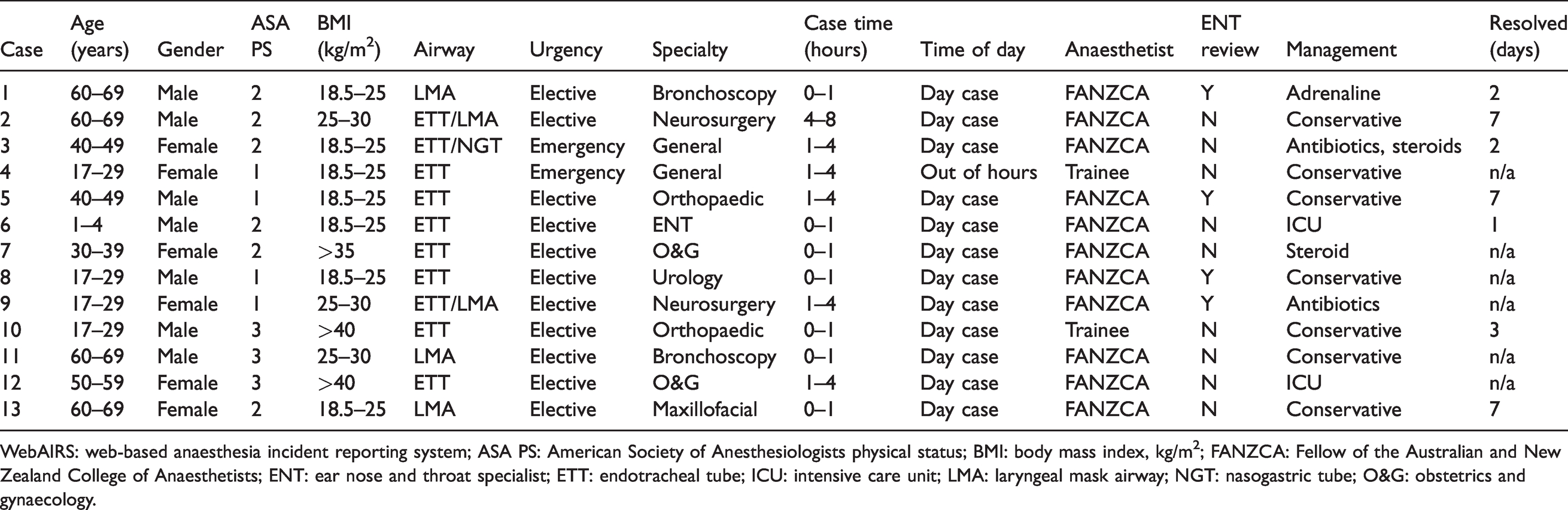
WebAIRS: web-based anaesthesia incident reporting system; ASA PS: American Society of Anesthesiologists physical status; BMI: body mass index, kg/m2; FANZCA: Fellow of the Australian and New Zealand College of Anaesthetists; ENT: ear nose and throat specialist; ETT: endotracheal tube; ICU: intensive care unit; LMA: laryngeal mask airway; NGT: nasogastric tube; O&G: obstetrics and gynaecology.
Case 1
An American Society of Anesthesiologists physical status (ASA PS) 2 man in the 60–69-year-old age group underwent an elective bronchoscopy with ultrasound biopsy. The patient had a size 4 laryngeal mask airway (LMA) that was easily inserted but was changed three times during the 35-minute procedure. The patient developed severe laryngospasm requiring boluses of propofol and endobronchial salbutamol. In the post-anaesthetic care unit (PACU), there was a small amount of blood noted on the LMA once it was expelled. The patient then developed severe stridor requiring nebulised adrenaline (epinephrine) and nebulised lidocaine with humidification. The patient was reviewed by the ear, nose and throat (ENT) team who confirmed a severely swollen uvula with elongation down to the epiglottis. He was admitted overnight for further humidified air and made a good recovery.
Case 2
An ASA PS 2 overweight man in the 60–69-year-old age group underwent an elective craniotomy for a meningioma. The patient had been intubated with an ETT for the more than four-hour case and an LMA exchange was attempted three times to facilitate a smooth wake-up. Ventilation with the LMA failed and the patient was bag–mask ventilated until awake. On the first day postoperatively, the patient complained of a sore throat and was found to have a swollen elongated uvula at the level of the base of the tongue. The patient was reassured, and the swelling resolved by one week postoperatively.
Case 3
An ASA PS 2 woman in the 40–49-year-old age group underwent an emergency laparotomy for bowel obstruction. The patient had a grade 1 Cormack–Lehane (C+L) view with a nasogastric tube in situ, which was placed by the surgical team. Intubation was uneventful with a size 7 mm internal diameter ETT for the operation. The patient had a sore throat for the following two days and was found to have an erythematous, white uvula with an area of necrosis. The patient was reviewed by the ENT team who commenced the patient on intravenous antibiotics and dexamethasone. The pain resolved over the next two days with some shortening of the uvula.
Case 4
An ASA PS 1 woman in the 17–29-year-old age group underwent an emergency laparoscopic appendicectomy. The patient was intubated with an ETT for the operation. After the procedure, the patient was noted to have some uvular bruising.
Case 5
An ASA PS 1 man in the 40–49-year-old age group underwent an elective Achilles tendon repair. The patient had an atraumatic intubation with a reinforced ETT taped in the midline before rolling the patient prone and placing the ETT to the right for the procedure. In the PACU, the patient had a sore throat. Four days postoperatively, the patient had an erythematous elongated uvula with a white necrotic tip that was sitting on the posterior tongue causing persistent cough. The ENT team confirmed uvular necrosis and provided reassurance. Symptoms resolved around day 7.
Case 6
An ASA PS 2 male child in the 1–4-year-old age group with a history of obstructive sleep apnoea and asthma underwent an elective adenotonsillectomy. The patient had an uneventful intubation with an ETT and was extubated deep at the end of the operation. Immediately he developed laryngospasm and intermittent airway obstruction persisting for 45 minutes. A decision was made to reintubate, insert a nasogastric tube to decompress the stomach and return to theatre to examine the airway for any foreign bodies. Examination of the airway found a swollen and enlarged uvula. The patient was extubated in the operating theatre and admitted to the intensive care unit (ICU) for observation without any further issues.
Case 7
An ASA PS 2 morbidly obese woman in the 30–39-year-old age group underwent an elective bilateral salpingectomy. The patient had a Mallampati 3 pharyngeal view and grade 2B (C+L) laryngeal view and had an atraumatic intubation with an ETT for the procedure. In the PACU, the patient had a sore throat that was treated with paracetamol, ibuprofen, lidocaine spray and dexamethasone. She re-presented to the emergency department the next day with a sore throat and difficulty swallowing, and was found to have a traumatic injury to the posterior pharynx. A swollen, elongated uvula was visible hitting the tongue. She was discharged with simple analgesia, dexamethasone and further lidocaine spray.
Case 8
An ASA PS 1 male child in the 1–4-year-old age group underwent an elective left radical orchidectomy. The patient had a failed first intubation by a medical student before an uneventful intubation with a grade 1 (C+L) view with an ETT for the one-hour procedure. Antibiotics and dexamethasone were given intraoperatively. In the PACU, the patient had a sore throat and was found to have an erythematous and swollen uvula. The patient was discharged home the same day and was reviewed the following day by the ENT team, who confirmed uvular ulceration with minimal necrosis.
Case 9
An ASA PS 1 woman in the 17–29-year-old age group with no significant comorbidities underwent an elective single level lumbar microdiscectomy. The patient had a grade 1 (C+L) laryngeal view and had an atraumatic intubation for the operation. At the end of the case, the airway was suctioned under vision and the patient was extubated deep for an LMA exchange. Two days postoperatively, the patient’s primary care provider contacted the anaesthetic consultant requesting further advice. The patient presented to the emergency department with a sore throat and painful swallowing. She was reviewed by an outpatient ENT team who found a black necrotic uvular tip confirming uvular necrosis. She was discharged home with oral antibiotics on the same day.
Case 10
An ASA PS 3 man in the 17–29-year-old age group with a history of osteogenesis imperfecta and body mass index (BMI) greater than 40 kg/m2 underwent an elective removal of metal ware from the distal radius. The patient appeared to have aspirated on induction and underwent a modified rapid sequence induction but was found to have no evidence of aspiration on suctioning the airway. The patient failed initial extubation due to inadequate reversal, then rapidly desaturated and was suctioned further due to extensive oral secretions. After he was completely reversed with sugammadex, he was safely extubated and was found to have a sore throat and a swollen, split uvula in the PACU. On phone review a few days later, he was pain-free and declined a formal review.
Case 11
An ASA PS 3 man in the 60–69-year-old age group underwent an elective bronchoscopy. It was noted that there was a significant amount of movement by the bronchoscope in and out of the dual lumen LMA that was placed. Postoperatively the patient was found to have a sore throat and a necrotic uvular tip.
Case 12
An ASA PS 3 woman in the 50–59-year-old age group with a history of morbid obesity and sleep apnoea underwent an elective laparoscopic hysterectomy. The patient received both spinal and general anaesthesia, and was then ventilated in a steep head-down position. She was successfully extubated in the lateral position. In the PACU, the patient developed airway obstruction which non-invasive ventilation failed to overcome; a rapid sequence induction was performed, and the uvula was noted to be oedematous at intubation. She was transferred to the ICU and successfully extubated the following morning.
Case 13
An ASA PS 2 woman in the 60–69-year-old age group underwent an elective removal of teeth with routine intravenous induction and atraumatic placement of a flexible LMA. A throat pack was then inserted with Magill’s forceps and there were no intraoperative issues with the airway. The surgery was uneventful, lasting less than one hour. At the end of the case the surgeon removed the throat pack and suctioned the pharynx. No further suctioning was required. The LMA was gently removed once the patient emerged from anaesthesia and opened her mouth voluntarily. In the PACU, the patient complained of sore throat but was discharged home with no other issues. During a phone conversation three days postoperatively, the patient described significant throat pain, inability to swallow, change in voice and constant irritation in the back of the throat. The patient described ‘bruising’ and ‘swelling’ to her uvula consistent with likely uvular ischaemia or necrosis. The patient did not present to her primary care provider or to hospital; therefore, there was no opportunity for a medical practitioner to examine the patient or confirm the diagnosis. Over the course of one week, her symptoms gradually settled, with mild voice change and throat irritation persisting.
Summary of cases
There were almost equal numbers of ASA PS 1, 2 or 3 patients. There were no ASA PS 4 or 5 patients. The age groups of up to 30 years, 30 to under 60 years, and over 60 years were similar in number and there were almost equal numbers of boys and men (n=7) and women (n=6). The majority of cases (54%) had a normal BMI, approximately a quarter were overweight (BMI 25–20 kg/m2) and approximately a quarter had a BMI greater than 30 kg/m2.
All the patients received general anaesthesia. The devices used in the airway included an ETT in ten cases (77%) and an LMA in five cases (38%). Other devices included a nasogastric tube in one case, ENT instruments in one case and a bronchoscope in three cases. However, in one of these cases the bronchoscope was used for a fibreoptic intubation and diagnosis, and did not cause the uvular swelling which was pre-existing. There were two emergency cases (15%) and one out-of-hours case (8%). The duration of procedures was almost evenly split between less than one hour and greater than one hour. No cases were greater than four hours. Most of the cases were performed in the operating theatre and seven cases (54%) became evident in the PACU. Two cases were performed at remote locations.
Most cases (92%) were managed by a specialist anaesthetist and a wide variety of surgical specialties were involved.
Four (31%) cases were reviewed by the ENT team. Treatment ranged from observation to medical management and admission to the ICU. Eleven cases (85%) were assessed as having a temporary disability by the reporter. The remaining four cases were stated as ‘not be affected by the incident’.
Discussion
Uvular necrosis appears to be an uncommon complication of airway management during anaesthesia, but as it presents only as a sore throat the condition might be under-reported. To our knowledge, our case series represents the largest reported to date. Although uvular necrosis is an uncommon cause of postoperative sore throat, clinicians should be suspicious if patients are reporting symptoms of a sore throat and difficulty swallowing liquids or solids. A necrotic uvula characteristically has a sloughy white tip, which may have areas of black necrotic tissue. Around the uvula and soft palate there may be some petechial haemorrhages from trauma (Figure 1). A sore throat after a procedure is very common and a more sinister cause may not initially be investigated by the surgical team (approximately 10% with LMA, approximately 40% with ETT). 8 After discharge, individuals who continue to experience a sore throat and difficulty swallowing are more likely to be followed up by their primary care provider or re-present to the emergency department for review. In both these cases, the treating anaesthetist involved in the case may not be notified of the adverse event.
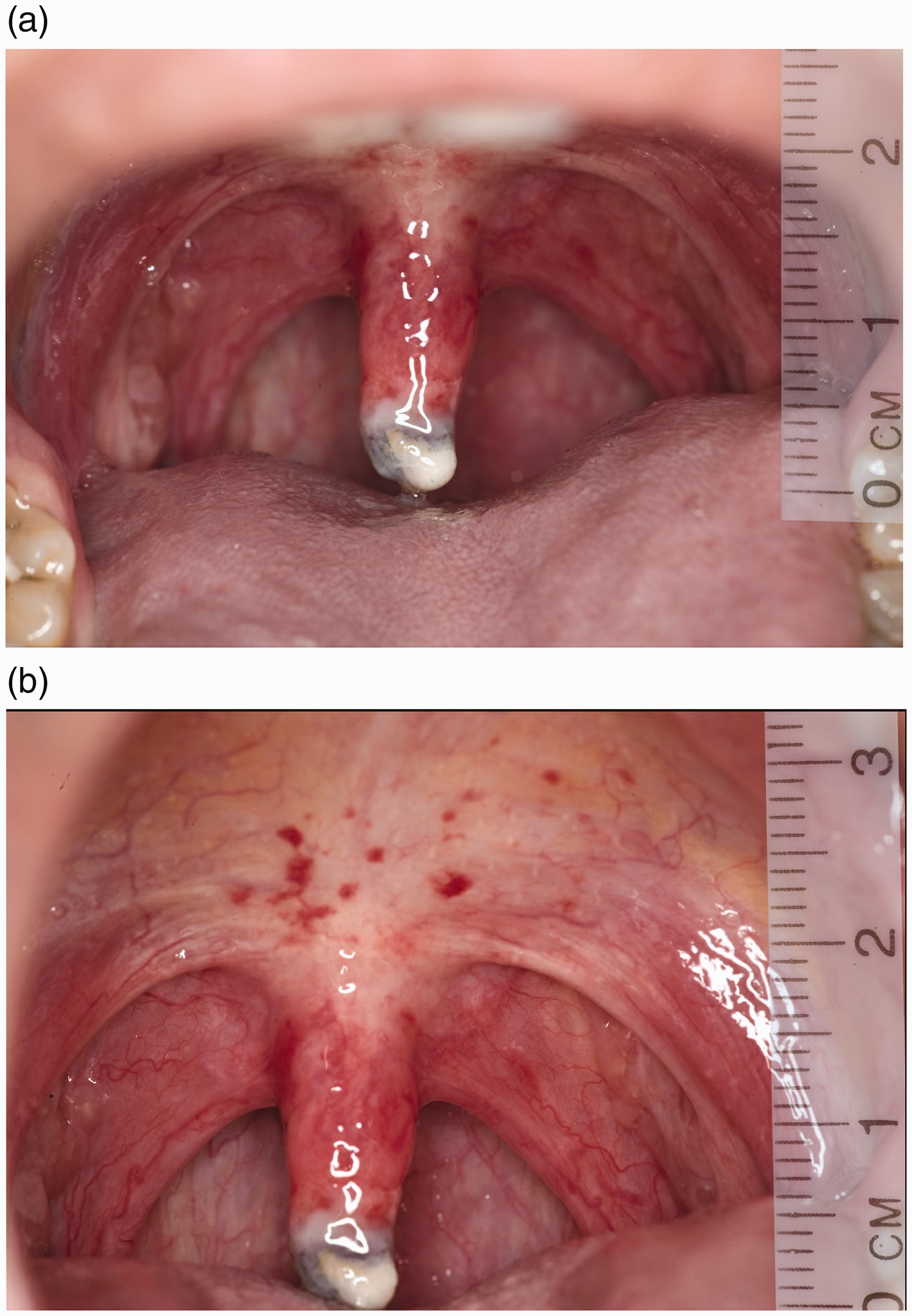
Necrotic uvula with a typical sloughy white tip can be seen in (a) and (b) while the petechial haemorrhages on the soft palate are visible in (b).
Reporting to webAIRS is voluntary and so numerators and denominators cannot be determined. Furthermore, with so few cases of uvular necrosis the positive predictive value for any hazards identified would be exceptionally small, and we did not identify any predictive factors in this case series. It is also possible that there are other factors that may contribute to uvular damage that have not yet been reported. The information is limited by the information entered by the treating anaesthetist, the potential for reporter bias, and the relatively small number of case reports. Furthermore, there was no long-term follow-up of patients included in this case series and therefore we cannot comment on the long-term mortality or morbidity associated with uvular necrosis.
There were no severe adverse outcomes or prolonged morbidity found in the literature search or found by this case series. The majority of cases of uvular injury or uvular necrosis were managed conservatively with simple analgesia and resolved in less than two weeks. Patients can therefore be reassured that any injury will likely improve without intervention. However, if symptoms were to persist or progress, such as increasing pain, developing fevers or infective symptoms, inability to talk or tolerate an oral diet or if there was any other concern, patients should present to their primary care provider. In the presence of any airway compromise, patients should present to the emergency department.
In view of the relatively benign outcomes that are seen in the 13 cases in this series as well as the majority of the reported cases in the literature, a reasonable approach in the management of these cases would be firstly to examine the patient to exclude a more serious injury to the palate or surrounding structures. In cases in which there might be doubt a referral to an ENT specialist for a second opinion would be prudent. If the injury is minor based on these clinical assessments, a conservative approach including simple treatment of the symptoms such as analgesia and mouth washes might be all that is required. The patient should be advised to request and attend a follow-up consultation if symptoms do not resolve or become progressively worse. In the literature review, which involved 53 cases, three cases with similar symptoms required surgical excision and one excision by the patient. In the setting of prolonged intubation, there is a risk of soft palate necrosis, that was seen in two patients who were intubated for one month, requiring surgery.
Conclusion
While it is not possible to determine incidence from voluntary reporting, it can be established that uvular injury due to airway instrumentation is an uncommon cause of an incident report to webAIRS. Nevertheless, the incidents reported should raise awareness of anaesthetists of the potential for uvular injury and that care should be taken with airway instrumentation. While the postoperative findings may vary, sore throat was the most frequent symptom. Most of the cases resolved spontaneously with no intervention required. Overall, the findings suggest that patients who sustain a uvular injury can be reassured, but they should be advised to seek review early if sore throat persists or any difficulty with breathing develops.
Footnotes
Acknowledgements
The author(s) would like to acknowledge the contribution of all members of ANZTADC (Australian and New Zealand Tripartite Anaesthetic Data Committee), past and present and the large number of anaesthetists reporting incidents to WebAIRS in the interests of greater patient safety.
The author(s) also thank N Barker, University of Queensland Librarian, Brisbane, Australia, for her valuable assistance with the systematic search.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.