
Abstract
The most recent estimates, published in 2016, have indicated that around 70% of anaesthesia providers in Papua New Guinea are non-physician anaesthetic providers and that they administer over 90% of anaesthetics, with a significant number unsupervised by a physician anaesthetist. Papua New Guinea has a physician anaesthetist ratio estimated to be 0.25 per 100,000 population, while Australia and New Zealand have a ratio of 19 physician anaesthetists per 100,000, which is 75 times that of Papua New Guinea. To reach a ratio of seven per 100,000, recommended as the minimum acceptable by the Lancet Commission in 2016, there will need to be over 35 practitioners trained per annum until 2030, at a time when the average annual numbers of recent years are less than three physicians and less than five non-physician anaesthetic providers. We review the development of anaesthesia administered by non-physician indigenous staff and the stages of development from heil tultuls, dokta bois, liklik doktas, native medical assistants, aid post orderlies, and Anaesthetic Technical Officers up to the current Anaesthetic Scientific Officers having attained the Diploma in Anaesthetic Science from the University of Papua New Guinea.
Keywords
New Guinea lies to the north of the Australian continent. It is the second largest island in the world and is split in half along the 141st meridian. The western half consists of the Indonesian provinces of Papua and West Papua, the eastern half is the sovereign nation of Papua New Guinea (PNG). 1 The population of PNG is estimated by the World Bank in 2019 to be 8,776,109 people, with a density of 15 persons per km 2 , with only 13% living in urban centres. 2
The first recorded anaesthetic administered on the island of New Guinea was on 9 December 1880 when an anaesthetic was administered by a Dr Goylan (or Goyan). It was administered at the Methodist Mission at Port Hunter, Duke of York Island, to Mrs Danks, the wife of a missionary, for removal of a retained placenta. It is not recorded what agent was used but both ether and chloroform were available at the settlement. 3
In 1884 the northern part was annexed by Germany to form German New Guinea and the southern part by Britain in 1888 to form British New Guinea. British New Guinea subsequently became known as Papua from 1905 and was transferred to the Commonwealth of Australia as a trusteeship in 1906. After the First World War, Australia took over control of German New Guinea under a League of Nations mandate. Australia thus administered the entire eastern half of the island but under two different administrations. Papua and New Guinea were administratively joined in 1949 to be governed as a single entity known as the Territory of Papua and New Guinea. Papua New Guinea attained independence in 1975. 4 One official language of PNG is Tok Pisin (along with English and Motu) and where Tok Pisin words are used we have added the English translation.
Sir Hubert Murray, Lieutenant-General and Chief Judicial Officer of Papua wrote in 1925: … Papuan had proved himself thoroughly competent at any work he was put to, from tapping rubber to driving an oil-launch, from administering anaesthetics in the operating ward to the installation of telephones.
5
… as will be seen from Dr Strong’s very interesting report, they can be taught such delicate work as skin-grafting; indeed, the Medical Officer at Samarai even has a native whom he entrusts with the administration of anaesthetics when he has to perform an operation.
6
Heil tultuls, medical tultuls and tultuls
Table 1 demonstrates the timeline of the introduction of non-physician anaesthetic providers (NPAPs) in PNG.
In the north of the country, German colonists had undertaken a training programme of developing medically trained local village members, heil tultuls, who were based in their own villages and provided a level of basic healthcare. In the Tok Pisin language, a tultul was a village official (assistant to the village chief or luluai) in colonial times (see Figure 2). 7 There were both administrative tultuls and medical tultuls. These were not full-time posts. This programme is recorded as having commenced around 1903. 8 In 1913, female health assistants were also appointed, primarily to promote the health of mothers and babies, but their numbers were very limited. 9
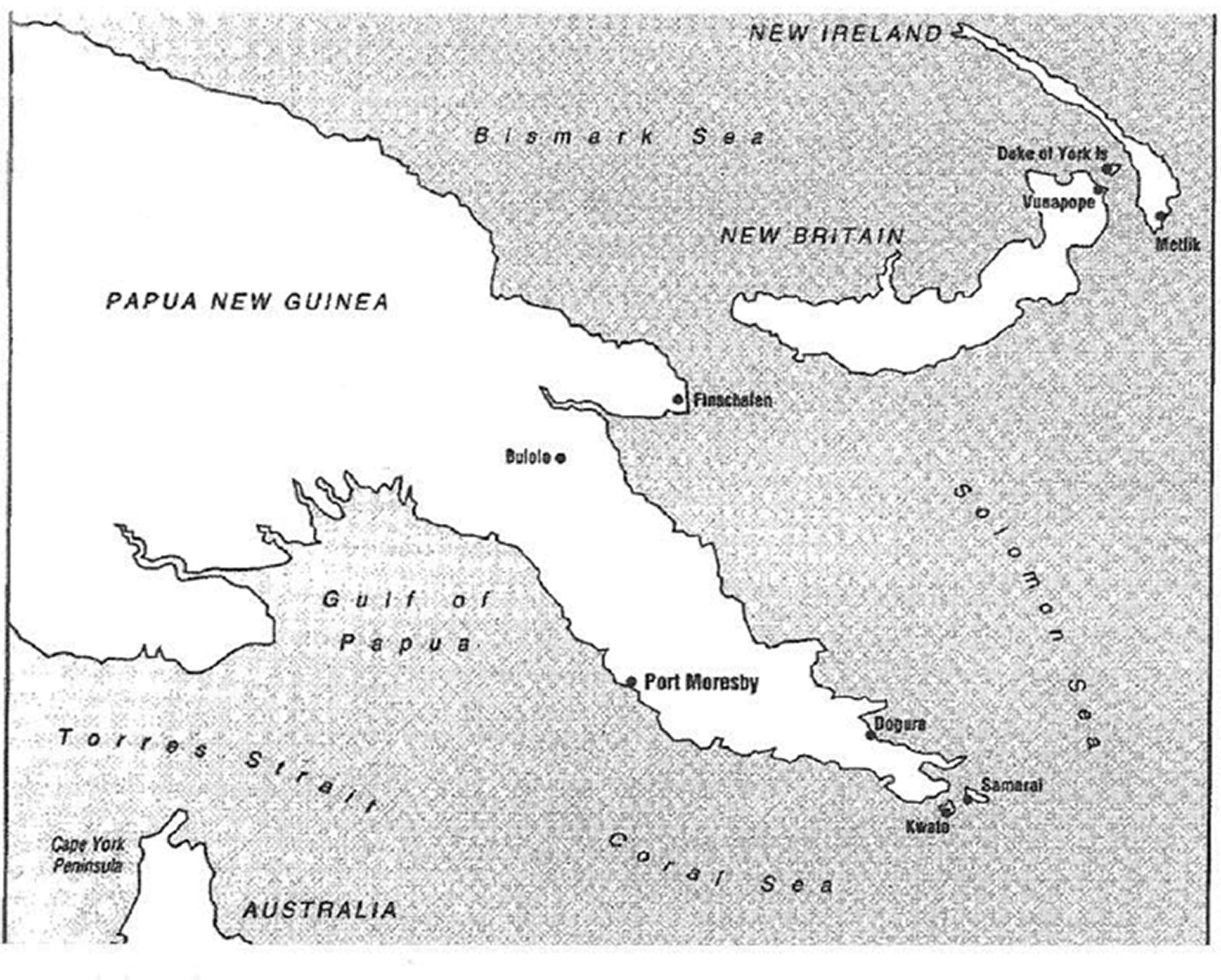
Map of Papua New Guinea,1908 from Phillips. 3

A tultul badge c. 1940s worn often on a hat or cap by the assistant to the village chief. It features the Australian coat of arms. Photograph by MG Cooper.
The heil tultuls were trained to administer injections but it is not recorded whether they administered anaesthetics, although they were trained to the level of administering intravenous drugs and assisting at operations.
10
Anaesthesia was predominantly for emergency care, by expatriate staff or under the direction of the surgeon. This level of medical care was usually provided by companies for their employees. Between 1914 and the outbreak of the Second World War medical ‘assistant training’ continued under Australian administration and there were approximately 4000 medical tultuls in the early 1940s. MacPherson described that after the First World War the Australian administration reduced the emphasis on heil tultuls being village based but promoted a system of rural aid posts and health centres: … the tultul was taught how to dress and treat tropical sores and other diseases, the recognition of cases requiring hospital treatment, administering treatment ordered by medical assistants, assisting at operations, elementary rules of sanitation and the methods of quarantining of infectious diseases.
11
Native medical assistants and aid post orderlies
In the 1930s Dr Walter Strong, then director of public health, developed a training programme for national (‘native’) medical assistants (NMAs). These assistants were trained in short courses in Sydney and later in PNG but were not thought to have enough school education to be able to cope with the medical school course in Suva, Fiji, which had been open since 1886. This training programme continued until the Second World War. 12
After the Second World War, John Gunther (later Sir John) was appointed director of public health, and aid post orderlies (APOs) were trained to replace their pre-war counterparts.
13
While this was occurring, a system commenced in 1946 in which Papuan and New Guinean students were sent to the Central Medical School in Fiji, for a five-year course which qualified them as native medical practitioners, later described as assistant medical practitioners, or assistant medical officers.
14
Although much inferior in status and certainly remuneration to medical doctors recruited from overseas, these graduates did virtually the same work as the doctors, particularly in rural health centres.
15
In the book Taim bilong masta (a Tok Pisin term referring to the colonial era), Gunther recalls:
4
One of the greatest boons that we had followed a discussion that I had with Nugget (Dr H C) Coombs who was then head of Post-War Reconstruction. He suggested that CRTS funds, Commonwealth Reconstruction Training Scheme funds, could be used for Papua New Guineans. It was really stretching the provisions of the scheme to the ultimate, but we grabbed this and started what I called a Native Medical Assistant Training Scheme, afterwards known as the Aid Post Orderly Scheme. I say quite proudly that we were just twenty years in front of the Chinese barefoot doctors. They adopted almost exactly the same principles as we did. We trained people, completely illiterates, to recognise major killing diseases, to use the specific drugs, and we sent them back to their villages. We taught them to their capacity in a matter of twelve months to two years. Now this was the quickest way we could get help to the villages. We had six or seven of these training schools spread through Papua New Guinea. At the base of it were simple village procedures to control common and debilitating diseases by the widespread use of aid-post orderlies (dokta bois – ‘doctor boys’ in Tok Pisin), village men with sufficient rudimentary training to administer a range of simple remedies for the most common maladies. More serious problems requiring constant care were brought to centres presided over by medical assistants (liklik doktas – ‘little doctors’ in Tok Pisin), while the seriously ill proceeded further up the chain to district and regional hospitals where specialist services were available from fully qualified staff. With this was associated the development of training opportunities for PNG nationals at all levels of the health service to the community.
4
Patrol officers, who were usually Australian, often had medical duties and also were called on to act as NPAPs on occasion.
4
A story is recorded of an anaesthetic administered by a kiap (an Australian patrol officer) so that a medical assistant could remove an axe from the skull of a man. I got a young patrol officer to administer the anaesthetic and I took the axe out. I had to cut down onto the bone, break an edge of the bone, and ease the axe out. It had penetrated the brain, and there was some infection. I used the old army technique of sulphanilamide and vaseline gauze packs, cleaned up all the mess and hoped for the best.
4
I spent a year doing a variety of things, then made up my mind to go to Papua New Guinea as a Cadet Patrol Officer. There I had more exposure to medicine. On numerous patrols to the interior and along the coast of the Gulf of Papua, I was administrator, surveyor, policeman, postman, health worker etc.
20
He credits this period with instilling in him an interest in medicine as a career and in PNG as a place. It would not be until 1993 that he would return as an instructor on the first Early Management of Severe Trauma (EMST) course conducted in PNG. From around 2000 he would return to PNG regularly to examine and instruct in anaesthesia, and assisted in the introduction of the Diploma in Anaesthetic Science (DAS) course that would commence in 2003. He was also appointed as the Visiting Professor of Anaesthesia at the University of Papua New Guinea. 20
Anaesthetic Technical Officers
This certificate apprenticeship-style course commenced in 1967 during the tenure of Dr John Foley as senior anaesthetist at Port Moresby General Hospital (PMGH). Dr Foley had arrived in PNG in 1963 with the Diploma of Anaesthesia qualification from the United Kingdom. He had already established an intensive care unit in Port Moresby that could ventilate patients predominantly with tetanus or Papuan taipan snake envenomation. In 1967 I had some study leave in England. While there I attended a seminar in Cambridge on anaesthesia in developing countries. A doctor from East Africa spoke of his program for training anaesthetic nurses, using an EMO anaesthetic machine. Upon my return I was able to start such a program working with what were then called Medical Assistants. The first course was with two such students for a year. Subsequently they went out into smaller hospitals to work on their own, or under the general supervision of the surgeon. On a visit to Goroka in December 1984 I was pleased to see one of those first two students anaesthetise for a Ramstedt procedure. (Open pyloromyotomy in an infant; TEL, personal communication, 2019)
This commenced in Port Moresby in 1967 with two students—John Pasiu and Gabriel Mandra. 16 A number of people were significantly involved in the training of local people under the ATO scheme. One was Ona Roma Cavill (née Varoneckas) (1937–2012). Roma was born in Lithuania and the family moved to Australia in 1947 where she completed medicine in Adelaide in 1961. She lived in PNG from 1962, initially in Mount Hagen then Port Moresby from 1965, leaving in 1977. She trained in anaesthesia under Dr John Foley from 1967 and subsequently continued training the ATOs. Returning to South Australia in 1977 she set up in general practice where she worked for 30 years in Glen Osmond.16,22
Dr John Board was an anaesthetist recruited to Lae after meeting John Foley when he was in his final year of training in Sydney. He spent 1971–1974 working in Lae and Goroka and remembers ATOs working unsupervised in Lae when he arrived, and that he then continued training ATOs sent from Port Moresby while in Lae. He does not recall any ATO training in his time in Goroka. In 1972 Dr Ronald Rae, an Australian qualified anaesthetist from Tasmania, had replaced Dr John Foley and was continuing the ATO training course in Port Moresby. John Board recalls Peter Mavad and John Ninkama as ATOs at that time (TEL, personal communication, 5 October 2020).
In the World Health Organization (WHO) review of health in PNG in 1978 there were listed 225 doctors, 288 HEOs, 1632 aid post orderlies, 1518 registered nurses and 1053 nurses’ aides.
23
So there was still a marked distribution weighted away from trained medical doctors for the provision of healthcare. A search of that 266-page document failed to find a single reference to the word ‘anaesthesia’. The health extension officer (HEO) is a person trained to provide a comprehensive health care and health improvement service at the intermediate level. This service is based on the health centre. The health extension officer at a health centre is responsible to the Provincial Health Extension Officer, who in turn is responsible to the Provincial Health Officer. Candidates for training must have a minimum of grade 10 education with credits in English, mathematics and science. The only school for health extension workers in the country is the College of Allied Health Sciences located in Madang, Madang. It offers a three-year course, including one year of community health practice. However, after graduation and registration, an additional one year of internship is required before the students are posted to a position of responsibility. In 1980 there were 22 new graduates and in 1981 there will be 25. The school is expected to increase its enrolment to fill the needs of the health services for 32 new graduates a year.
23
The ATOs were trained well and successfully completed their exams satisfactorily. Both Dr. Patel and I continuously upgraded their knowledge by visiting the peripheral hospitals time to time. An ATO training centre was in the Highlands. Whenever I visited the local hospitals, I talked to them on resuscitation, particularly. Envenomation was a common occurrence. Antivenin was administered at the site, patient intubated by the ATO and transported by air, hand ventilated. ICU at the PMGH had many such patients. Nurses from the neighbouring island countries followed the ATO course in Port Moresby. They were keen and eager to learn. It was a pleasure to teach them too.
Dr Harry Aigeeleng referring to ATO training in the 1990s remembers: I am not aware of a specific training centre for ATOs. But I know that certain hospitals like PMGH, Goroka, Lae, Mt. Hagen and Madang had anaesthetists who were given the responsibility by the Training Division of the National Dept of Health to run training for ATOs. I believe these anaesthetists may have met and put together a curriculum that they used for training. I have not seen this document when I became an Anaesthetist. I trained my ATOs using Anaesthesia at a District Hospital
25
and Synopsis of Anaesthesia.
26
The following is how I conducted training for ATOs basically by observing what the anaesthetists were doing when I was a registrar. Candidates were identified usually by surgeons of respective hospitals in need of an ATO and sent to the nearest anaesthetist for 12 months training. The training was mainly on-the-job with some theory at the table side and usually with the above books as recommended texts to read and make notes in preparation for the exam. Because mentoring is usually 1–1 or at times 2–1, the exam is set only after the anaesthetist is satisfied that the candidate practices safe anaesthesia. Sometimes it may exceed 12 months before the candidate is deemed safe to practice. (personal communication from Dr Aigeeleng to TEL, August 2019).
Anaesthetic Scientific Officers and the Diploma in Anaesthetic Science
In 2005, Professor Garry Phillips stated: I had become aware over the first few years that most of the anaesthetics in PNG were administered by Anaesthetic Technical Officers (ATOs), who were nursing or other health graduates who had done a year’s apprenticeship under a specialist, starting back in the 1960s. After organizing a total of six workshops for these people, held in Port Moresby, Madang and Mt Hagen, it was decided that it would be better for the program to be transferred to the University of PNG as a Diploma in Anaesthetic Science (DAS), the graduates being called Anaesthetic Scientific Officers (ASOs). In addition to retaining the apprenticeship component, a University standard educational program was put in place. This was achieved with the assistance of Dr Harry Aigeeleng, Professor Mathias Sapuri, the Dean, and one of the experienced ATOs, Mr Marx Yabri, who became the coordinator of the course. Within three years, an estimated 60% of existing ATOs had converted to the Diploma of Anaesthetic Science, and new entrants had commenced to graduate.
20
Professor Garry Phillips, Visiting Professor (University of Papua New Guinea), Dr Gertrude Marun (nee Didei), chief anaesthetist, and Dr Harry Aigeeleng, senior lecturer, were able to design a two-year diploma programme. Originally the university requested a four-year degree programme starting with a one-year science foundation and then three years of clinical training, but it was proposed by the anaesthetists and agreed that the course should require students with experience and training in health, emergencies and life-threatening situations. It was felt that qualified nurses and HEOs would be more suitable and that their prior learning be taken as the first year that would automatically score the points for year 1 and the programme that was written by Phillips, Marun and Aigeeleng became that for year 2.
27
The ATOs were consulted all along during that period. They did their own research and brought to our attention that there must be a change of name from Anaesthetic Technical Officer (ATO) training to Anaesthetic Scientific Officer (ASO) training. The senior ATOs noted that on the salary scale the Diploma would be meaningless if the title ATO was not changed. A technical officer earns less than a scientific officer on the Public Service salary scale. Prof. Garry Philips presented this to the Academic Board and was accepted in time in 2002 for us to start the program in 2003. (personal communication from Dr Harry Aigeeleng to TEL, August 2019).
They then go to full-time clinical work at PMGH where they are exposed to obstetric and paediatrics as well as all of the general specialties. They are rostered on call and experience an elective and emergency caseload. In October each year they undertake examinations and then have a six-week elective period. This can be taken in their home hospital if there is a specialist anaesthetist to supervise, otherwise they stay in Port Moresby. They complete their year in the first week of December. They must complete a logbook of their cases and this involves a minimum volume of practice. There is no semester break in this course. An outline of the course and logbook minimum volume of practice is shown in Appendix 1.
As a result of this, ASOs now have a university qualification. They do not have any annual continuing medical education requirement but are entitled to attend the annual PNG Medical Society Symposium which includes the Society of Anaesthetists of PNG (SAPNG) annual meeting. This includes attending specific workshops such as Airways and Basic Life Support courses run annually by Drs Chris Acott and Yasmin Endlich from Adelaide.
The chief anaesthetist for PNG has made it mandatory for all ASOs and anaesthetists attending the symposium to attend the workshops, funded from their hospitals, every two years. ASOs also attend Essential Pain Management (EPM) courses and Safe Anaesthesia from Education (SAFE) obstetric and SAFE paediatrics courses. The Australian and New Zealand College of Anaesthetists (ANZCA) have supported ASO training in PNG since its inception in 2003 with teaching visits and attendance at the annual medical symposium (Figure 3). This has been supported by Richard Morris, Garry Phillips, Michael Cooper, Roni Krieser, Mick Stone, Peter Commons, Jessica Lim, Fiona Reardon, Andrew Fenton, Adriano Cocciante, Steve Threlfo (biomedical engineer), Chris Acott, Yasmin Endlich, Terry Loughnan, Craig Noonan, Heather Loane, Suzi Nou, Anna Loughnan, Maggie Wong, Nam Le, Geoff Gordon, Mike Tronson, Phil Ragg, Chris Bowden, Wayne Morriss and Zoe Lagana.

Some of the extended Papua New Guinea (PNG) anaesthesia family. PNG Medical Symposium, Port Moresby, September 2017.
Progress of the ASO programme
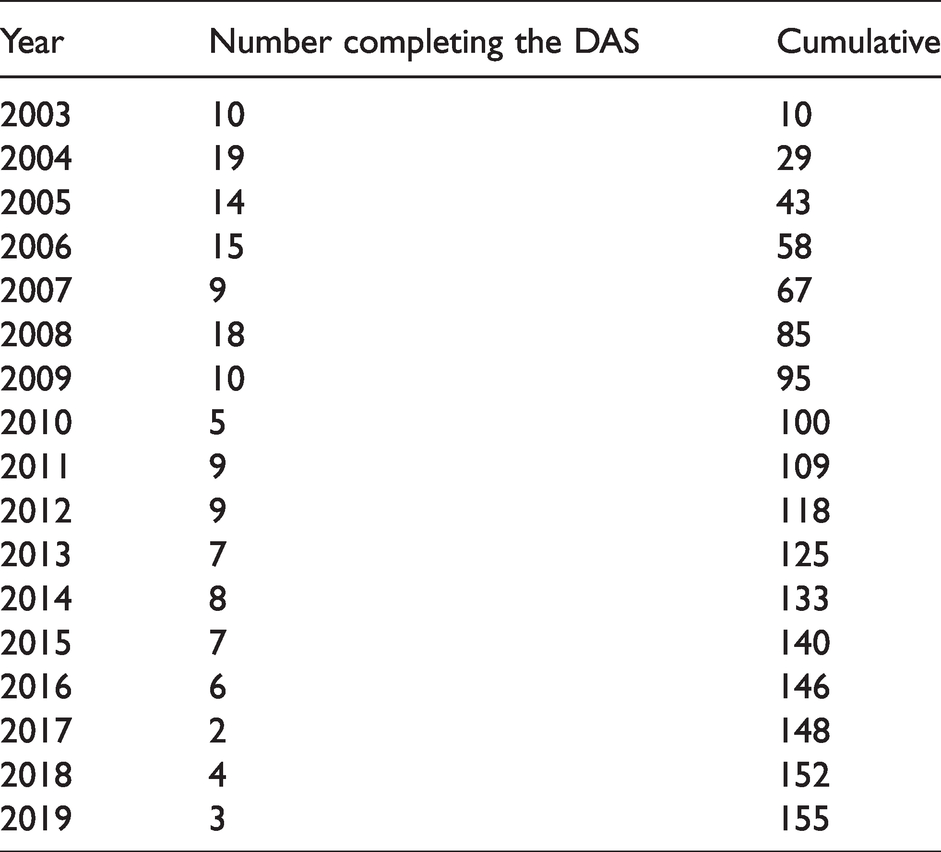
Table 2 shows the number of DAS graduates each year. The number of DAS graduates at the start was high because there was an opportunity for people working as ATOs entering into the diploma course to upgrade their qualification. However, the numbers of entrants have dropped off steadily, with low numbers since 2009. An arrangement that enabled ATOs to upgrade was that after completing their classroom education in Port Moresby they returned to their hospitals to continue anaesthetic services until returning to sit exams. This was an acceptable response to what would have become a staffing crisis, had ATOs left their posts for a year. At present two DAS candidates and about the same number of MMed candidates graduate per year which is far below the 35 per annum required to reach the minimum numbers of practitioners as recommended by global workforce surveys. 28 The global anaesthesia workforce survey was conducted in 2015. It is now 2020, so in the years 2016–2020 there needed to be 140 persons trained and, in the time, there have been 13 PAPs complete the diploma, six complete MMed training and 15 ASOs—a total of 34. This is far below the minimum required numbers, and there have also been retirements and deaths among anaesthetic staff in PNG.
Timeline for introduction of non-physician anaesthetic providers in Papua New Guinea.
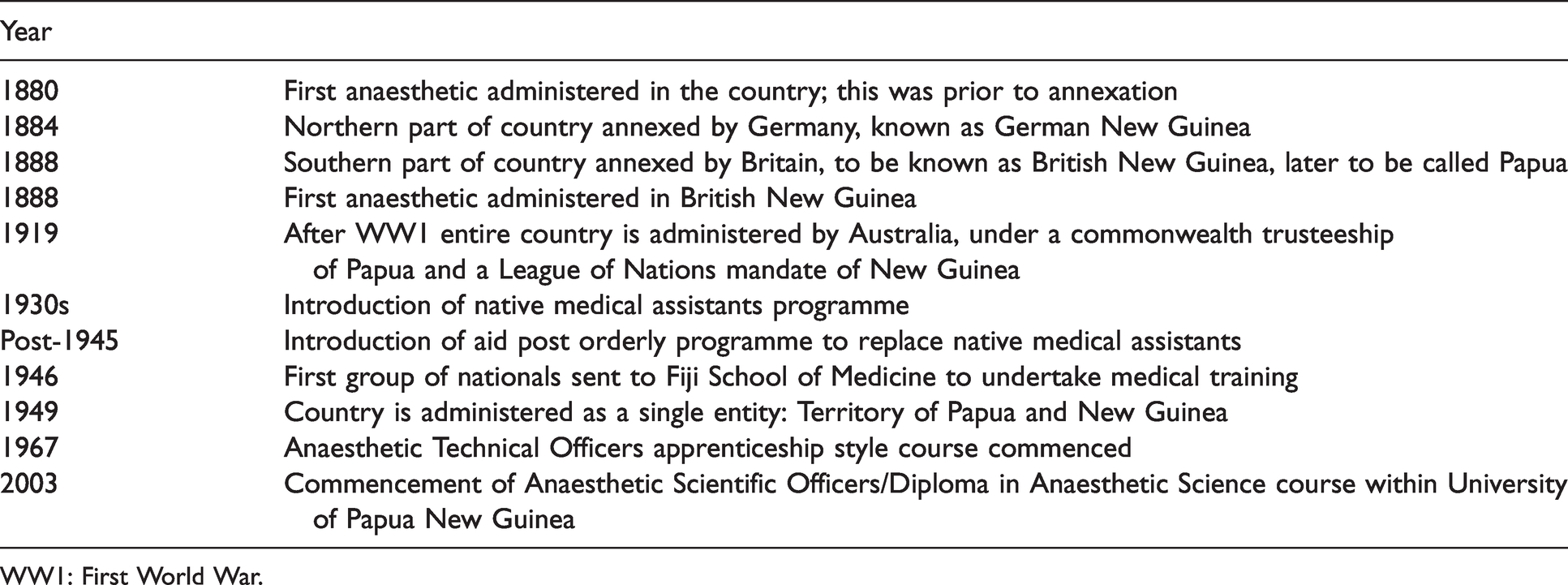
WW1: First World War.
Progress of Anaesthetic Scientific Officers completing the Diploma in Anaesthetic Science course at the University of Papua New Guinea.
Current situation
The PNG national health system is based on a decentralised model. It consists of a network of 2500 aid posts (1800 functional), approximately 800 sub/health centres, 21 provincial hospitals and one national referral hospital (PMGH, which also operates as a provincial hospital). The government and church-based providers predominantly provide health services. 29
In 2016, Cooper et al. wrote that the Lancet Commission estimated that the required minimum number of specialist anaesthetic physicians in low and middle-income countries should be seven per 100,000 head of population. The incidence of physician anaesthesia providers (PAPs) in PNG was estimated to be 0.25 per 100,000 population compared to 19.1 in Australia. In PNG, of the 99 anaesthesia providers, 19 were physicians and 80 were NPAPs, with a further ten trainees. It is estimated that by 2030 there will need to have been 523 anaesthetic providers trained to achieve the WHO goal of seven per 100,000 and this represents 35 graduates per annum. 28
The World Federation of Societies of Anaesthesiologists (WFSA) anaesthesia workforce survey of PNG estimated 45 PAPs, which included trainees and some in administration, and 94 NPAPs with a combined total of 1.82 per 100,000, and noted that 68% of providers were NPAPs many of whom work without PAP supervision. 30 While these numbers are slightly different, the overall picture is entirely consistent with a health system structure heavily dependent on NPAPs who do the vast majority of cases and in many cases work unsupervised by a physician anaesthetist. Overall, in the Pacific region there are twice as many NPAPs as physician anaesthetists. 28
Many low- and middle-income countries will require this team-based approach of task-sharing between NPAPs and physician anaesthetists for many years to come,31,32 and this will be particularly important in PNG.
The current system of training for NPAPs of a DAS at the University of Papua New Guinea commenced in 2003 and has since graduated 155 diplomates up till the end of 2019. To meet increasing anaesthesia service demands with rapid population growth, there is a major need for increased PAPs and NPAPs in PNG.
Footnotes
Author Contribution(s)
Acknowledgements
The authors would also like to express their gratitude to Maxine Wade at the Australian Society of Anaesthetists, and Monica Cronin and Cassandra Gordon at the Australian and New Zealand College of Anaesthetists for their assistance in contacting colleagues who had worked in PNG. They would also like to thank Dr Pankaj Patel, Dr Sivapalan Varatharajan, Dr Gajinder Oberoi, Dr Prakesh Kulkarni, Dr John Board, Dr Vic Callanan, Dr Wayne Morriss, Dr Duncan Dobunaba, Dr Gertrude Didei, Dr Lisa Akelisi-Yockapua, Dr Magea Pole, and all of their colleagues who contributed their memories and insights into this project, without which it would not have been possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the heritage grant from the Geoffrey Kaye Museum of Anaesthetic History at the Australian and New Zealand College of Anaesthetists.