
Abstract
Postoperative ‘enhanced care’ models that sit between critical care and ward-based care may allow for more cost-effective and efficient utilisation of resources for high-risk surgical patients. In this retrospective observational study, we describe an overnight intensive recovery model in a tertiary hospital, termed ‘recovery high dependency unit’, and the characteristics, treatment, disposition at discharge and in-hospital outcomes of patients admitted to this unit. We included all adult patients (≥18 years) admitted to the recovery high dependency unit for at least one hour between July 2017 and June 2020. Over this three-year period, 1257 patients were included in the study. The median length of stay in the recovery high dependency unit was 12.6 (interquartile range 9.1–15.9) hours and the median length of hospital stay was 8.3 (interquartile range 5.0–17.3) days. Hospital discharge data showed that 1027 (81.7%) patients were discharged home and that 37 (2.9%) patients died. Non-invasive ventilation was delivered to 59 (4.7%) patients and 290 (23.1%) required vasopressor support. A total of 164 patients (13.0%) were admitted to the intensive care unit following their recovery high dependency unit admission. Of the 1093 patients who were discharged to the ward, 70 patients (6.4%) had a medical emergency team call within 24 hours of discharge from the recovery high dependency unit. In this study of a recovery high dependency unit patient cohort, there was a relatively low need for intensive care unit admission postoperatively and a very low incidence of medical emergency team calls post-discharge to the ward. Other institutions may consider the introduction and evaluation of this model in the care of their higher risk surgical patients.
Introduction
The volume of surgical procedures continues to grow each year and patients undergoing surgery are ageing faster than the general population in many high-income countries. 1 Advancing age and increasing comorbidities will continue to present considerable challenges to perioperative management. 2 Higher levels of care are recommended for high-risk patients to minimise postoperative complications, morbidity and mortality. 3
With intensive care beds limited in many countries, there is a need to develop alternative models of perioperative care. Despite such need, extended post-anaesthesia care in this high-risk cohort remains an under-researched field.4,5 Moreover, the location and duration of post-anaesthesia care, the appropriate balance of anaesthesia or intensive care–led service provision, and risk stratification of the surgical patient cohort remain unclear. 6
There has recently been interest in models of ‘enhanced care’ that sit between critical care and ward-based care. 7 This can take the form of extended postoperative recovery room care, 8 enhanced recovery programmes 9 and even mandated high dependency unit (HDU) admission based on predictive mortality modelling, such as the National Emergency Laparotomy Audit in the UK.10,11 ‘Enhanced care’ models may improve the quality of patient care, decrease workload on ward staff, reduce cancellation of elective surgery and allow for more cost-effective and efficient utilisation of resources. Regrettably, such models have only been described in pilot studies, and their sustainability remains unknown.
The aim of this study was to describe a model of enhanced care termed ‘recovery HDU’ which has proved sustainable over a period of ten years in a tertiary teaching hospital. Our model closely aligns with the concept of overnight intensive recovery, first described almost 20 years ago, 12 but involves anaesthesia and intensive care team co-management. This retrospective observational study reports on the characteristics, treatment, disposition at discharge and in-hospital outcomes of patients admitted to our unit over a three-year period.
Methods
Ethics
Local institutional ethics approval was sought (Austin Health Human Research Ethics Committee, 145 Studley Road, Heidelberg 3084, Australia). Approval for the study to be conducted as an audit was granted (project reference no.: Audit 20/177) on 18 January 2021.
Setting
The Austin Hospital is a 560-bed major academic teaching hospital in Melbourne, Australia. The hospital has almost 90,000 emergency department presentations, 29,000 multi-day admissions, and performs 17,000 surgeries through 11 operating theatres each year. The hospital is a state referral centre for liver transplant, spinal cord injury, complex epilepsy, thoracic aortic surgery and toxicology patients. The intensive care unit (ICU) treats approximately 2200 patients per year and had 22 beds per day on average available for patients at the time of the study.
Model of care
The recovery high dependency unit (RHD) was created in 2011 to facilitate the high burden of elective and emergency surgery in the hospital while still offering intermediate care for an increasingly ageing and complex population. 13 This RHD operates as a central combined unit with triage and admission decisions coordinated by anaesthetists and patient management, and discharge decisions overseen by ICU specialists and registrars.
The two-bed unit physically sits in a section of the operating theatres’ post-anaesthesia care unit (PACU), located on the same floor and within 30 m of the ICU. It is staffed by recovery room nursing staff at a ratio of 1:1 during daytime hours and 1:2 overnight. The increased staffing ratio during daytime hours permits flexibility with nursing staff to care for the RHD patients (1:1 for the initial period) while still assisting and maintaining patient flow through the PACU (1:2 at times of high patient throughput as well as scheduled nursing breaks). The model does not allow for more than two patients to be admitted to the RHD. Overflow of referrals is admitted directly into the ICU, although with triaging, these patients are deemed most likely to require care beyond an overnight admission.
Patients admitted to the RHD are considered to require ‘overnight’ observation and treatment, but are likely to be discharged to their reserved postoperative ward bed prior to the surgical ward rounds the following morning (i.e. before 0700 hours). Patients anticipated to require a longer period of HDU observation or support (i.e. prolonged requirement for vasopressor therapy or respiratory support) are referred directly for ICU admission at the time of morning evaluation.
RHD referrals and admissions are coordinated by the in-charge anaesthetist and include elective surgical patients with significant comorbidities identified from the pre-admission clinic, emergency surgical patients referred on the day of surgery, and patients with unanticipated intraoperative instability. There are usually four to six potential patients per day from which two patients will be admitted to the RHD postoperatively. The remaining patients are either admitted to the ICU or discharged to the ward after a period of extended (four to six hours) recovery in the PACU. The in-charge anaesthetist can ‘check in’ with the anaesthetists caring for patients earmarked for RHD during their surgery, during which time it may become apparent that RHD is no longer required. In such cases, the patient may receive extended stay in the PACU. The intensive care team is not routinely involved in these triaging and admission processes.
On admission to the RHD, the treating anaesthetist hands over the patient to the ICU medical team who are subsequently responsible for all management and patient care decisions including the suitability and timing of discharge to the ward. ICU medical staff routinely physically review the RHD patients on admission, during the evening ward round and prior to discharge, and are otherwise available on call from the main ICU. Patients who are not deemed suitable for discharge to the ward at the end of the first postoperative day are transferred to a HDU bed within the ICU for ongoing care.
This model of care runs from Monday to Saturday morning and facilitates additional intermediate level care for up to ten postoperative patients each week. Infrequently, if one of the beds is not utilised by a postoperative patient, it may be used for an acute medical patient requiring overnight HDU monitoring or observation.
Data collection
A 36-month period (July 2017 to June 2020) was audited. All adult patients (≥18 years) admitted to the RHD for at least one hour were included. Data were sourced from patient medical records and electronic databases and include demographics, hospital admission details, reason for RHD admission, APACHE-3 (Acute Physiology and Chronic Health Evaluation) scores, medical therapies instituted in the RHD (non-invasive ventilation, vasopressor therapy), post-RHD discharge destination and pre-defined in-hospital complications based on the International Classification of Diseases (ICD-10) coding (anaemia, renal failure, delirium, fall, pressure injury, wound infection). 14
Statistical analysis
Data were managed on an Excel database and analysed using R 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria). We performed standard epidemiological descriptions of the studied population by expressing medians, interquartile ranges (IQRs), percentages and ranges. Differences in proportions were assessed using the chi-square test or Fisher’s exact test. A P value less than 0.05 was taken to indicate statistical significance.
Results
Overall characteristics of the recovery high dependency unit cohort
Over the three-year period, 1257 patients were included in the study. The median age of patients admitted to the RHD was 67 (IQR 55–76) years and 59.9% were men. The median Charlson comorbidity index (CCI) was 5.0 (IQR 3.0–7.0). Patients were most commonly admitted under hepatobiliary, orthopaedics, colorectal and urology surgical units (Table 1).
Characteristics of patients admitted to the recovery high dependency unit and those discharged to the ward or the intensive care unit.
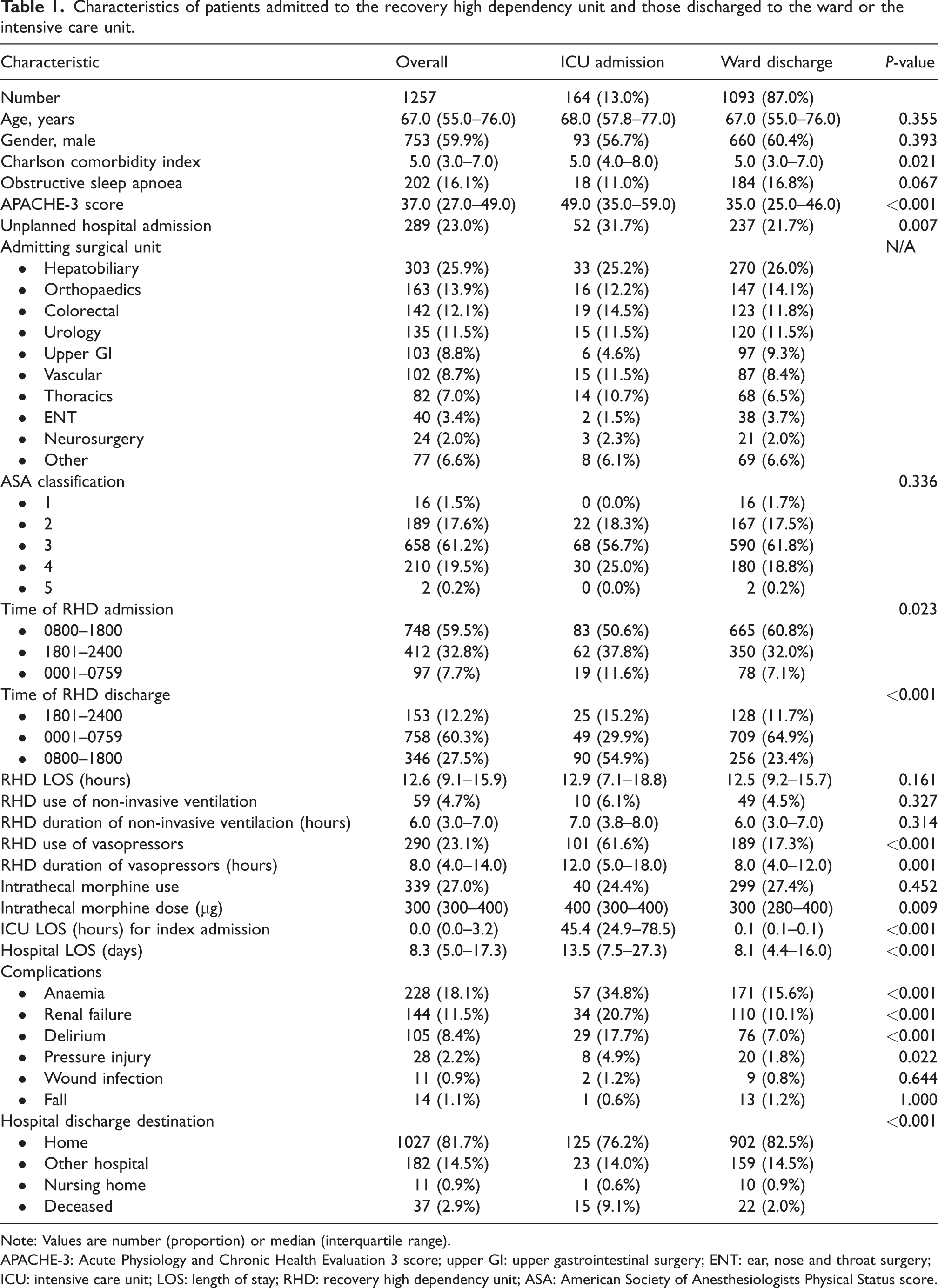
Note: Values are number (proportion) or median (interquartile range).
APACHE-3: Acute Physiology and Chronic Health Evaluation 3 score; upper GI: upper gastrointestinal surgery; ENT: ear, nose and throat surgery; ICU: intensive care unit; LOS: length of stay; RHD: recovery high dependency unit; ASA: American Society of Anesthesiologists Physical Status score.
Among the 1257 admissions, 1171 (93.2%) patients had a surgical procedure prior to admission to the RHD. A further 86 patients (6.8%) were either medical or intensive care patients admitted to the RHD from wards or the ICU due to patient overflow. Of the postoperative cohort, 277 (23.7%) patients had emergency operations, 870 (80.9%) had an American Society of Anesthesiologists (ASA) physical status class of three or more, and 339 (27.0%) received more than 200 mcg of intrathecal morphine intraoperatively. Non-invasive ventilation (NIV) was delivered to 59 (4.7%) patients mostly using their own NIV devices for pre-existing obstructive sleep apnoea, and 290 (23.1%) patients required vasopressor support.
The median length of stay in the RHD was 12.6 (IQR 9.1–15.9) hours and the median length of hospital stay was 8.3 (IQR 5.0–17.3) days. Hospital discharge data showed that 1027 (81.7%) patients were discharged home and that 37 (2.9%) patients died (Figure 1). Overall, RHD bed occupancy during the study period was 85.2%.
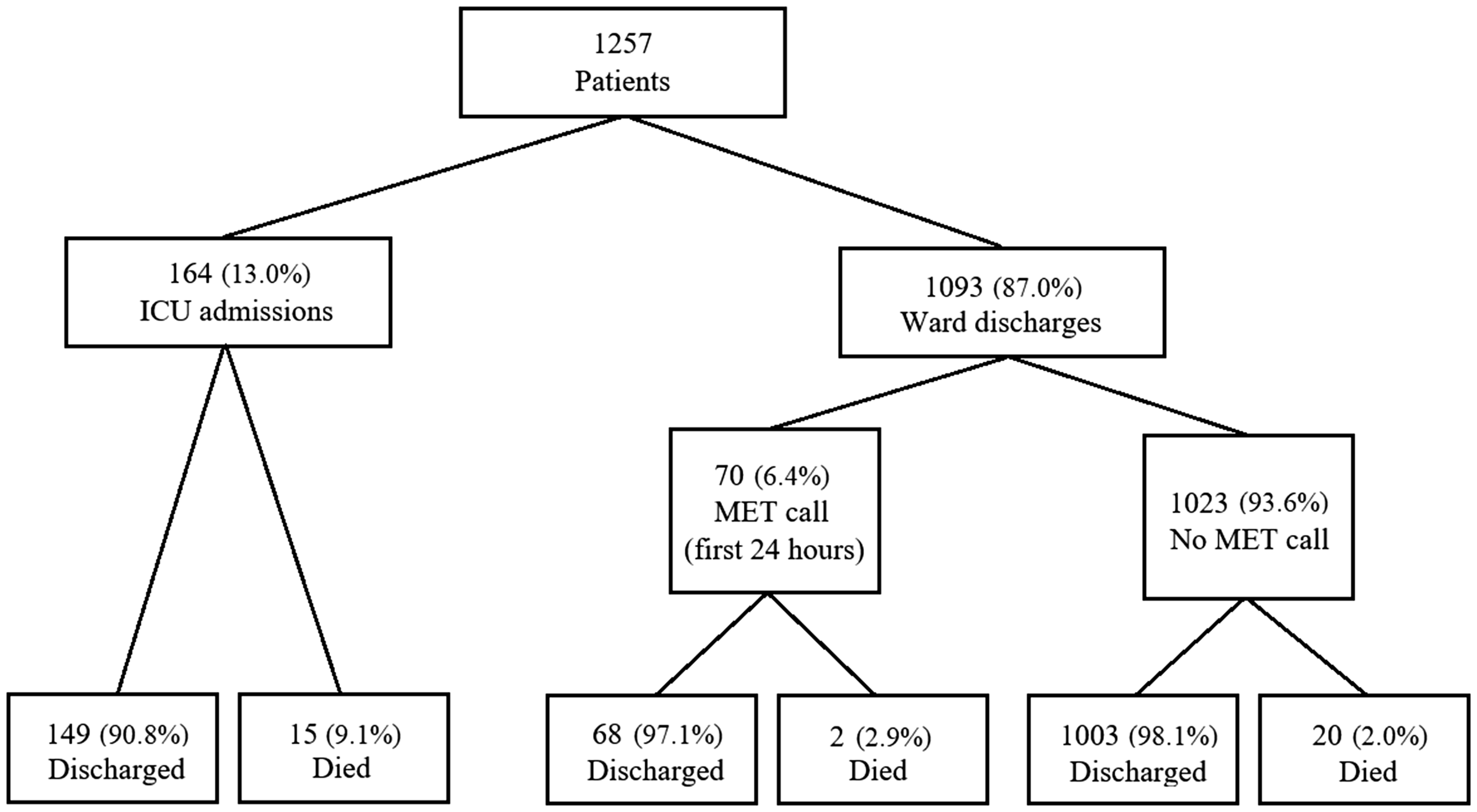
Flow diagram of all recovery high dependency unit admissions and discharge outcomes. MET: medical emergency team; ICU: intensive care unit.
There was minimal missing data in the study. The ASA physical status class was not documented for 96 patients (8.2%). No assumptions were made regarding the values of the missing data and comparisons were made on available data only.
Comparison between recovery high dependency and non recovery high dependence patients
During this three-year period, 29,537 patients had surgery with general anaesthesia and were discharged directly from the PACU to a ward. Of the 1093 RHD patients who were discharged to the ward, 1001 had surgery with general anaesthesia. The RHD cohort was older (median 67.0 versus 59.0 years, P < 0.001), had a higher CCI (median 5.0 versus 3.0, P < 0.001), longer length of operation (3.2 versus 1.3 hours, P < 0.001), longer length of hospital stay (median 8.1 versus 4.0 days, P < 0.001) and a higher rate of medical emergency team (MET) calls in the first 24 hours postoperatively (median 6.3% versus 2.2%, P < 0.001) (Table 2).
Characteristics of patients who received general anaesthesia and were admitted to the recovery high dependency unit or were discharged to the ward.
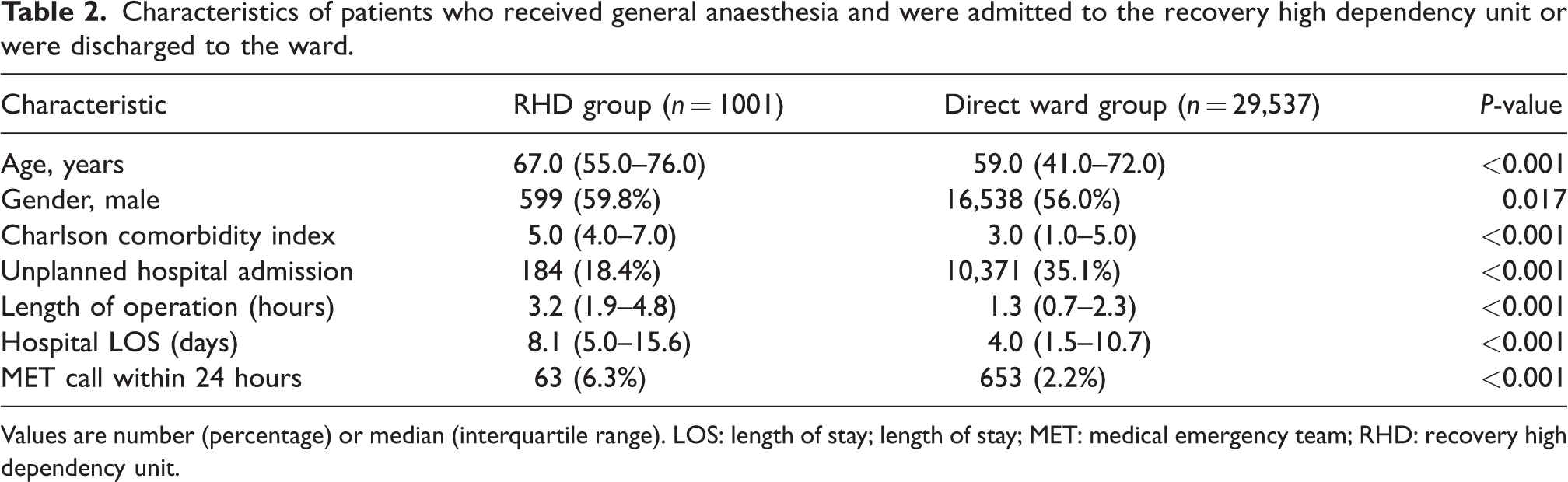
Values are number (percentage) or median (interquartile range). LOS: length of stay; length of stay; MET: medical emergency team; RHD: recovery high dependency unit.
Associations with requirement for discharge to intensive care
A total of 164 patients (13.0%) were transferred to the main ICU following their RHD admission, with the remaining 1093 patients discharged to the ward (Table 1). Of the postoperative cohort, 131 (11.2%) patients were admitted to the ICU. Patients who were admitted to the ICU had statistically significantly higher APACHE-3 scores (median 49.0 versus 35.0, P < 0.001) and were more likely to have presented as an unplanned hospital admission (median 31.7% versus 21.7%, P = 0.007). They were also more likely to be admitted to the RHD after hours (between 1800 and 0800 hours, P = 0.023) and discharged from the RHD during daytime hours (between 0800 and 1800 hours, P < 0.001).
Furthermore, patients requiring transfer to the ICU were more likely to receive vasopressors (61.6% versus 17.3%, P < 0.001) and received them for a longer duration (median 12.0 versus 8.0 hours, P = 0.001) during their RHD stay. These patients had a longer median hospital length of stay (13.5 versus 8.1 days, P < 0.001), were more likely to have in-hospital complications such as anaemia, renal failure and delirium, and were more likely to die in hospital (P < 0.001).
Associations with early medical emergency team activation
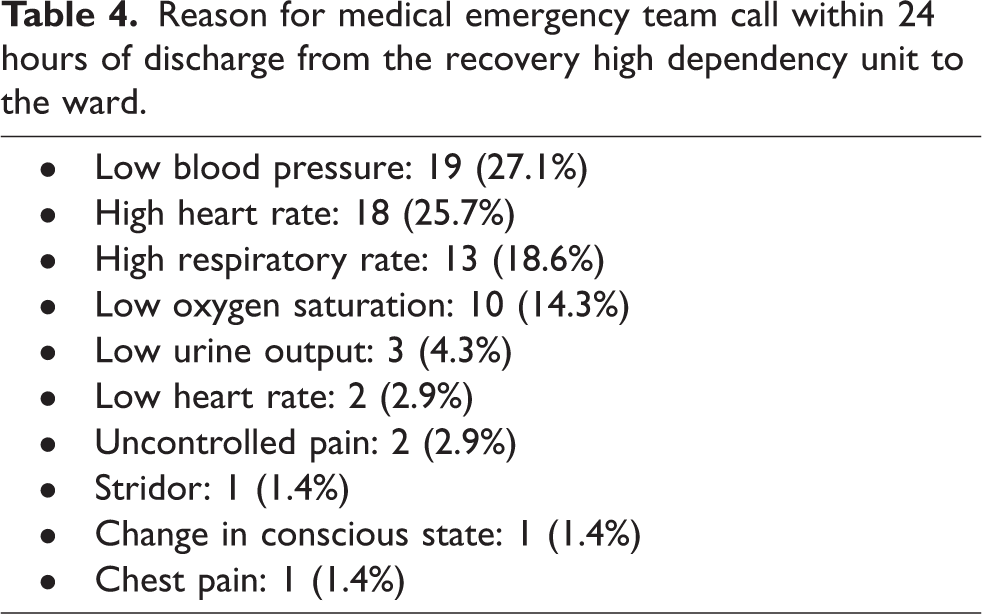
Of the 1093 patients who were discharged to the ward, 70 patients (6.4%) had a MET call within 24 hours of discharge from the RHD (Table 3). Of these patients, eight (11.4%) were admitted to the ICU following their MET call. Patients who had a MET call were likely to be older (median 73.5 versus 66.0 years, P = 0.014) and to have required non-invasive ventilation in the RHD (11.4% versus 4.0%, P = 0.010). Patients who had a MET call also had a significantly longer median hospital length of stay (11.7 versus 7.8 days, P < 0.001) and were less likely to be discharged home (P = 0.026). The most common reasons for MET activation were hypotension (27.1%), tachycardia (25.7%), tachypnoea (18.6%) and hypoxia (14.3%) (Table 4).
Characteristics of patients discharged from the recovery high dependency unit to the ward according to medical emergency team activation.
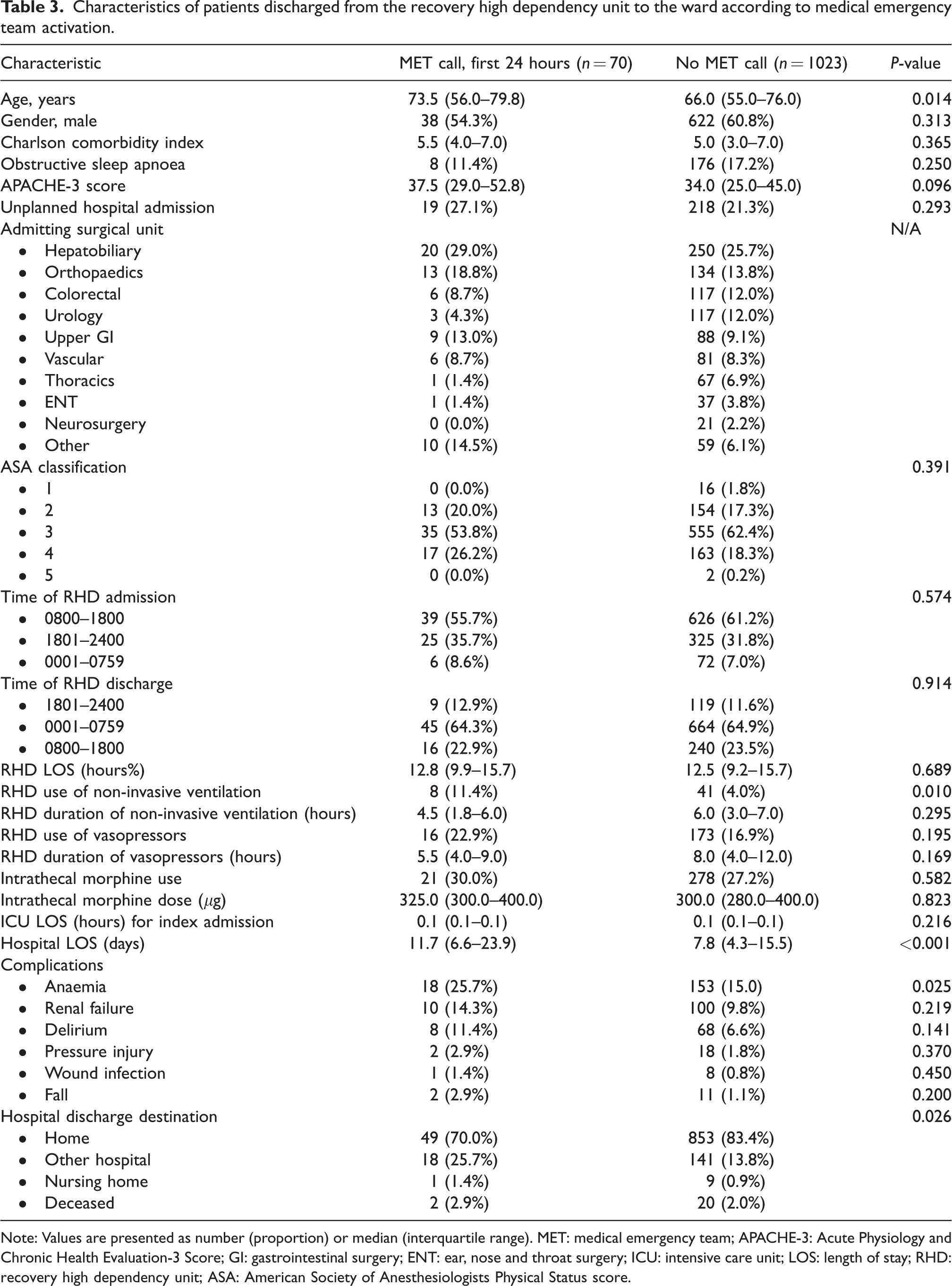
Note: Values are presented as number (proportion) or median (interquartile range). MET: medical emergency team; APACHE-3: Acute Physiology and Chronic Health Evaluation-3 Score; GI: gastrointestinal surgery; ENT: ear, nose and throat surgery; ICU: intensive care unit; LOS: length of stay; RHD: recovery high dependency unit; ASA: American Society of Anesthesiologists Physical Status score.
Reason for medical emergency team call within 24 hours of discharge from the recovery high dependency unit to the ward.
Discussion
This retrospective observational study of our RHD showed that we were able to admit an additional 1257 patients over three years for overnight intensive care support outside of our ICU bed capacity. This model permitted almost 5% of patients to receive non-invasive ventilation, almost a quarter to receive a sustained period of vasopressor support and a quarter to receive high-dose intrathecal morphine with close postoperative cardiorespiratory monitoring. More than 80% of this cohort had an ASA physical status score of 3 or more indicating moderate to severe systemic disease that results in some functional limitation. They were also significantly older, had more comorbidities and had longer operations than the general surgical population admitted directly to the ward postoperatively. Despite this, less than one in eight required ICU admission following their RHD stay and, of those discharged to the ward, one in 16 triggered a MET call in their first 24 hours post-discharge. Despite their comorbidities and intensity of treatment, overall mortality was less than 3%.
Comparison with previous studies
Our data compare favourably with a recent interventional study assessing the effect of extended recovery room care in moderate risk surgical patients. 8 Our patient cohort was slightly younger and a higher proportion had elective surgery (76% versus 66%), but a similar proportion had an ASA physical status class of 3 or more. Our patient cohort had a higher ICU admission rate (13% versus 8%) but a lower proportion of MET activations if discharged to the ward (6% versus 12%) and shorter hospital length of stay (8.3 versus 9.2–10.9 days). Our patient outcomes were also comparable with previous studies of overnight intensive recovery models of care with regard to ASA physical status scores, ICU admission rates, hospital length of stay and mortality.15–17 A previous study has suggested that intensivist-led PACU care may increase surgical throughput and reduce short-term patient admissions to the ICU. 18 Our findings are aligned with this concept. Our ICU co-led model also allows for medical patient admissions at times of high acuity and ICU overflow, although such events occurred less than once per week.
Implications for clinicians and policy makers
Our findings suggest that an overnight intensive recovery model as an adjunctive strategy to reduce ICU bed demand provides flexibility for surgical patient triage, extends recovery room nurses’ scope of practice and increases surgical throughput. Moreover, they suggest that co-management by anaesthesia and intensive care teams allows the anaesthesia team to triage patients effectively with full overview of all theatre cases for the day, and allows facilitation of postoperative management by the intensive care team, smoother transition to ICU admission for patients requiring ongoing support, and earlier identification of patients who require post-discharge support on the ward by the critical care outreach team. Finally, they suggest that this model supports the safe and efficient delivery of care to patients who may be too vulnerable for surgical ward transfer after their initial stay in the PACU.
Strengths and limitations
To our knowledge, this is the largest published study of patient characteristics and outcomes of an overnight intensive recovery model. Our cohort of patients had a median length of RHD stay of 12 hours. We also identified characteristics of patients who were more likely to require ICU admission and were more susceptible to MET calls post-discharge. Our patient cohort had similar acuity to those in contemporaneous studies. Our model of care has been shown to be satisfactory with low overall ICU admissions, low post-discharge morbidity and mortality, and has proved sustainable over ten years.
The limitations of this study are its retrospective methodology and single-centre nature. We were unable to collect data on the total number of patients triaged for the RHD. A proportion of these patients would either be discharged to the ward postoperatively or admitted to the ICU, and their outcomes in comparison to the RHD cohort would be of interest. Finally, the cost benefit of this model, its impact on surgical throughput and ICU bed demand is unclear. Although we did not analyse cost-effectiveness, this model allowed us to care for an additional 419 patients per year outside of our ICU bed capacity. Further prospective evaluation and comparison of characteristics and outcomes of RHD patients with those referred but not admitted to the RHD is planned.
Conclusion
In this retrospective observational study of an RHD patient cohort, there was a relatively low need for ICU admission postoperatively and a very low incidence of MET calls post-discharge to the ward. This model of care has proved to be very safe and sustainable as a co-managed anaesthesia and intensive care service. Other institutions may consider the introduction and evaluation of this model in the care of their higher-risk surgical patients.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank Dr Luke Fletcher for his assistance with the study.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.