
Abstract
Airway management in patients presenting with severe airway obstruction can present a challenge to the anaesthetist, as conventional difficult airway pathways are often inappropriate. The use of a transtracheal jet cannula is an alternative means of airway securement, but lack of familiarity has limited its use in general tertiary hospitals. We report a retrospective audit of the use of transtracheal jet ventilation in a general tertiary healthcare centre over the past seven years, with a total of 50 patients with severe airway compromise undergoing pharyngolaryngeal surgery. Transtracheal jet ventilation was successful in 98% of patients, and was the definitive means of airway management in 43 cases. In six cases, the technique was a useful temporising measure while the airway was secured by other means. Minor complications occurred in 12% of patients. No major morbidities or mortalities were recorded. We conclude that transtracheal jet ventilation for high-risk pharyngolaryngeal surgery can be performed using a high frequency jet ventilator, with a high rate of success and only minor complications. Cannulation of the trachea below the cricothyroid membrane is feasible but more challenging. Low-flow apnoeic oxygenation through the transtracheal jet ventilation cannula maintains oxygenation during initial surgical airway manipulation.
Introduction
Approaching the difficult airway in elective pharyngeal or laryngotracheal surgery can be challenging, particularly because the standard algorithms for difficult airway management often do not apply. 1 , 2 Fibreoptic intubation, in many settings the gold standard for securing the airway awake, can be hazardous and/or unsuccessful in the patient with laryngeal pathology. 3 Elective tracheostomies, often regarded as the fail-safe technique of choice, are now less frequently performed, are not without significant morbidity, and are an unpleasant experience for the awake patient. 4
An alternative is transtracheal jet ventilation (TTJV). In this technique, the trachea is accessed with a percutaneous cannula, inserted via the cricothyroid space or between tracheal rings. The patient is then jet ventilated, either at low frequency using a manual device, or by means of a high frequency jet ventilator (HFJV). First described by Spoerel et al. in 1971, 5 the technique has been used in both emergency and elective anaesthetic procedures, either as the definitive method of ventilating the patient for the entire case, 6 , 7 or as a temporising measure.8–10 Recently, a case series by Ross-Anderson et al. focused on the use of TTJV in elective ear, nose and throat (ENT) patients presenting with significant airway compromise. 11
Using the techniques and safety parameters described by Ross-Anderson et al., 11 we have implemented the use of elective TTJV in our institution, a general tertiary healthcare centre where elective laryngotracheal surgery is performed on a regular basis. Given the infrequency of the use of the technique locally, we have performed an audit of 50 cases and would like to report the outcomes we observed, as well as the lessons we learnt along the way.
Methodology
A review of the use of TTJV at our institution was performed for the years 2012–2018 inclusive, based on a de-identified internal database kept by the Department of Anaesthesia listing all TTJV cases since our initial use of the technique in 2012. Ethics approval was sought and obtained prior to commencement of the review process (Monash Health Human Research Ethics Committee ref: RES-18-0000-462Q).
We included all patients presenting electively for laryngotracheal surgery on whom TTJV was performed. The main indication for TTJV in these patients was laryngotracheal obstruction in which conventional airway approaches were deemed difficult or impossible. Other factors included the preference of the anaesthetist and surgeon involved in the patient’s care, the patient’s anatomy based on clinical presentation and radiological examination, the degree and level of airway obstruction, and patient wishes. It was essential that, based on imaging and other assessment, the treating anaesthetist would be able to place the jet cannula inferior to the airway lesion.
All procedures were performed in the operating theatre, with the ENT surgeon in close attendance. Procedures were performed either by consultant anaesthetists experienced in ENT cancer anaesthesia, or by senior anaesthesia trainees under their direct supervision. All consultant anaesthetists directly or indirectly involved with these cases were familiar with the use of HFJV, and were able to troubleshoot any issues that arose with the cannulation.
Our technique closely followed that outlined by Ross-Anderson et al. in their aforementioned case series, 11 which included ventilation using HFJV. Patients were started on a remifentanil infusion at 0.05 µg/kg/min prior to tracheal cannulation to provide mild sedation and analgesia, while maintaining consciousness and a patent airway. The patient was positioned on the operating table with the neck extended. Monitoring was applied and supplemental oxygen given via nasal prongs or a nasopharyngeal catheter. After preparation with alcoholic chlorhexidine, the skin was infiltrated with 2% lidocaine. Initial puncture at the chosen level was with a 23 g hypodermic needle, to allow intratracheal administration of 2 ml of 2% lidocaine. See supplementary video 1, available online.
The transtracheal cannula used in all but one case was a 13G VBM jet ventilation catheter (Ravussin VBM Catheter; VBM Medizintechnik GmbH, Sulz Am Neckar, Germany). Confirmation of correct placement of the cannula in the trachea was by both aspiration of air into a saline-filled syringe and attachment of capnography to the jet cannula. See supplementary video 2, available online.
After pre-oxygenation, the patients were induced using a propofol bolus ranging from 1.5 to 3 mg/kg. Muscle relaxation was achieved using atracurium 0.5 mg/kg. Anaesthesia was maintained using propofol plus remifentanil total intravenous anaesthesia (TIVA).
After satisfactory placement of the surgical laryngoscope, patients were ventilated using a Monsoon high frequency jet ventilator (Acutronic Medical Systems AG, Hirzel, Switzerland), with an initial driving pressure of 1.0 bar, a frequency of 120 breaths per minute, fractional inspired oxygen (FI
From 2016, an addition to our technique involved the use of low-flow apnoeic oxygenation via the transtracheal jet cannula, once the cannula was successfully placed. From that time, this formed part of the initial airway management for most cases. This was achieved by connecting the transtracheal cannula to an oxygen flowmeter running low-flow oxygen (<0.5 L/min), a standard oxygen tubing, a three-way tap with the third outlet closed, and a short intravenous extension with Luer lock connectors. The technique is depicted in Figure 1.
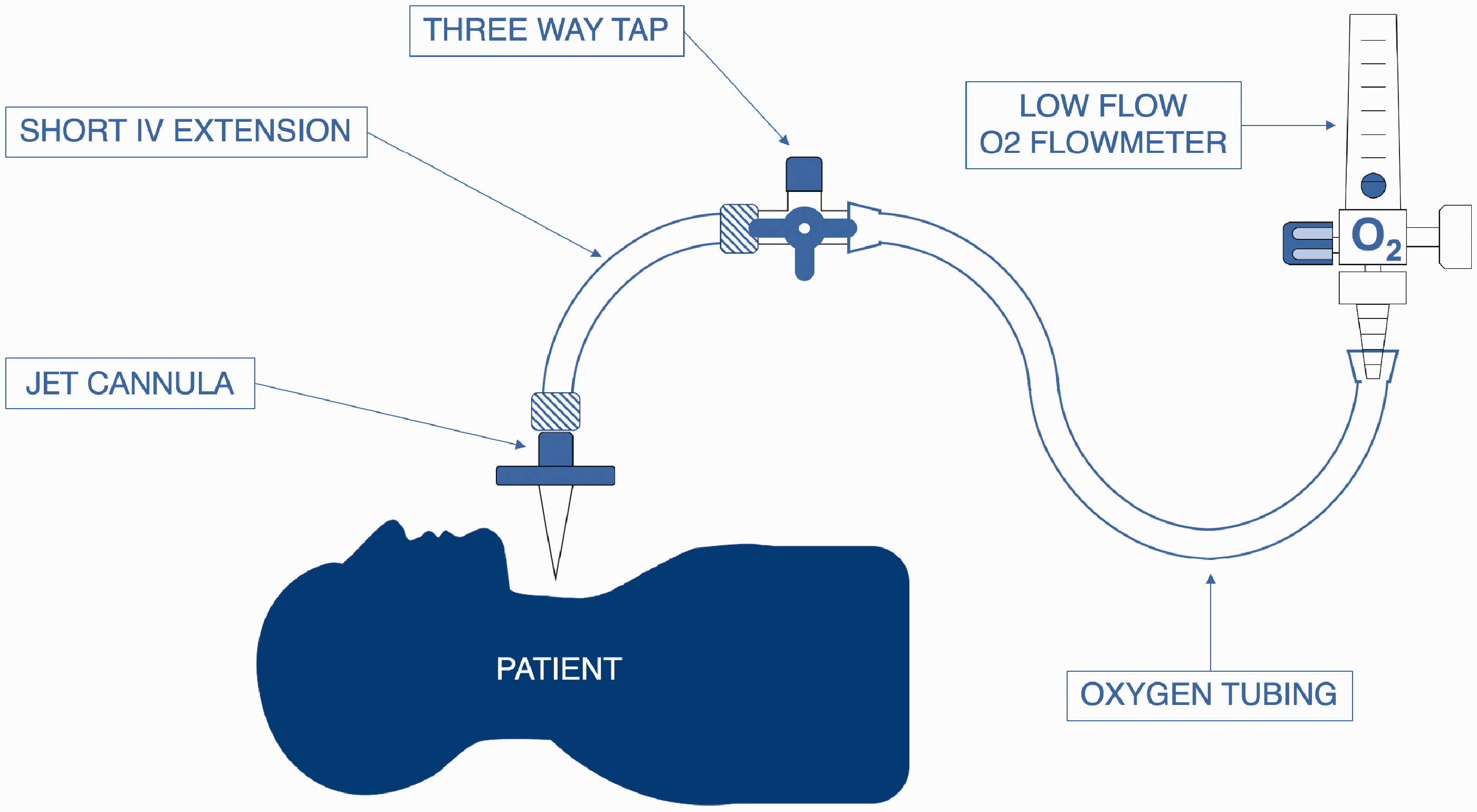
Our set-up for apnoeic oxygenation via transtracheal jet cannula. Safety precautions: low-flow oxygen only – 0.5 L/min was our preferred upper limit.
At the end of surgery, a laryngeal mask airway (LMA) was inserted. Ventilation was tested via the LMA, residual neuromuscular block was reversed with neostigmine and, upon return of adequate spontaneous ventilation, the patient was taken to the recovery ward. The jet cannula was removed once the patient was awake and ready to return to the post-surgical ward.
The database included patient details, procedural details and general comments. Patient details included the patient’s age, American Society of Anesthesiologists (ASA) physical status classification and the pathology which necessitated surgery. Procedural details included the needle used, site of puncture (cricothyroid, tracheal or low tracheal, the latter arbitrarily defined as being ‘close to the sternal notch’), number of passes required to secure the airway and any failed attempts. General comments included complications or any details we felt were pertinent for further learning.
Results
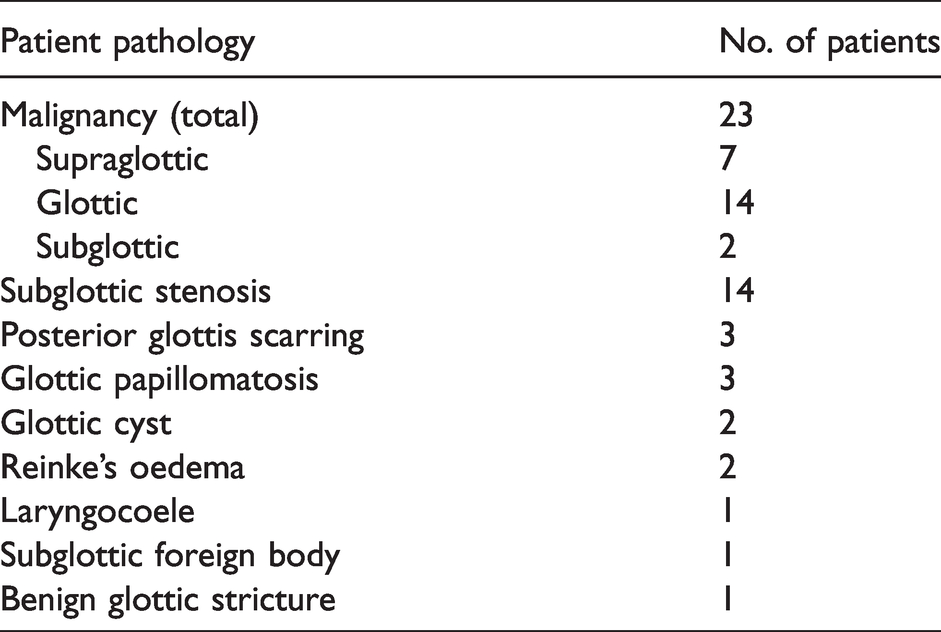
Fifty cases were identified. The mean age of the patient cohort was 66 (range 36–86) years. The ASA physical status (PS) classification for the patients ranged from ASA-PS 2 to ASA-PS 4. Table 1 is a list of surgical diagnoses. The majority of the cases were performed electively, with 48 patients scheduled for an elective theatre list, whereas in two patients TTJV was performed in a semi-emergent fashion.
Patient pathology.
The site of puncture was evenly distributed between cricothyroid, tracheal and low tracheal. Airway access was successful on first pass in 60% of the patients, second pass in 22% of patients, and three or more passes in 16% of patients. Forty-nine out of 50 patients were successfully cannulated. In one patient, the procedure was abandoned after three unsuccessful attempts.
The one failed case was a patient presenting with Reinke’s oedema, with significant inflammation of not only her vocal cords but also the surrounding tissues, making anatomical assessment of landmarks challenging. Three attempts at the tracheal level were made to pass the jet cannula, all of which were unsuccessful in locating the tracheal space. The patient was then intubated successfully endotracheally with a microlaryngoscopy tube, and surgery proceeded uneventfully.
Table 2 shows the number of passes required for cannulation versus the level of cannulation.
Number of passes versus location of cannula puncture.
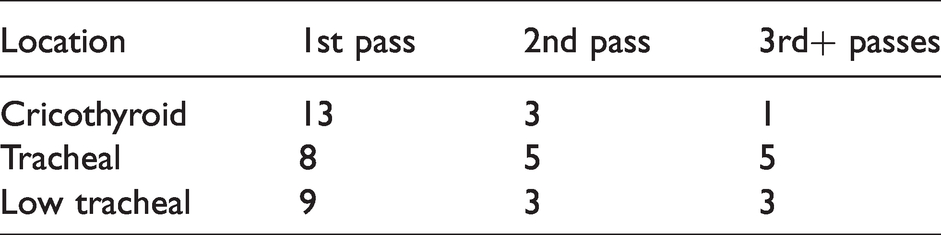
Cannulation at the cricothyroid level was successful at first or second pass on 16 out of 17 occasions.
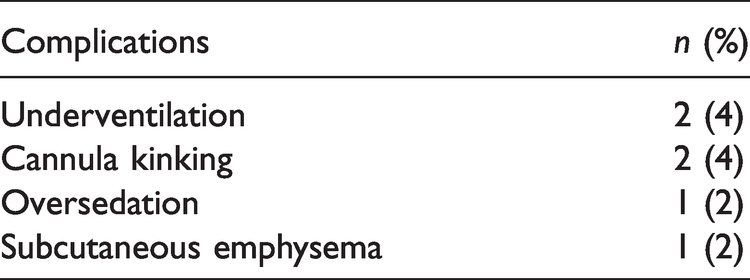
Six complications, all minor, were reported, for an overall complication rate of 12%. Table 3 lists the complications encountered. The most significant was a case of postoperative subcutaneous emphysema, without airway compromise. The patient was transported to the intensive care unit for overnight monitoring in a stable condition, and the subcutaneous emphysema resolved spontaneously. One patient was excessively sedated by the remifentanil infusion and was bag-mask ventilated while the jet cannula was passed successfully. While excessive sedation is not a complication of TTJV per se, we felt it prudent to report it as a possible complication, given the danger of over-sedation in this patient group. Two patients had higher than anticipated end-tidal carbon dioxide (ETCO2) at the completion of the case on LMA insertion, indicating intraoperative hypoventilation. In two cases, kinking of the jet cannula resulted in failure of jet ventilation, with the need for insertion of a fresh cannula; one of these desaturated briefly, until jet ventilation was restored.
Complications.
In the majority of cases (43), ventilation for the entire case was with HFJV via the jet cannula. In two cases, the underlying surgical pathology necessitated the performance of a tracheostomy: in one case after initial passage of an endotracheal jet tube via the surgical laryngoscope; and in one case by using the jet cannula for passage of a wire which in turn allowed placement of a percutaneous tracheostomy tube. In four cases, oxygenation via the jet cannula was used as a temporising method while the airway was secured endotracheally: twice with bougie plus microlaryngoscopy tube; once with a surgically placed endotracheal jet tube; and once with a small endotracheal tube over a flexible fibreoptic laryngoscope, facilitated by the use of a hyperangulated videolaryngoscope.
Discussion
This audit is significant for two reasons. First, we affirm the existing literature that TTJV can be safely and effectively performed in the elective setting in patients presenting with severe airway obstruction, as evidenced by a 98% success rate of TTJV cannulation, and a low incidence of minor complications. The complications encountered—and the absence of significant morbidity or mortality—are consistent with those reported in previous series.6–12
Second, we have demonstrated that TTJV can be performed safely within an ENT head and neck cancer service within a general tertiary hospital. It is our opinion that several important factors contributed to the good outcomes documented in this audit: a small team of anaesthetists with experience in managing complex head and neck surgical cases; a perioperative team (including ENT surgeons, surgical nurses, anaesthetic nurses and anaesthetic assistants) all familiar with the technique; and the use of a high frequency jet ventilator.
For all our cases, we used a high frequency jet ventilator with high-pressure alarms and automatic cut-out should the pressure limits be exceeded. The most disastrous complication of high-pressure jet ventilation is barotrauma. The literature strongly suggests that the risk is higher with handheld, low frequency devices. 13 , 14 We believe that our use of HFJV has contributed significantly to the low complication rate.
This audit has yielded several valuable learning points.
The first concerns the technical aspects of tracheal cannulation. Reflection on our failed case led to the conclusion that the three attempts at cannulation were almost certainly extratracheal, with the curved VBM needle passing parallel to the tracheal wall. We believe an initial 90° angle of cannula to skin is the optimal approach for tracheal entry, with the angle then flattened to allow the needle and cannula to pass fully into the tracheal lumen. Our trainees have found it helpful to imagine the technique as analogous to cannulating a large, thick-walled vein.
It is important to have in mind that as the trachea descends from the larynx, it moves posteriorly into the mediastinum. 15 This makes entry at the tracheal level more difficult, as does the narrower space between the tracheal rings compared with the cricothyroid space. This is borne out by the higher requirement for second or third passes with cannulation at levels below the cricothyroid.
It is the opinion of the authors that detailed knowledge of individual patient anatomy is essential to the success of the technique. This is especially relevant in malignancy, where the operator must not only consider the spread of the tumour, but also anatomical anomalies and distortion of other neck structures due to the malignancy.
A previous review discussed the several advantages of the Ravussin VBM jet ventilation catheter, as well as the significant disadvantage that it can kink. 16 This occurred in two of our 50 cases, necessitating the passing of a new jet catheter. We believe this problem is more likely when the catheter has to pass through a greater distance to reach the trachea; that is, in larger patients and when the entry point is lower in the neck. We have on one occasion used a 6 French emergency transtracheal airway catheter (Cook, Bloomington, IN, USA) for transtracheal entry in a large male patient; we found it less liable to kink but more difficult to pass than the VBM catheter.
There has been increasing interest in the use of apnoeic oxygenation, particularly in ENT surgery. 17 We are experienced in the use of low-flow apnoeic oxygenation via endotracheal catheter in ENT microlaryngoscopy. 18 The use of low-flow apnoeic oxygenation via the transtracheal jet catheter was added to our technique after we found it to be a successful temporising measure during initial surgical debulking of a large, obstructing laryngeal tumour. When there is a major degree of airway obstruction, the repeated high-pressure alarms and automatic interruption of ventilation by the jet ventilator can be sufficient to prevent adequate ventilation and oxygenation of the patient. Low-flow apnoeic oxygenation safely maintains adequate oxygenation for at least ten minutes, giving the surgeon time to manipulate the operating laryngoscope and, if necessary, do some initial tumour debulking to open an adequate pathway for egress of gas.
We ascertained that the VBM jet ventilation catheter is laser-resistant (personal communication; VBM Medizintechnik GmbH, Sulz Am Neckar, Germany), meaning that laser could be used as part of the surgical technique if necessary.
A final point concerns patient empowerment, reduction of risk, and avoidance of morbidity. The use of TTJV resulted in a number of patients avoiding tracheostomies, which could potentially contribute to improved long-term outcomes and reduction in morbidity.19–21
A particularly memorable case was that of a patient with a large glottic tumour who expressed a strong desire to deliver a speech at his daughter’s forthcoming wedding. With the use of TTJV, he was able to avoid a tracheostomy while having his tumour debulked, and thus his wish to speak at his daughter’s wedding was fulfilled.
Conclusions
In summary, we believe that the low complication rate and high rate of successful completion of surgery demonstrate that TTJV can be performed safely in the elective setting for patients presenting for laryngotracheal surgery with severe airway compromise. We recommend careful patient assessment, the use of a high frequency jet ventilator with pressure monitoring and automatic high-pressure cut-out, and the presence of an experienced theatre team. In addition, apnoeic oxygenation via the transtracheal cannula appears to be a safe and helpful temporising measure in cases in which inadequate gas egress makes initial high frequency jet ventilation difficult. We hope that with increased awareness of the usefulness of this technique, it will be adopted more widely.
Footnotes
Author Contribution(s)
Acknowledgements
The authors wish to acknowledge the collegial support of the Monash Health ENT surgeons, in particular E Sigston, C Giddings and N Vallance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The individuals featured within the videos demonstrating the procedure have given their informed consent for the publication of the videos in the present work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.