
Abstract
Papua New Guinea is a Pacific country that remains an enigma to the world at large. Despite massive geographical challenges due to mountainous terrain, remote islands, poverty, and with 80% of the population of over eight million living in rural villages, Papua New Guinea has managed to develop national medical and postgraduate specialty training. The first recorded anaesthetic was administered in Papua New Guinea in 1880 and the first anaesthetist trained in 1968. The University of Papua New Guinea graduated its first diploma in anaesthesia candidate in 1986 and its first master of medicine candidate in anaesthesiology in 1991. As of December 2021, there have been 82 diplomas and 40 masters of medicine awarded. We review the factors and influences bearing on the development of physician anaesthesia training in Papua New Guinea over this period. Many of the people involved have contributed information used in this article.
Keywords
The health system of any low and middle-income country is that country’s greatest asset in caring for the wellbeing of its people. The Lancet Commission on Global Surgery (LCoGS) in 2015 stated that: Surgical and anaesthesia care should be an integral component of a national health system in countries at all levels of development.
1
In 2010 an estimated 32.9% (16.9 million) of all deaths worldwide were from conditions needing surgical care and this exceeded the combined deaths from HIV/AIDS, tuberculosis and malaria.2,3 The medical workforce need applies particularly to surgeons, anaesthesiologists and obstetricians, and the critical numbers of these particular medical specialists have a direct correlation with survival from surgical and obstetric conditions. 4 The LCoGS recommends 20 surgeons, anaesthesiologists and obstetricians per 100,000 population with current recommendations being a minimum of four physician anaesthesia providers (PAPs) per 100,000. However, it takes many years to train these specialists and there is much competition in a low resource country for trainees in different specialties, especially with low medical school graduation numbers. Anaesthesia in developing countries has been identified as a significant risk for patients due to few PAPs, paucity of training for non-physician anaesthesia providers (NPAPs), very limited patient monitoring, and poor supplies of appropriate disposables and drugs for anaesthesia. 5
Papua New Guinea (PNG) is due north of Australia and is the eastern half of New Guinea, the second largest island in the world. It is one of the countries with the least number of trained physician anaesthesiologists in contrast to high-income country neighbours such as Australia and New Zealand who have 75 times the PAPs. 6 PNG has 0.25 PAPs per 100,000 which is on par with Zambia, Sudan and Benin. 7 PNG has 22 provinces with 80% of the population living in remote villages throughout the mountainous highlands or on the many remote smaller islands. It is estimated that PNG will need over 500 physician anaesthesiologists trained by 2030 to reach the LCoGS and other goals. 7 At current rates of physician anaesthesiology training this is unattainable. This paper maps the factors and influences bearing on the development of physician anaesthesia training in PNG.
Early days of colonisation
Before the First World War, the northern half of what is now PNG was German New Guinea and the southern half was British New Guinea. This southern part, known as Papua from 1905, was transferred to Australia as a trusteeship in 1906. There may be undiscovered early reports of anaesthesia in government, missionary and trading histories of that era in English and German. In 1863 German physicians had experience with ether, chloroform and nitrous oxide to provide surgical anaesthesia in Germany,
8
and this extended to their colonial territory in German New Guinea: When hospitals were built they were simple in construction and lacked equipment for complicated surgery, although operations under full anaesthetic were not unknown.
9
Australia took control of the eastern side of the island after the First World War under two different administrations—Papua and New Guinea. These were united as a territory in 1946, and PNG achieved independence in 1975.
The earliest report so far of an anaesthetic in PNG is in 1880, and was the manual removal of a retained placenta from the wife of a missionary. 10 The first recorded anaesthetic administered to a national (indigenous) patient is referenced in a German book that records the administration of chloroform by Dr Wilhelm Wendland to several Bogadjim villagers for the removal of arrows, 2 weeks after a tribal fight in 1896. 11 Lady (Dr) Phyllis Cilento in her book My Life records in 1923 administering anaesthesia for her husband in Rabaul, consisting of ‘alcohol, chloroform and ether, to get them asleep and then converting to ether’. 12 Anaesthetics when administered were delivered by expatriate doctors or locally trained ‘native medical practitioners’ who were under the guidance of the surgeon.
During the Second World War, there were major theatres of war in New Guinea involving Australian, American and Japanese forces. Anaesthesia and surgery were provided extensively by these military forces but will not be addressed in this paper.
Non-physician anaesthesia providers
In the Pacific Island nations, PNG and Timor-Leste, there are twice as many NPAPs as there are PAPs. In PNG, 80–90% of anaesthesia is provided by NPAPs, known as anaesthetic scientific officers (ASOs), who undertake a one-year diploma of anaesthetic sciences course at the University of Papua New Guinea.7,13 This task-sharing or task-shifting is essential for normal surgical services in remote provincial hospitals in PNG while a pool of physician anaesthetists is developed which may take decades or could never be achieved.14,15
Expatriate physician anaesthetists
In 1966, the territory of PNG had a population of over 2 million people which included 20,000 Australians and 6000 Asians. Of 217 hospitals in the Territory, 102 are controlled by the administration and 115 by missions. Of 6249 medical personnel, 4778 are indigenous. There are 147 European doctors and 438 non-indigenous nurses, and one trained anaesthetist.
16
The first specialist anaesthetist appointed in PNG was in 1961. It is reported as having been an ‘Egyptian doctor named Noah’ but nothing else is recorded. The second specialist anaesthetist appointed in PNG was Dr John Foley in 1963. 11
Dr (David) John Foley DA, FANZCA (1932–2021) was born in the United Kingdom, educated at Clifton College and studied medicine at the University of Bristol, graduating in 1955. He worked at Nuneaton and successfully passed his diploma of anaesthesia (DA) in 1960. Foley subsequently worked at Geelong Hospital, Victoria, Australia, as the medical superintendent before going to PNG from 1963 to November 1971.
11
After leaving PNG he worked in Adelaide as an anaesthetist. He was elected to fellowship of the Australian and New Zealand College of Anaesthetists (ANZCA) in October 1996 in recognition of his contributions to anaesthesia and medicine. In 1967 I had some study leave in England. Whilst there I attended a seminar in Cambridge on anaesthesia in developing countries. A doctor from East Africa spoke of his program for training anaesthetic nurses, using an EMO machine. Upon my return I was able to start such a programme working with what were then called Medical Assistants. The first course was with two such students for a year. Subsequently they went out into smaller hospitals to work on their own, or under general supervision of the surgeon. On a visit to Goroka in December 1984 I was pleased to see one of those first two students anaesthetise for a Ramstedt’s Procedure. Although assured that there were no fire risks with ether, relaxants and air, I did not use the EMO for head and neck surgery. I also spent a week in Liverpool with the paediatric anaesthetic unit there. They gave me a pulse monitor – it had a throat microphone to pick up pulses in the fingertip, and a very simple circuit. I also bought an East–Freeman ventilator. This was invaluable in relieving me from manual ventilation over lengthy “Commando operations” – excision and pedicle grafts for mouth and tongue cancers which occur following the use of betel nut – usually at least one a week, lasting 8–11 hours. I spent a month in Anguganak in the Sepik as a locum for Dr John Sturt, working with the Brethren mission there. While there a hospital orderly’s wife went into labour with a hand presentation. I gave a spinal anaesthetic and did the caesarean section (the only time I have ever done the procedure) the baby survived only to die nine months later of malaria. This always seemed to me a prime example of the need for public health measures to run with, or even ahead of, curative medicine. It was a very busy time in Port Moresby running anaesthetics for a 400-bed hospital, with limited assistance. Besides this I taught the medical students some pharmacology, was involved in setting up a medical society with its journal and was responsible for the intensive care unit. In late 1968 I took a year off from anaesthetics to take up an administrative post in the Department of Public Health, as Assistant Director (Medical Services) which meant that I had responsibility for the Government hospital services. This gave me an opportunity to travel widely visiting some of the many hospitals – especially in the smaller centres. I felt that my major contribution had been the development of an anaesthetic Assistants Course, and the development of an Intensive Care Unit where we could concentrate serious cases. It was therefore with some dismay that I read criticism of both of these in Eileen (Ellen) Kettle’s History of Nursing in Papua New Guinea – criticisms which were contrary to the facts in both matters. (John Foley, unpublished autobiography. Sent to TEL by John Foley, May 2020)
Dr Foley wrote a plea in 1967 for the modernisation of anaesthetic practice in Papua and New Guinea with specialist anaesthetists and also nurse anaesthetists (or NPAPs) to provide services in more remote areas. 17 He also contributed the chapter on preanaesthesia preparation to the book Medical Officer’s Pocket Book published in 1966 by the Department of Public Health, Territory of Papua and New Guinea. 18 In this chapter of four pages he talks about the importance of preoperative assessment and optimisation, the need for fasting, management of respiratory complications and hypotension as well as premedication and the issues of postoperative care and when it is safe to discharge from the recovery ward. He suggested a chest X-ray for all patients and not proceeding with a haemoglobin level less than 10 g/dL. 18
Dr Roma Varoneckas (1937–2012) was born in Lithuania and moved to Adelaide as a child. She graduated from the University of Adelaide and worked in Mt Hagen from 1963 to 1965 and then Port Moresby, giving anaesthesia from 1967 until she left PNG in 1977. She was registered as a specialist having done 5 years supervision under Foley. Roma had to anaesthetise Foley for his appendicectomy, with Foley later returning the favour and anaesthetising Varoneckas for the delivery of one of her children. 11
John Foley left in 1971 and was replaced in 1972 by Dr Ronald Rae (1928–2018) from Tasmania. Ron had done his medical training at the University of Melbourne, completing his studies in 1961 at the Alfred Hospital (Dr John Paull, personal correspondence with TEL, December 2020). Rae was recruited to replace John Foley by the Australian government-administered Public Health Department of the territory of PNG. Ron had gained his Australian anaesthetic fellowship (of the Faculty of Anaesthetists of the Royal Australasian College of Surgeons (FARACS)) in 1971 and took up the post in Port Moresby just after he finished training. It is believed that he left when PNG achieved independence in 1975. He returned to Tasmania and worked at the Mersey Hospital. Initially, the Port Moresby position had been offered to Dr John Board but he chose to remain in Lae as a result of having established a strong working relationship at the Australian and New Guinea Administrative Unit Hospital.
Dr (Alan) John Board trained in anaesthesia at St George Hospital, Kogarah, Sydney. As a senior registrar in 1970 he met Dr John Foley at a conference in Canberra and was invited to work in PNG. He travelled to Lae where he spent 2 months as a trial with his family, and they returned in January 1971 for several years, working in Lae and Goroka. John developed strong ties in Lae and declined when offered the opportunity to take up the post in Port Moresby after John Foley departed in 1971. Board returned several times to PNG on Australian government-supported trips and acted as external examiner in 1991 for Dr Noel Yaubihi’s successful masters of medicine (anaesthesiology) exams. Dr Board went on to become director of anaesthesia at the Royal Children’s Hospital, Brisbane, and pioneered the introduction of anaesthesia for paediatric liver transplantation in Australia. We were employed by the PHD (Public Health Dept) of TPNG (Territory of Papua and New Guinea) but it was all paid for by the Australian Government. There were two levels of pay, the local pay rate and the expatriate rate. I was moved to TPNG by the Dept of Territories and then employed by PHD at the expatriate rate. At the time of Self Government, from memory Jan 1974, the expatriates were offered the choice of staying with PHD at the local pay rate or becoming employees of the Australian Government at the expatriate pay rate. I chose, as did most expats to change to the Australian Government at the expat pay rate. Nothing changed as far as the work, just a different source of pay, like secondment. Ron Rae was not in PNG prior to being recruited to replace John Foley. I was involved in training the ATOs and trained a few. When I arrived they were already giving unsupervised anaesthetics. (John Board, personal correspondence with TEL, 30 September 2020)
In the pre-independence era, there were some specialised surgical aid missions from Australia. In 1960 Dr Brian Dwyer (director at St Vincent’s Hospital, Sydney) and surgeon Dr Harry Windsor (who performed the first heart transplant in Australia) went to PNG for 4 weeks with a team undertaking thoracic surgery for advanced tuberculosis which was widespread. 19 Dr Wendy Reid worked at Port Moresby in the 1960s and taught anaesthesia. From 1972 to 1974 Dr Rae Howard, an Australian doctor, worked with her husband Dr Ian Riley at the remote Tari Hospital in the Southern Highlands. She gave anaesthetics using an EMO inhaler, there was no ventilator and an extremely limited oxygen supply. 20 She later joined the University of Papua New Guinea (UPNG), Port Moresby in 1982 and became a lecturer in pharmacology and anaesthesia while her husband was the professor of community health with the university until 1986 (Ian Riley, personal correspondence with PBW, 2020). Dr Laurie Doolan worked as an anaesthetist with the 2nd Battalion Pacific Islands Regiment in Wewak and Port Moresby in the early 1970 s (Laurie Doolan, personal communication with TEL, November 2019).
At this time anaesthesia was often performed in many provincial hospitals by other specialities, one author (MC) witnessed an Australian paediatrician being responsible for anaesthesia at Mendi Hospital in 1981—this included anaesthesia for a thoracotomy for an arrow in the heart—which the patient survived. Other major mission hospitals have provided surgical and anaesthetic services for many years, and these include St Mary’s Hospital, Vunapope, Rabaul, and Kudjip Hospital in the Western Highlands.
Medical anaesthetic training phase one
Prior to 1951 all doctors in Papua and New Guinea were expatriates, working for the Australian government, industry (mining or copra) or missionaries. However, there was a significant potential for Papuan and New Guinean medical staff after the war. 21 In 1947 while the country was governed by Australia under a United Nations international trusteeship, it was decided to send some national men to Fiji to train as ‘local doktas’ at the Central Medical School, Suva. This was a 5-year course after which candidates returned to New Guinea for deployment as ‘doktas’. Sixteen of 60 who commenced completed their training. The first being Dr Wilfred Moi who commenced in 1947 and graduated in 1951. 22 Dr Moi had previously completed the orderly training programme on Gemo Island, Port Moresby. 23 This programme continued until 1963. The programme was ceased once the Papuan Medical College opened in 1960. 22 It appears that nationals already in training in Fiji completed their course there. 11 Dr Himson Mulas undertook and completed this programme from 1953 to 1958. Returning to PNG he completed residency years and then undertook anaesthetic training with Dr John Foley at Taurama Hospital, later known as Port Moresby General Hospital (PMGH). Dr Mulas was sent to the Alfred Hospital in Melbourne, Australia, in 1966 to 1967, where he undertook further anaesthetic training. On his return to PNG, he continued his career in anaesthesia but shortly after moved into administration in Rabaul and Lae. He is recognised as the first PNG national doctor acknowledged as a specialist anaesthetist. 24
Medical anaesthetic training phase two
The Papuan Medical College based at Taurama, Port Moresby, commenced in 1960 graduating its first class of three in 1964, with 44 people graduating in total up until closure in 1970. These were the first medical students trained in PNG. Two were of particular importance:
Dr Christiaan (Chris) Marjen (1939–2014) (Figure 1) was born in Opiaref village in the Dutch East Indies (now Indonesia). He was in the first group of students attending the Papuan Medical College, beginning in 1962 and graduating in 1969. 22 Chris undertook residency posts in Port Moresby until 1973 when he travelled to Australia. He began his anaesthetic training in Sydney at Royal Prince Alfred Hospital but was called back to PNG in 1975 at independence. He subsequently was able to become naturalised as a PNG citizen and completed his training at the Anaesthesiology Center Western Pacific in Manila, Philippines in 1976. He was appointed as the senior medical specialist anaesthetist to PMGH in 1977. 11 Chris Marjen was the inaugural president of the Society of Anaesthetists of Papua New Guinea (SAPNG), a position he held from 1986 to 2001. After 10 years in private practice, he returned to PMGH in 1991 and went on to become chief executive officer of the hospital from 1996 until 2003. He retired in 2008. Marjen received a member of the order of the British Empire (MBE) in 1995 and the order of Logohu (PNG) in 2009 for services to medicine in PNG, as well as life membership of the PNG Medical Society. 11
Dr Chris Marjen (1939–2014). Photo courtesy of UPNG Press and bookshop. 38
Dr Ume Arua (died 2002) was another anaesthetist at that time who came from Bereina, Central Province. He also graduated in 1969 from the Papuan Medical College and subsequently trained in anaesthesia in Manila gaining the DA. 22 Dr John Hains, former president of the Australian Society of Anaesthetists recalls him undertaking some training in Brisbane in the early 1970s, and presenting Arua with a Goldman vaporiser (John Hains, personal correspondence with TEL, July 2020). Arua was based at Goroka Hospital and was working there when Dr Gajinder Oberoi arrived in 1987. Dr Gertrude Marun and Dr Magea Pole (personal correspondence with TEL, July 2020) confirm Dr Arua working in Goroka for many years, and subsequently transferring to Port Moresby in the early 1990 s where he worked as an anaesthetist mainly in the obstetric unit until his death while on-call. It is believed that Arua commenced the master of medicine training but did not complete it (personal recollection, HA). 11
Medical anaesthetic training phase three
Opening in 1966, UPNG began a medical course with the first graduates obtaining their degrees in 1972. The Papuan Medical College was the forerunner to the current School of Medicine and Health Sciences (SMHS), UPNG. 22 There are now approximately 50 graduates per annum. A second medical school opened in Madang at the Divine Word University in 2016 and has graduated their first doctors at the end of 2020. All current national doctors with anaesthetic qualifications undertook their medical training from UPNG.
Early development of physician anaesthetic training programme in PNG
The master of medicine (MMed) in surgery commenced in 1974, with their first candidates at UPNG graduating in 1978. 25 UPNG also accepted anaesthesiology training from 1974. However, it failed to attract candidates for various reasons including perceived lack of prestige, income and the length of course being 4 years. This was the situation for the initial 11 years with no applicant being attracted. Several people were subsequently instrumental in mentoring and attracting candidates to the MMed in anaesthesiology course.
Dr Pankaj Patel was recruited to Madang as an anaesthetist in 1980. Her husband Prof Niv Patil was appointed as a surgeon. She had trained in medicine in India and completed her fellowship in anaesthesia in Britain. In addition to her clinical work, she introduced anaesthetic training to the health extension officers curriculum and wrote a handbook on anaesthetic practice for health extension officers. After these accomplishments she was recruited by the Department of Health to introduce anaesthetic training to PMGH/UPNG in 1985 on the retirement of Dr Semesa Serevatu. Dr Serevatu was a Fijian anaesthetist who had been awarded a fellowship of FARACS in 1972. He held the post as chief anaesthetist at PMGH from 1980 to 1985 when he retired due to ill health arising from the complications of diabetes. He returned to Fiji and worked there as one of the few anaesthetists after the 1987 coup despite a leg amputation. He passed away in 1994.
Dr Patel was able to attract a candidate to the training programme by offering a one-year DA prior to entering the masters’ 3-year programme. In personal correspondence she says that the programme was based on an Indian programme with which she was familiar, and it was seen as more attractive than committing to 4 years. The DA commenced in 1986 with the training of Dr Gary Ou’u under her supervision. 26 There were four more diplomates: Billy Selve, Tekie Purewa, Yet Akalana and Noel Yaubihi before the first MMed graduate was attracted. Dr Patel recalled that the examiners for the first DA were Dr James O’Callaghan from Brisbane, herself and Dr Gajinder Oberoi.
Recollections of Pankaj Patel: Dr. Serevatu, senior specialist, retired in 1985, at the same time a couple of other specialists also left PNG, leaving a considerable gap at Port Moresby Hospital and the Faculty of Medicine. The Secretary of Health at that time, Quentin Reilly, requested that I take over as a Senior Specialist and organise training programme at all levels in anaesthesia with an aim to gradually localise, as per department of health’s plan, and provide continuity for service commitments as well as training. The first job in Port Moresby Hospital was to lay down proper protocols for the theatres and anaesthetic department in safe practice. Having organised this aspect, the most important task was to plan for future manpower and match the training needs in anaesthesia for Papua New Guinea. Next question was how to attract medical graduates to the speciality. This was easier said than done! The residents who did their two months’ residency were targeted with a limited success. Lack of specialists around the country had been a stumbling block to successful training in the past and if this was not remedied it would be the same vicious circle. The Secretary of Health was very supportive in the recruitment drive for specialist from overseas, so all base hospitals and larger provincial hospitals would have one specialist who would be responsible for training in that hospital. To attract medical graduates to anaesthesia an intermediate training with an award of Diploma was proposed by Dr Isaac and Dr Patel and approved by the UPNG in 1986. The one-year course started to attract interest amongst the medical graduates. Most of them felt that even if they decided not to pursue a further carrier in anaesthesia, they would benefit from the additional qualification if they chose to work in a smaller hospital as part-time anaesthetists. This plan was encouraged and supported by the Department of Health, which would allow additional anaesthetic support for hospitals like Arawa, Mendi etc. where only one ATO (Anaesthetic Technical Officer, precursor to the current Anaesthetic Scientific Officer) provided service. The first anaesthetic trainees for the Diploma course were enrolled in 1987. (The) Australian Aid Development Bureau (AIDB) was very helpful in providing sponsorship for lecturers and external examiners from Australia. Initially anaesthetists who had previously worked in PNG were invited as visiting lecturers, later Dr Tess Cramond from Brisbane was very helpful in recommending external examiners for the Diploma and MMed Anaesthesia. Once the medical officers had successfully completed the Diploma, they were offered the option of enrolling for the Masters course for further three years, one of which would be spent in the Highlands, mainly in Goroka. Dr Noel Yaubihi was the first UPNG graduate to complete his Masters and be registered as a specialist. (Pankaj Patel, personal correspondence with TEL, 2019)
While Patel was in Port Moresby, Dr Mike Tronson from Melbourne acted as external examiner in 1990 along with Dr Prakash Kulkarni, an Indian graduate who was working in Lae and who went on to work in the USA, and retired as professor of anesthesiology at Jefferson Medical College in Philadelphia. Dr Geoff Gordon of Townsville acted as visiting lecturer around this time also. Dr Patel left PNG in 1991 and her role of trainee supervisor was taken over by Dr Sivapalan Varatharajan who departed in 1993. He was subsequently replaced by Dr Gajinder Oberoi who had been working in Goroka and arranging teaching of doctors and NPAPs. Dr Oberoi completed his contract and left Port Moresby in December 1994 (Dr Varatharajan, personal correspondence with TEL, August 2020).
Since then, the role of trainee supervisor has been held by PNG graduates, with Dr Noel Yaubihi 1994 to 1998, Dr Gertrude Marun (formerly Didei) 1998 to 2005, Dr Harry Aigeeleng 2006 to 2013 and currently Dr Pauline Wake 2014 to the present.
Dr Varatharajan, or Dr Vara, as he is universally known, is a Sri Lankan anaesthetist who was born in Ceylon in 1936. He graduated MB BS in Ceylon in 1961 and completed primary fellowship of FARACS training in Ceylon and the second part fellowship of FARACS in London in 1967, returning to Ceylon in 1970. After working around the country in government hospitals he decided to move on to PNG, arriving in September 1987 and stayed in Port Moresby for 5 years. After this he worked in Brunei for 16 years until retiring in 2009 (coinciding with the end of hostilities against Tamils, and returning to Sri Lanka). During his time in Port Moresby, he worked initially alongside Dr Pankaj Patel as head of department of teaching and training local doctors in anaesthesia. There were specialist anaesthetists in Goroka (Dr Oberoi and Dr Mohan), and Dr Kulkarni in Lae. Varatharajan recalls that: … most of the Specialists were expatriates along with the local surgeon.
In addition to training doctors for the newly running diploma and MMed in anaesthesia courses he also remembers teaching: … medical students (three weeks) and interns (six weeks). During this period, one was able to train the local doctors to administer anaesthesia at the peripheral hospitals. I was very fond of regional blocks, particularly brachial plexus and ankle blocks. Ketamine was a readily available intravenous anaesthetic agent. Nurse Anaesthetists (ATOs) did an excellent job within their powers. The ATOs were trained well and successfully completed their exams satisfactorily. Both Dr. Patel and I continuously upgraded their knowledge by visiting the peripheral hospitals from time to time. The ATO training centre was in the Highlands. Whenever I visited the local hospitals, I talked to them on resuscitation, particularly. (Dr Varatharajan, personal correspondence with TEL, October 2020)
Dr Usha Mohan, wife of Dr Mohan, recalls this of her husband while working in Madang: Dr Mohan worked as the anaesthesiologist in Madang General Hospital from 1986 up until mid 1992. He had two assistants who were qualified Health Extension Officers – I forget their names. One of them left after a year or two and the other one stayed on until we left in 1992. Dr Mohan trained the Health Extension Officers from the Allied School of Sciences. We were employed by the Ministry of Health. He knew Dr Patel and was in regular touch with her. (Usha Mohan, personal correspondence with PBW, 2021)
Gajinder Oberoi was born in Lucknow, India in 1953. He completed his schooling and medical training in Punjab and his anaesthetic specialist training in New Delhi at the All India Institute of Medical Sciences. Oberoi arrived in Goroka in April 1987 and worked there as senior specialist anaesthetist until October 1993. During his time in Goroka, the training of ATOs continued as a priority. His memory was of training four each year. In this time, he also came into contact with and mentored the first PNG national to complete the diploma and master of medicine exam in anaesthesiology: Dr Noel Yaubihi. In 1993 Dr Oberoi was transferred to PMGH as a senior staff anaesthetist after the departure of Dr Sivapalan Varatharajan, with Dr Noel Yaubihi as director. Gajinder left Goroka in October 1993 and completed his contract at PMGH in December 1994. During his time in Port Moresby, he was supervisor of training for DA and MMed candidates. He then moved to Adelaide, Australia where he completed fellowships in anaesthesia and in pain medicine before moving to Royal Hobart Hospital, Tasmania (personal correspondence to TEL, July 2020). Dr Oberoi co-authored an important textbook with Professor Garry Phillips—Anaesthesia and Emergency Situations 27 —and other important books for anaesthetists who also did intensive care when possible, including Care of the Critically Ill Patient in the Tropics by David Watters (professor of surgery, UPNG 1992–2000). 28
Current DA and MMed anaesthesiology programme, UPNG
The DA was first awarded in 1987 and the first MMed graduation was in 1991 with the programme continuing at present. Candidates must first complete the diploma which is one year, and if the candidate achieves a mark over 60% in that exam they are able to apply for the MMed programme. MMed takes 3 years with written exams after year one and a written exam, viva exam and successful presentation of a thesis to complete the third year. Case reports and assignments are required as part of the course. Training for the DA can be undertaken in any hospital in the country where there is an MMed qualified anaesthetist to supervise. Examinations at the end of the year are always undertaken at the UPNG in Port Moresby. MMed candidates can complete some years outside of PMGH, but all candidates are strongly advised to complete at least the third year and usually the last 2 years in Port Moresby because of exposure to intensive care, visiting specialist surgical teams and a greater range of anaesthetic practice.
To date there have only been two university-appointed senior lecturers who have conducted the DA and MMed courses.
The first was Dr Harry Aigeeleng (Figure 2) who was initially seconded to the School of Medicine and Health Sciences (SMHS) at UPNG from the Department of Health and then was permanently appointed in 2003. He continued to coordinate training until stepping down in 2013. Since then, the post has been held by Dr Pauline Wake (Figure 2), a Milne Bay doctor born on remote Woodlark Island. She has been assisted by the appointments of Dr Elizabeth Inaido-Lee in 2015, Dr Nancy Kwara in 2017 and Dr Michelle Masta in 2020–2021. These people are responsible for overseeing exams, required course work throughout the year and arranging syllabus and end-of-year exams. They have a major role in trainee welfare and personal development as well as medical student teaching.

Dr Harry Aigeeleng (left) and Dr Pauline Wake, October 2021 in Port Moresby at the University of PNG exams. Photo courtesy of Dr Michelle Masta.
The first four candidates to undertake the diploma did not proceed to MMed, but Dr Noel Yaubihi (Figure 3) after completing his DA, entered MMed training and successfully completed this in 1991.
Dr Noel Yaubihi who retired in 2021. Photo courtesy of Dr Lucas Samof.
A review of trainees shows their outcomes (Table 1). Part of the explanation of the discrepancy between those undertaking DA and MMed is that, at the time, trainees in emergency medicine (EM) had the opportunity to complete a diploma in another specialty and many chose anaesthesia. Sixteen EM candidates have successfully attained the DA with several others withdrawing before exams. All this occurred when interest in anaesthesia training as a specialty among doctors was low, and it had the benefit of increasing the skill set of EM doctors. There has been no intake of EM candidates for the DA since 2016 when EM training was restructured and EM trainees spend 3-month supervised attachments in both the operating theatres and intensive care unit (ICU) with objectives set from their own disciplines.
Outcomes of DA/MMed programmes at UPNG until December 2021.
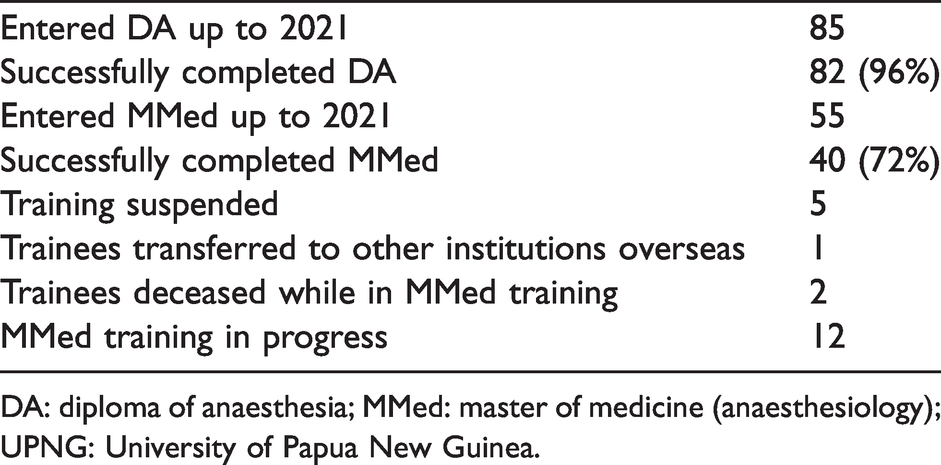
DA: diploma of anaesthesia; MMed: master of medicine (anaesthesiology); UPNG: University of Papua New Guinea.
As one of the two anaesthesia training facilities in the Pacific Island nations, with the other being Fiji, PNG provides the opportunity for doctors from other countries to undertake postgraduate training in anaesthesia. Training of anaesthetists in UPNG provides valuable resources for the rest of the Pacific Island nations. Table 2 shows their countries of origin.
Non-PNG Pacific countries of origin for DA and MMed training at UPNG (n = 10).
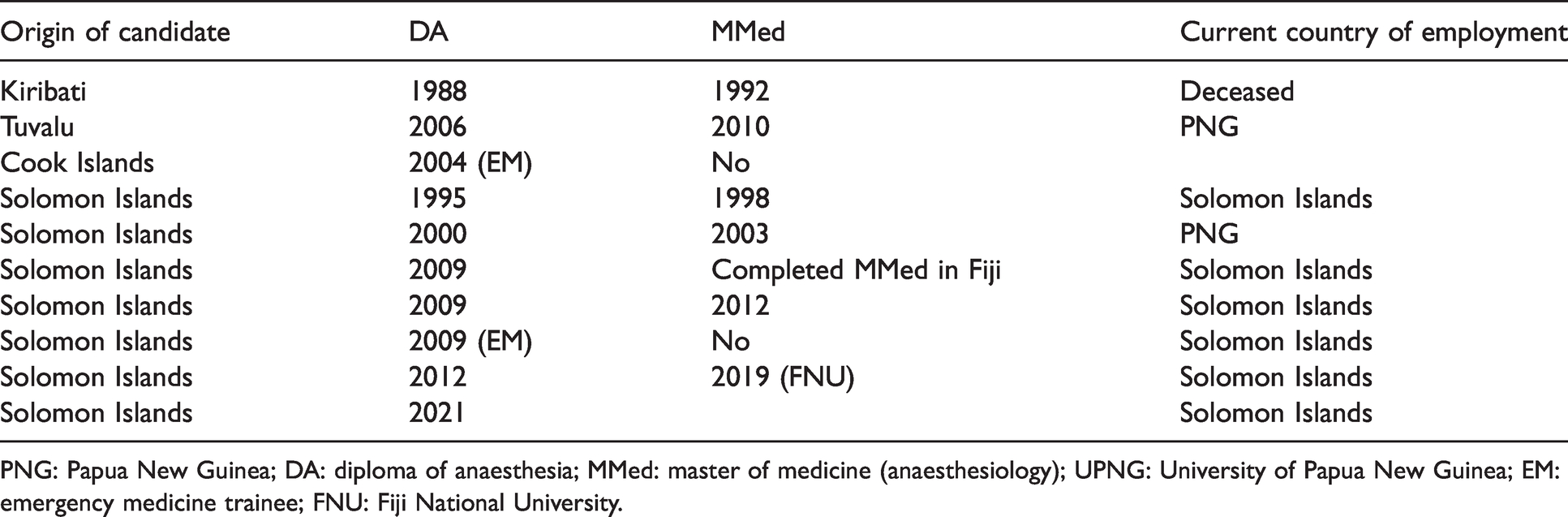
PNG: Papua New Guinea; DA: diploma of anaesthesia; MMed: master of medicine (anaesthesiology); UPNG: University of Papua New Guinea; EM: emergency medicine trainee; FNU: Fiji National University.
External examiners were originally arranged informally by the PNG teaching supervisor on the advice of Professor Tess Cramond (nee Brophy) from Brisbane, an ex-dean of the Australian faculty. The examiner at the first DA exam was Dr Jim O’Callaghan from Queensland who examined for several years. Dr Mike Tronson from Melbourne was the examiner in 1990 and Dr John Board examined in 1991. Professor Doug Jones and Dr Kester Brown examined from 1992 to 1994. Professor Garry Phillips examined from 1995 and Dr Wayne Morriss from New Zealand from 2002 until 2007. In 2008 no exams were held and from 2009 to 2021 Dr Terry Loughnan was external examiner. These trips were funded through AusAid and ANZCA support. Since 2016 the anaesthetic examiners in UPNG have also included an ICU specialist which in 2016 and 2017 was Dr George Skowronski and from 2018 to 2021 was Dr Mark Nicholls. In both DA and MMed exams an external examiner is mandated by UPNG. This is now arranged and supported by ANZCA and UPNG.
Currently there are MMed anaesthetists in Port Moresby, Rabaul, Lae, Madang, Mendi, Wewak and Alotau but not in any of the other 16 provincial government hospitals in PNG which are supplied by NPAPs. This does not include mission or mining hospitals.
The first three anaesthetists who were trained prior to the UPNG course commencing all received placements and training in Australia: Dr Mulas in Melbourne, Dr Marjen in Sydney and Dr Arua in Brisbane. These attachments have continued until the present with many of the anaesthetists in PNG training internationally (Table 3).
Overseas training positions of Papua New Guinean anaesthesiologists and scholarship source (where applicable).
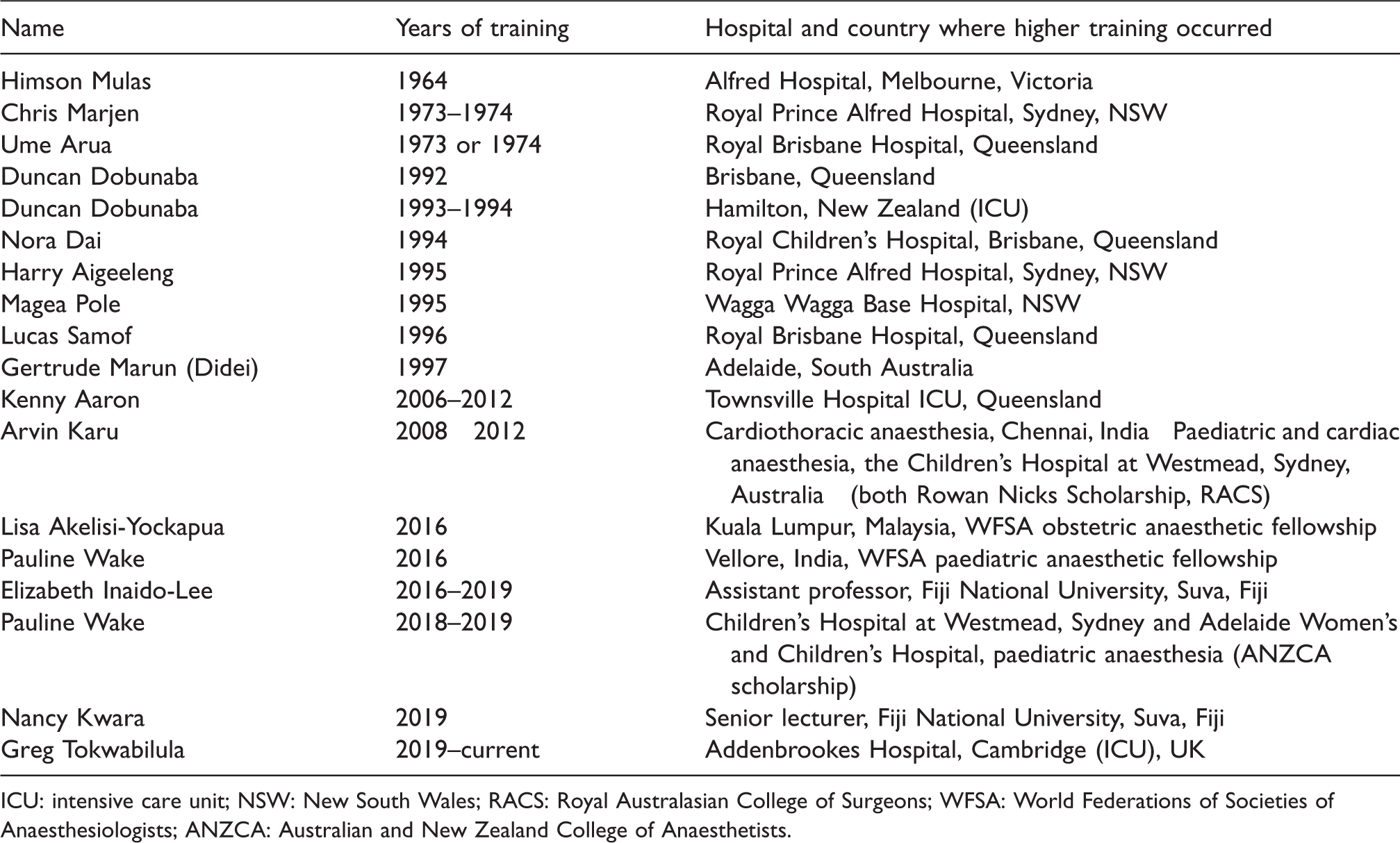
ICU: intensive care unit; NSW: New South Wales; RACS: Royal Australasian College of Surgeons; WFSA: World Federations of Societies of Anaesthesiologists; ANZCA: Australian and New Zealand College of Anaesthetists.
Table 4 lists all the graduates in master of medicine (anaesthesiology) from UPNG since 1991.
Master of medicine (anaesthesiology) graduands from the University of Papua New Guinea (n = 40).
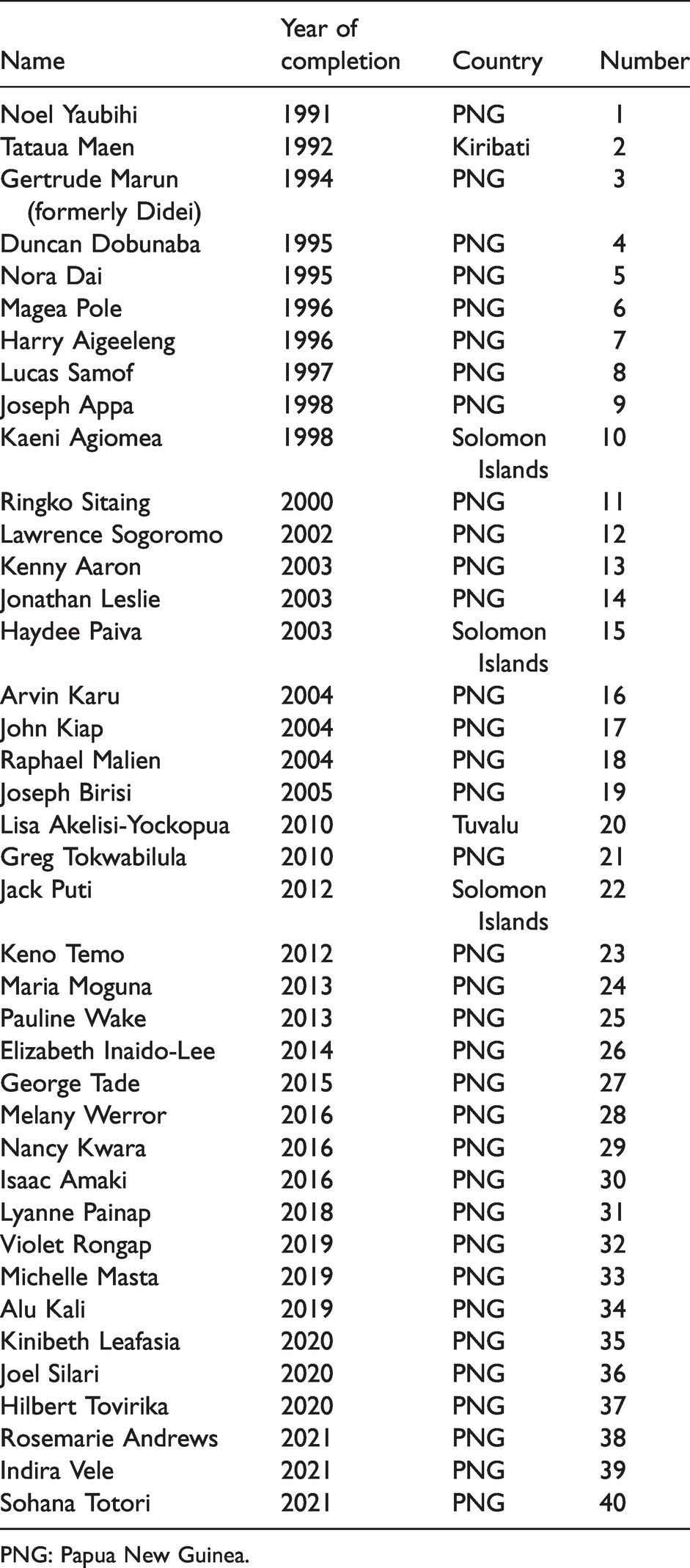
PNG: Papua New Guinea.
Over many years local anaesthetists have been involved in the running of an ICU at Port Moresby and Lae. A separate part of the MMed exam is a short answer paper on ICU topics and the short case vivas include an ICU patient. Drs Dobunaba, Aaron and Tokwabilula have undertaken additional ICU training overseas and are currently involved in running the unit at PMGH while Dr Marun is involved in Lae. Anaesthetic trainees rotate through the ICU.
PNG is one of the few countries in the world where there exists a mechanism at UPNG for higher postgraduate diplomas (HPGDs) in medical subspecialties. This takes 2 years. Currently the only HGPD attained is in cardiac anaesthesia, held by Dr Arvin Karu. Now there are two candidates in paediatric anaesthesia and one in obstetrics and gynaecology anaesthesia, with planning underway for head and neck/airway anaesthesia and pain medicine HPGDs. The College of Intensive Care Medicine in Australia has also supported submission for a HPGD in intensive care medicine with three trainees enrolled.
There has been a very high retention rate of MMed anaesthesiology graduates in PNG, which is reflective of all the specialist workforce in PNG. 29 In recent years, anaesthesia in PNG has been supported by anaesthetists with visiting surgical teams who have provided one to one clinical and other teaching. Most of these missions have been funded by AusAid, the Royal Australasian College of Surgeons and the Australian Department of Foreign Aid and Trade. There has also been support from Rotary, Doctors Assisting in South-Pacific Islands, Open Heart International, Australian Volunteers International and Médecins Sans Frontières. There have been other educational visits as well.
Anaesthetists involved include Chris Acott, Matthew Crawford, Michael Cooper, David Daly, Fergus Davidson, Yasmin Endlich, Roger Goucke, Susan Hale, Andrew Jeffries, Roni Kreiser, Elaine Lee, Janet Loughran, John Keneally, David Kinchington, Michele O’Brien, David Pescod, Alan Rubinstein, Michael Shun, Neil Street, Stephen Swallow, Sally Wharton, Darren Wolfers and many others.
Deserving of mention is Dr Oliver Adams, a German anaesthetist who worked for Médecins Sans Frontieres in Tari in the highlands from 2012 to 2013 and then in Kundiawa from 2014 to 2020, after which he returned to Germany. During this time he assisted in training anaesthetic registrars as well as ASOs. He coordinated a safer anaesthesia from education (SAFE) obstetric course, an essential pain management (EPM) course, one shared primary trauma course, several advanced cardiac life support courses and one difficult airway workshop in Kundiawa. Also, Dr Zhang was a Chinese anaesthetist who first went to PNG in 1995 and worked in Rabaul. He later returned as a contract medical officer who worked in Lae where he trained ASOs and then moved to Port Moresby where he continued to train ASOs as well as in-theatre teaching of registrars.
Outside of Australian support, there have also been teams of doctors, including anaesthetists from China working at PMGH in the last two decades 11 and more recently as part of the ‘belt and road’ initiative. Other doctors have been supplied by the Cuban government. PNG sits on the Pacific ‘ring of fire’ and has major volcanic natural disasters involving surgical responses from local medical services and international medical teams.30,31
Involvement of ANZCA
Despite the DA and MMed programmes being established initially on an Indian model, with which Dr Pankaj Patel was familiar, there has been long-standing close relations between ANZCA (and its predecessor—the Faculty of Anaesthetists, Royal Australasian College of Surgeons) and the anaesthetic training system in PNG.
Professor Garry Phillips (1936–2016) from Adelaide, attended the first early management of severe trauma course held in PNG as an instructor in 1993. At the invitation of Dr Gajinder Oberoi, whom he met on that visit, he undertook three visits per year, each of one to 2 weeks’ duration teaching trainees and examining from 1993 to 2004.
As a result of Professor Garry Phillips’ involvement with PNG, a programme commenced that was supported by Dr Vic Callanan at Townsville Hospital in Queensland, where PNG registrars, usually in the last year of their MMed training, could spend 12 months. This extended from 1996 to 2006. For participants in that project see Table 5.
PNG anaesthetic registrars rotated from PNG to Townsville Hospital, Queensland.
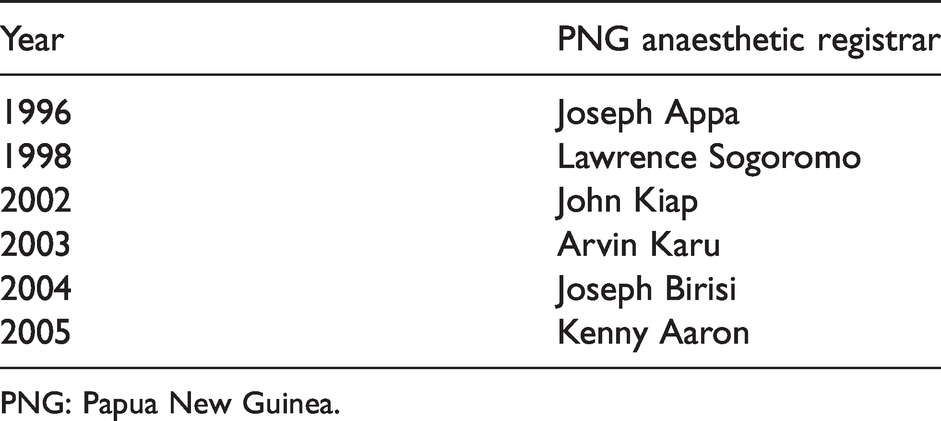
PNG: Papua New Guinea.
Garry Phillips was president of ANZCA from 1996 to 1998 and was appointed professor to UPNG in 1998. Professor Phillips had a unique attachment to PNG having served for 2 years in 1956 and 1957, as a kiap or cadet patrol officer in remote parts of the country before commencing his medical studies. Phillips and Dr Harry Aigeeleng played major roles in the further development of the training programme for anaesthetic trainees as well as the establishment of a diploma course for NPAPs, who until 2003 received on-the-job training only.
In 2000 Phillips wrote to Dr Mathias Sapuri, dean of the faculty of medicine at UPNG, pointing out that the number of MMed graduates in surgery, otorhinolaryngology, ophthalmology and obstetrics/gynaecology far outstripped the number of graduates in anaesthesiology with obvious consequences for the training of all specialties. This was raised with the Health Minister and Health Secretary at the time.
From 2006 until 2009 there were no MMed anaesthetists graduating, reflecting the low position of anaesthesia as a specialty in PNG. In 2007, a group was formed within ANZCA to support anaesthesia education in PNG, and in 2008 two educational visits were funded. This support group consisted of Professor Garry Phillips, Drs Harry Aigeeleng, Wayne Morriss, Richard Morris and Michael Cooper. In May 2010, the ANZCA overseas aid committee was formed with Drs Wayne Morriss (chair), Michael Cooper, Roger Goucke, Roni Krieser, Professor Kate Leslie, Drs Rob McDougall and David Pescod. The support of anaesthesia in PNG is one of the committee’s core activities. Dr Michael Cooper became chair in 2012 and the committee was renamed the global development committee in 2020. Dr Yasmin Endlich became chair in 2022.
After Phillips’ retirement this role was taken on by Dr Michael Cooper from Sydney who was appointed as adjunct professor of anaesthesiology to UPNG in 2014. This role is currently one of mentoring PNG colleagues and supporting scholarships, assisting with arranging teaching visits, arranging external examiners each year, assisting with international conference attendance, academic support and attending the annual medical symposium. There is now a significant need for an in-country professor of anaesthesia at UPNG. Two Presidents of ANZCA have visited and presented papers in PNG—Professor David A Scott and Dr Rod Mitchell.
Pain is a major neglected problem in low and middle-income countries. 32 The EPM course, designed by Roger Goucke and Wayne Morriss, has become a global standard for pain medicine education for these settings.33,34 This course was pioneered in PNG with the first course being run in Lae in April 2010 with Drs Gertrude Marun (Didei) and Harry Aigeeleng as the local champions. Since then, it has been run in over 63 countries, is in 16 languages, has an EPM lite version for medical students and now the recently released EPM online. 35 EPM is now co-badged with ANZCA and the World Federation of Societies of Anaesthesiologists (WFSA).
A prominent feature of ANZCA-sponsored assistance has been the regular teaching visits that are aimed at exam preparation for ASO, DA and MMed trainees. There have been enormous efforts from regular visiting tutors: Michael Stone, Wayne Morriss, Andrew Fenton, Richard Morris, Michael Cooper, Adri Cocciante, Jessica Lim, Roni Krieser, Chris Bowden and Peter Commons, with this list not being exhaustive.
ANZCA has also assisted with running specialty workshops such as airway management and ultrasound by Drs Chris Acott and Yasmin Endlich that have been an annual event at the medical symposium since 2009, SAFE obstetric anaesthesia courses with Drs Terry Loughnan, Anna Loughnan, Craig Noonan, Heather Loane, Suzi Nou, Nam Le and Maggie Wong and a SAFE paediatric anaesthesia course with Dr Michael Cooper in 2017.
ANZCA has also supported a book prize in anaesthesia since 1996 for the final MMed exam and later an undergraduate prize in anaesthesia. In 2012 the current prize system was commenced, also supported by ANZCA (Table 6).
Annual Australian and New Zealand College of Anaesthetists academic prize winners.
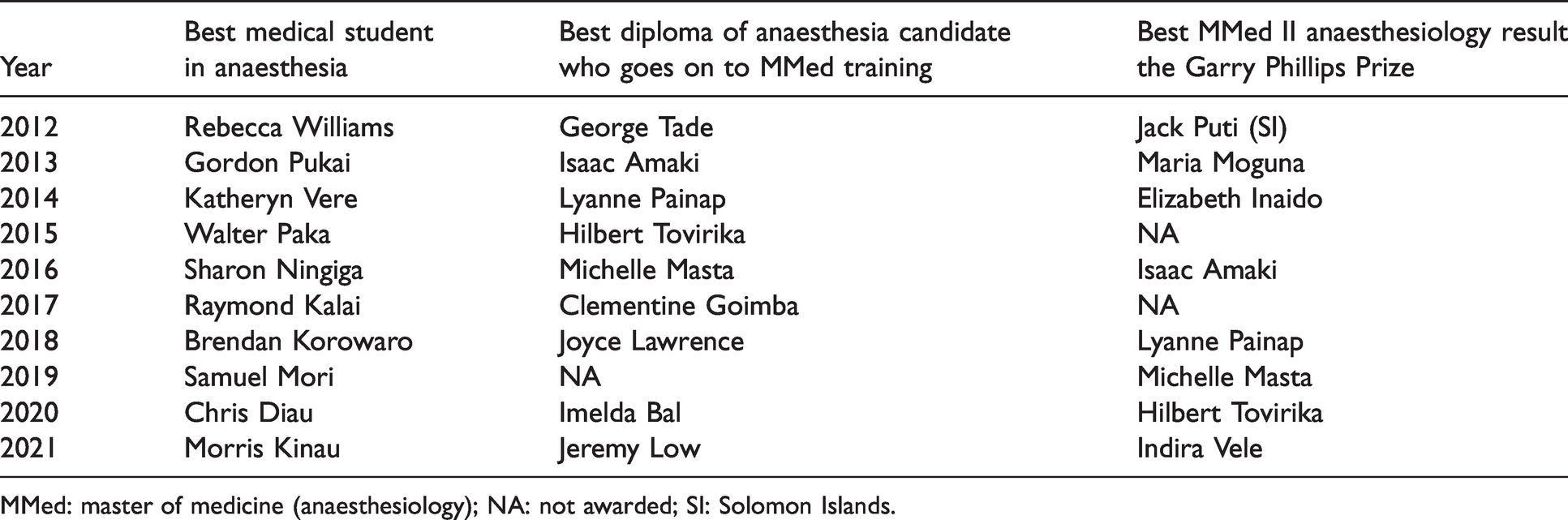
MMed: master of medicine (anaesthesiology); NA: not awarded; SI: Solomon Islands.
The SAPNG has been a member of the WFSA since 1992, with several members attending and speaking at the World Congresses of Anaesthesiology, and two anaesthetists have been the beneficiaries of WFSA scholarships (Table 3). Two presidents of the WFSA have visited PNG: Kester Brown (Australia) and David Wilkinson (UK).
The COVID-19 pandemic did not spare PNG and the anaesthetic community there has been the mainstay of treatment of very ill patients, mainly in the capital Port Moresby, and also a few other towns. The SAPNG has issued national guidelines to help steer this treatment. This has impacted on anaesthetic training and external support, and caused an even greater delay and disruption of normal healthcare than that seen in high-income countries.36,37 ANZCA has been providing personal protective equipment for the exams and donated many Lifebox pulse oximeters before and during the pandemic to most hospitals in the country.
In summary, the current system of national medical trainees undertaking specialist anaesthetic training in PNG started in 1984 and continues to expand. It is now 30 years since the first masters of medicine graduate in anaesthesiology and 40 have now graduated, with several candidates now passing each year. Continued support and investment in medical education is essential for PNG to progress.
In a country with as diverse a history as PNG, there have been many individuals from many different countries who worked in and taught anaesthesia and related disciplines there at various times. The authors apologise for any oversights and would like to hear from anyone who has been inadvertently omitted. Resources and documentation generated by this research will be lodged with ANZCA.
Footnotes
Author Contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the Heritage Grant from the Geoffrey Kaye Museum of Anaesthetic History at ANZCA.
Acknowledgements
The authors would also like to express gratitude to Maxine Wade at the Australian Society of Anaesthetists, Monica Cronin and Cassandra Gordon at ANZCA for their assistance in contacting colleagues who had worked in PNG; Anthony Wall and Kate Davis at ANZCA, Paul Cargill formerly at ANZCA for support with many PNG projects. They would also thank Dr Pankaj Patel, Dr Sivapalan Varatharajan, Dr Gajinder Oberoi, Dr Prakesh Kulkarni, Dr John Foley, Dr John Board, Dr Vic Callinan, Dr Wayne Morriss, Dr Duncan Dobunaba, Dr Nora Dai, Dr Gertrude Didei, Dr Arvin Karu, Dr Lisa Akelisi-Yockapua, Dr Magea Pole, Dr Lucas Samof and all of their colleagues who contributed their memories and insights into this project. The authors acknowledge their friends and colleagues—Professor John Vince and Professor Nakapi Tefuarani of the UPNG for their ongoing support to anaesthesia over many years, and Professor Frank Griffin, vice chancellor, UPNG. They also acknowledge the long-term support of their late colleague, Dr Lawrence Sogoromo.