
Abstract
The introduction of anaesthesia on 16 October 1846 brought about tremendous changes in the discipline of surgery. We sought to determine whether the concept of painless surgery was accepted by practitioners and patients, and whether this led to an increase in frequency and variety of surgical operations performed. To study these changes, we analysed surgical records from Massachusetts General Hospital, Boston, Massachusetts (MGH) in the months surrounding the discovery of ether anaesthesia. Surgical records from MGH between 25 February 1846 and 14 March 1847 were examined, and the variables studied included number of operations, type of operations, patient demographics, complications and analgesics used, as well as comments made by surgeons. Immediately following the introduction of anaesthesia, MGH experienced a sizeable increase in the volume of surgical operations. This included a doubling in the percentage of female patients undergoing surgery. Orthopaedic procedures and amputations both increased in frequency, as did the number of surgeons operating. Several records indicated the presence of postoperative wound infection. Operations were still performed without anaesthesia. Following the introduction of ether anaesthesia in 1846, surgical volume increased, and more women underwent surgery. This suggests early acceptance of anaesthesia by patients and the medical profession. In an era prior to the introduction of antiseptic and aseptic techniques it is not surprising that wound infections were observed in several patients. We provide a glimpse of anaesthesia and surgery during the first few months after the first public demonstration of anaesthesia at MGH.
Keywords
Introduction
Prior to the introduction of anaesthesia
In the period prior to what is now known and celebrated as Ether Day (16 October 1846), surgery was a limited and somewhat barbaric profession. Conscious patients underwent unimaginable pain during operations.
1
The unfortunate reality that faced both surgeons and patients was that in some instances, surgery was often greatly beneficial or even necessary.
2
George Hayward (1791–1863), a surgeon at Massachusetts General Hospital (MGH), was quite familiar with weighing the pros and cons of operating. In an article published in The Boston Medical and Surgical Journal (8 July 1840), he described this predicament as it pertained to amputations at MGH in the era prior to anaesthesia: While it is no doubt true that amputation is sometimes too long delayed, it is equally certain that it is often performed when it might have been avoided. It is difficult in many cases to decide on the best course, but the operation should not be done without the clearest evidence of its necessity, for it is a hazardous and painful one, and, even when perfectly successful, leaves the patient in a mutilated state. The [patient’s] head being firmly supported by two assistants, the incision was commenced between the eyebrows, and the flap of skin dissected up so as entirely to isolate it from the skin of the forehead … The knife was also passed between the lip and upper jaw … and the adhesions between the two, for the space of an inch, entirely cut away. The horror of great darkness, and the sense of desertion by God and man, bordering close on despair, which swept through my mind and overwhelmed my heart, I can never forget, however gladly I would do so … I still recall with unwelcome vividness the spreading out of the instruments: the twisting of the tourniquet: the first incision: the fingering of the sawed bone: the sponge pressed on the flap: the tying of the blood-vessels: the stitching of the skin: the bloody dismembered limb lying on the floor.
Ether Day
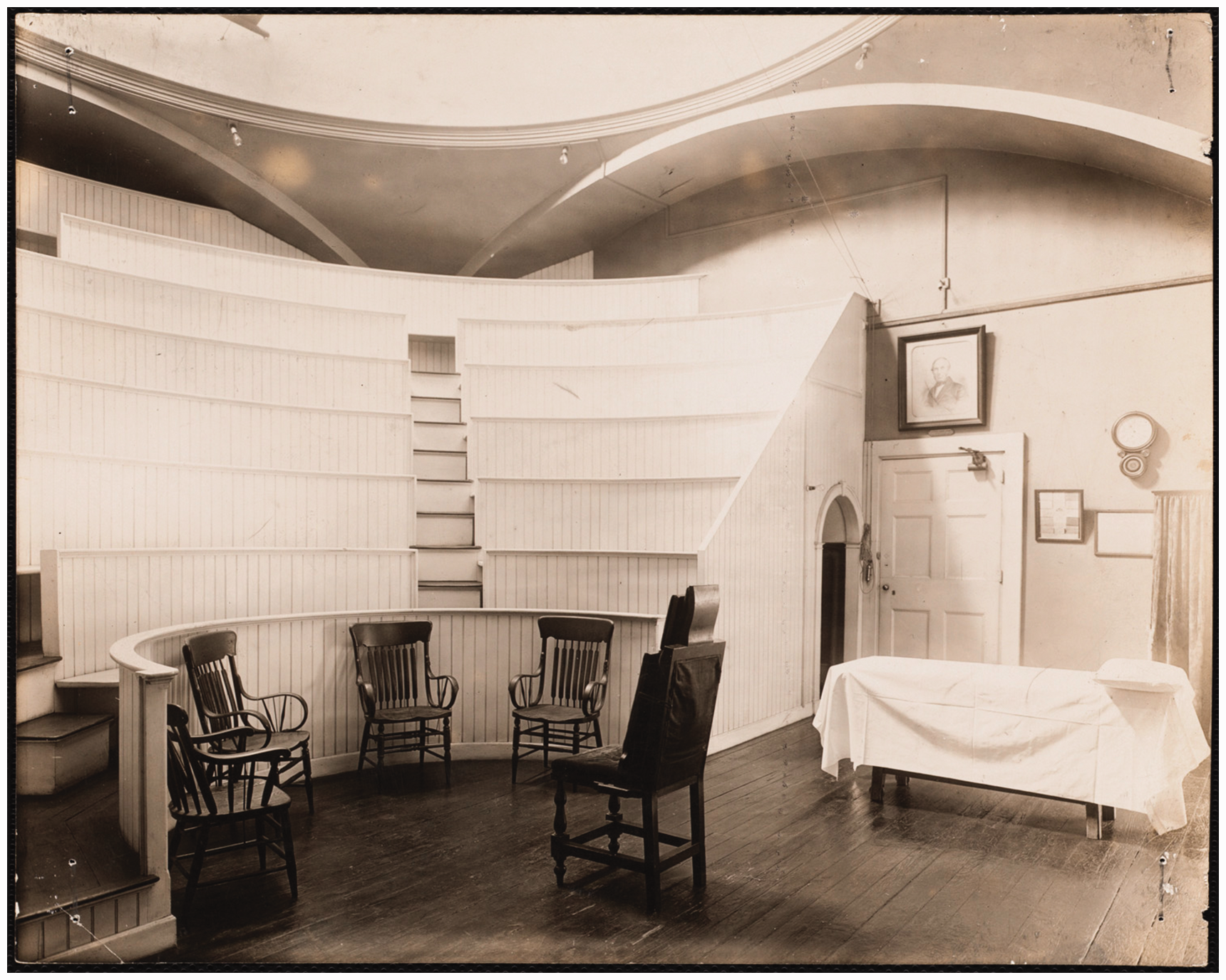
On 16 October 1846, a medical student by the name of William TG Morton (1819–1868) (Figure 1) demonstrated to the world one of the greatest medical discoveries to date. Morton did not graduate from medical or dental school. He served as an apprentice to Horace Wells (1815–1848) and even practised dentistry on his own. He then attended Harvard Medical School, but did not complete his studies. He was awarded an honorary MD degree in 1852 by the Washington University of Medicine, later known as the College of Physicians and Surgeons of Baltimore. 7 Morton had proved successful in performing painless tooth extractions in patients who inhaled ether before their procedures, and now hoped to demonstrate this finding to the medical world in the operating theatre of MGH (Figure 2). 8 His anaesthetic would be put to the test during an operation performed by John Collins Warren (1778–1856) that involved the removal of a tumour from the neck of 20-year-old Edward Gilbert Abbott (1825–1855). 9 Apart from the inhaled ether, there were no other analgesics given to Abbott prior to surgery.
During the operation, the patient remained in a semiconscious state, muttering occasionally. Upon waking, Abbott reported the pain to be considerably mitigated, as though his skin was being scratched. 10 Warren celebrated the successful demonstration, turning to those in attendance and reportedly decreeing, ‘Gentlemen, this is no humbug.’ 11 And so, general anaesthesia was introduced to the field of surgery. The word ‘humbug’ was supposedly used in reference to an earlier attempt by Wells in the previous year to conduct a painless tooth extraction under the influence of nitrous oxide. The patient cried out during the procedure and the entire demonstration was deemed a failure. 12 Although the patient later claimed to have no recollection of pain, the damage was done, and the entire incident dismissed as ‘humbug’.
The overall impact of Morton’s demonstration cannot be overstated. Upon Morton’s death in New York City, the chief surgeon at St. Luke’s Hospital in New York City announced, ‘Gentlemen, you see lying before you a man who has done more for humanity and the relief of suffering than any man who has ever lived.’
13
At his final resting place in Mount Auburn Cemetery of Cambridge, Massachusetts, Morton’s tombstone reads: Inventor and Revealer of Anesthetic Inhalation: Before Whom in all time, Surgery was Agony; By Whom Pain in Surgery was Averted and Annulled; Since Whom, Science has control of Pain.
14
Methods
We examined 40 surgical records from MGH between 25 February 1846 and 14 March 1847 to study changes brought about by the introduction of ether anaesthesia and determine the overall initial impact of this discovery on surgical practices at MGH. These records are held in the Francis A. Countway Library of Medicine and the archives of MGH in Boston. This analysis covers 11 operations performed prior to Ether Day, the famous Ether Day operation itself and 28 operations performed after the first public demonstration of ether.
Results
We were able to access 40 surgical records that spanned the period from 25 February 1846 to 14 March 1847. Of these, 11 procedures were performed prior to the advent of ether anaesthesia on 16 October 1846 and 28 procedures performed after it. This increase in surgical volume from roughly 1.6 surgical procedures a month in the period before Ether Day to 5.6 surgical procedures in the months following the demonstration reflects a 250% change.
Only two out of the 11 operations in the seven-month period leading up to Ether Day were performed on women. Of the 28 procedures after Ether Day, ten (36%) were performed on women, reflecting a 100% increase in operations on female patients.
The age of patients undergoing surgery did not appear to change during this period surrounding the first use of anaesthesia. Median age in the 11 cases before Ether Day was 35 years, compared with a median age of 30 years after the demonstration (P = 0.09; not significant (NS)).
After the demonstration of inhalational anaesthesia, the number of surgeons performing operations at MGH increased. In the seven-month period leading up to Ether Day, only three surgeons are mentioned in the records. Alfred Lambert (1822–1885) performed one procedure, while Solomon D Townsend (1793–1869) and John Collins Warren performed five each. In the roughly five months after the public ether demonstration, a few other surgeons appeared on the records. Warren and Townsend continued to operate regularly and were accompanied by Henry J Bigelow (1818–1890), George Hayward (1791–1863) and Samuel Parkman (1816–1864). Hayward (n = 9) and Warren (n = 9) performed the most operations, followed by Townsend (n = 5), Parkman (n = 3) and Bigelow (n = 1). Two records do not list the surgeon. One record lists both Hayward and Warren as surgeons.
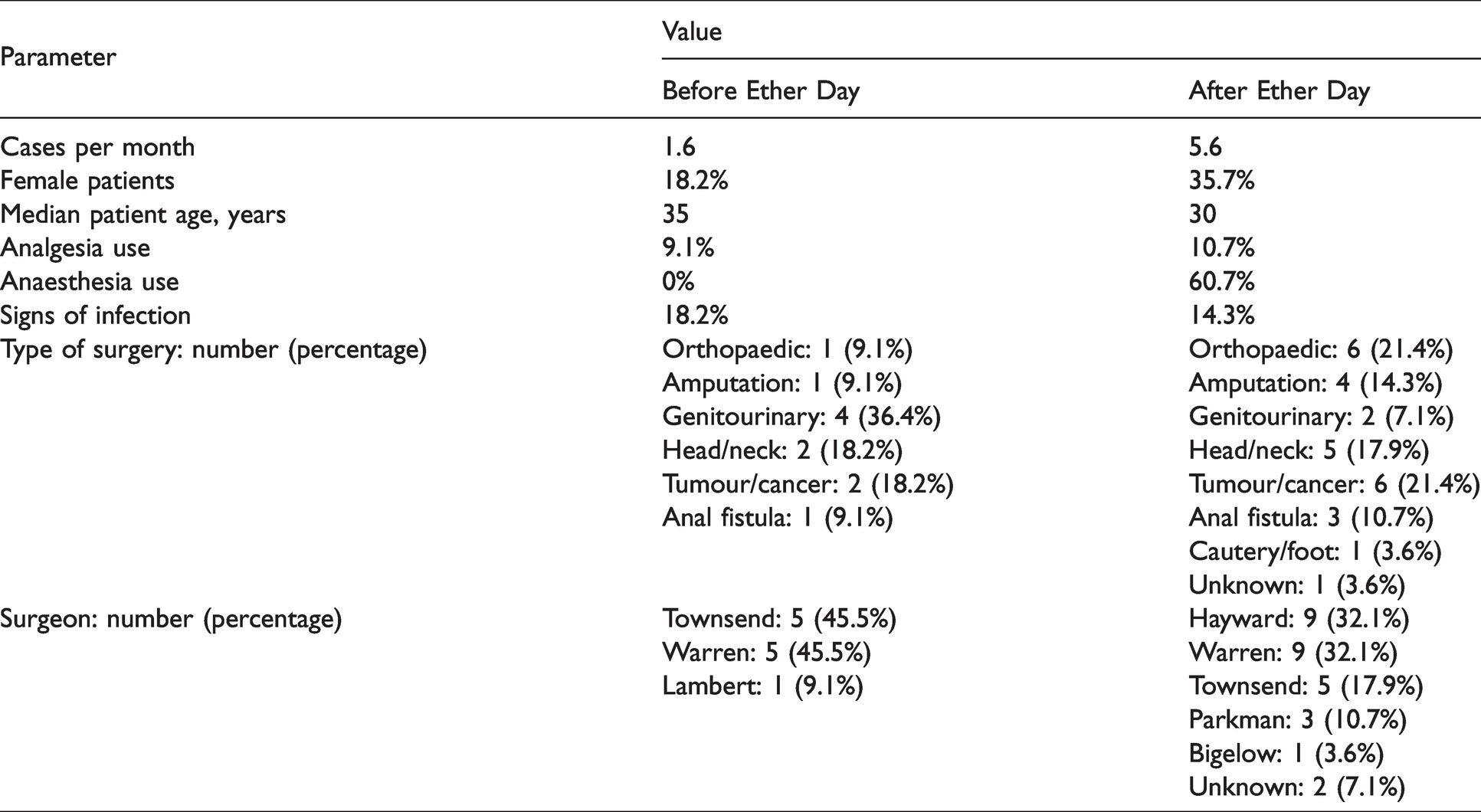
Table 1 shows the different types of surgical procedures performed at MGH during the months surrounding Ether Day. While genitourinary operations accounted for the largest percentage (36.4%) of procedures before Ether Day, only two (7.1%) genitourinary operations were performed in the five months following Ether Day. This decrease was made up by an increase in the percentage of amputations and orthopaedic procedures. Other surgical procedures were performed at a similar rate before and after Ether Day.
Variables recorded in the surgical records surrounding Ether Day.
Intraoperative analgesics are known to have been in use prior to the introduction of general anaesthetics. In the MGH records analysed here, one case prior to Ether Day lists the use of opium to help manage patient pain during a procedure involving the removal of urinary stones. ‘Opium’ and ‘laudanum-opium’ are documented analgesics used in three of the cases that took place after Morton’s ether demonstration. One of these three procedures involved the removal of a bone spur from the humerus and was performed without the use of ether. The other two uses of intraoperative analgesia after Ether Day were given in concert with general anaesthesia. One of these two patients underwent a mid-thigh amputation, and the other underwent removal of a carcinoma of the mandible. One of 11 patients received intraoperative analgesics before Ether Day, while three of 28 did so after Ether Day. Of these three patients, one underwent surgery without anaesthesia. It is possible that information about the use of intraoperative analgesics is incomplete or recorded in documents other than the surgical records.
Of the 28 operations performed after Ether Day, 17 records document the use of general anaesthesia with references about the use of ‘ether’ and ‘sulfuric ether’, or ‘aether’ to anaesthetise the patient. Eleven of the 28 operations were performed without general anaesthesia, despite Morton’s demonstration. The surgeons for these cases are as follows: Warren (three), Hayward (three), Townsend (two), Bigelow (one) and unknown (two). Vital signs were not recorded in any of the 40 records analysed. Length of the procedure was documented in six of the 40 records (range: 5 min to 4 h; median: 2 h; average: 2 h and 3 min).
While all 40 patients survived the surgical procedure, six showed signs of postoperative infection. Prior to Ether Day, two out of the 11 (∼18%) patients exhibited signs of infection, while four out of 28 (∼14%) did so after Ether Day. As expected, the use of ether did not initially influence the rate of postoperative infection (χ2 = 0.76; NS)
Additional comments
Most of the surgical records contain additional information not discussed above. These generally include various findings deemed noteworthy by the surgeon. After Ether Day, a handful of records describe how patients tolerated general anaesthesia, or whether a procedure was performed without ether.
On 16 November 1846, Townsend performed a below knee amputation on a 35-year-old male who presented with a comminuted fracture of his left lower leg. It is interesting that even one month after Ether Day, the patient underwent this procedure without ether or analgesia. Townsend’s notes from this record depict the psychological trauma associated with operations performed on conscious patients. He describes one patient yelling and thrashing about after an operation, and that he was restrained in a straitjacket to be worn through the following day. Two days later, ether was administered to this patient to help him relax and return to a more stable demeanour. Townsend also noted that this patient was given morphine regularly during recovery.
Hayward provided quite a different commentary on a procedure that took place on 4 December 1846. With the assistance of Morton as the anaesthetist, Hayward performed the removal of a tumour from the left breast of a 55-year-old female patient. The operation took place with the use of ‘sulfuric ether’ as the general anaesthetic. No additional analgesic was administered. Hayward describes the patient as struggling during the procedure, but ultimately not remembering anything afterwards.
Other records note similar experiences regarding patient response to ether as a general anaesthetic. In a surgical record from 12 December 1846, Warren comments that his patient was in great spirits throughout the procedure and felt like nothing had been done to her at all. Morton is again listed as the anaesthetist who provided ‘sulfuric ether’ to the 58-year-old woman during an operation that involved the removal of a malignant dysplasia of her upper jaw. The record does not mention the use of any additional drug to control pain.
Ten days later, on 22 December 1846, Parkman describes a reduction of a dislocated humerus that was performed under ‘aether’. No anaesthetist is documented in the records, but Parkman does note that the patient, a 58-year-old woman, remained completely unconscious throughout the whole procedure. A little over a week later (2 January 1847), Townsend also documented a 42-year-old female patient who was completely unconscious through her operation. The patient was given ‘aether’ prior to the amputation of her leg and was noted by Townsend to ‘not remember anything of the operation’.
On 2 January 1847 Hayward operated on a 27-year-old man suffering from fistula-in-ano. Hayward wrote that the patient, who was initially ‘excited’ during the ether inhalation, did not completely lose consciousness during the operation. He added that although the patient called out incomprehensible complaints during the procedure, he did not recall pain or experience any postoperative complication.
A record dated 9 January 1847 describes Hayward performing an amputation of the foot on a 50-year-old female patient. It is noted that the patient ‘suffered from spasm and some level of asphyxia during the inhalation of ether prior to surgery’. No additional details are mentioned but this appears to be the first record of an anaesthetic complication at MGH.
This less than desirable outcome was not repeated in Hayward’s next case. On 19 January 1847, a 27-year-old female patient was scheduled for the removal of a labial tumour the size of a ‘hen’s egg’. She was given ‘sulfuric ether’ prior to surgery and ‘reported pleasant dreams throughout the procedure’; a great improvement from what had happened to the previous patient.
Discussion
The introduction of anaesthesia was an essential prerequisite for the development of the discipline of surgery. Surgery could now be offered as a pain-free procedure to patients. Surgeons were able to prioritise precision over speed.15,17,18 More diseases and conditions could be treated surgically. 19 This analysis of 40 surgical records surrounding the 16 October 1846 demonstration provides insight on the initial changes in surgery at MGH in the mid-19th century.
One would expect surgical volume to increase with the introduction of anaesthesia. We note a 250% increase, but the numbers are small and likely reflect several concomitant phenomena. The introduction of ether anaesthesia was closely followed by an increase in the rate of surgery among admitted patients at MGH. The rise appeared to be the greatest among women, the elderly, the native-born, non-labourers and amputees, all of whom received anaesthetics most frequently. Following the ether demonstration, the rate of surgery for men admitted to MGH doubled and the rate in women more than tripled. 20
Along with an increase in surgical volume, the records show an increase in the number of surgeons performing operations at MGH after Ether Day. This increase is likely due in part to the advent of anaesthesia, as there is no evidence to suggest that the hospital expanded its medical staff for other reasons. It is important to note that while the records first show Hayward, Parkman and Bigelow operating after Ether Day, two of these surgeons were already in practice. Hayward was a visiting surgeon at MGH from 1823 to 1851 and even headed the surgical department for a year from 1837 to 1838. 21 Parkman is listed as a visiting surgeon during the period of 1845–1854. Bigelow was officially appointed one of the surgeons of MGH in the year 1847. 22
Although the concept and application of anaesthesia had been successfully demonstrated, there were not many individuals available to administer anaesthesia. Morton was not even certain of the outcome of his demonstration. He had not disclosed the identity of the potion he had used and little information existed about equipment needed to administer ether. Surgery was a nascent discipline with only a limited number of conditions requiring the expertise of surgeons. It would take a few years before surgeons could attempt more complex surgical operations. Most procedures were carried out in desperation, and in conditions that were either neglected or in urgent need of intervention. Furthermore, prior to the introduction of antisepsis and antibiotics, surgical procedures were primarily carried out on extremities or on superficial structures. Surgical outcomes were poor, and Morton’s patient who survived Ether Day needed six weeks to recover from the operation.
The median age of patients remained essentially unchanged after Ether Day. Children were noted early on to be at a higher risk of complications linked to anaesthesia. 23 Morton stopped administering ether to children after he observed that younger patients were more likely to suffer from nausea and vomiting after surgery. 24 This complication was associated with significant morbidity and mortality. 25 While physician anaesthesiologists were still many decades away, 26 Morton is recognised as the first recorded anaesthetist at MGH, evident on Warren’s surgical record from 16 October 1846. Four other records in this period list Morton as the anaesthetist on the case. There are no other anaesthetists listed on the records during this period.
Amputations and orthopaedic cases increased in frequency. Opium, a drug with a well-documented history in pain relief at the time, 27 was used infrequently both with or without ether to aid in pain management. With the introduction of anaesthesia, it may not have occurred to surgeons that the patient would require postoperative analgesia. Ether was a long-acting anaesthetic and operating room records may not have included comments about analgesics that may have been administered several hours later. Apart from opium, ‘warm water’ and ‘castor oil’ were the only medications mentioned in operations carried out after Ether Day.
Although information about the discovery of the analgesic and anaesthetic properties of ether and nitrous oxide spread quickly across the world, it is not known how rapidly these were included in routine surgical care. Quantitative data from the United States, Europe or other parts of the world is not available but ether and chloroform were commonly used within one to two years after the demonstration of 1846.
The earliest use of anaesthesia records was introduced about 50 years later, and vital signs were not recorded in any of the documents. Harvey Cushing (1869–1939) and Ernest Codman (1869–1940) would become the pioneers of the anaesthesia record in the late 19th century while medical students at Harvard Medical School. 28 Their records documented vital signs and many details about the patient and the operation.
Infection remained a major barrier in surgical treatment. 16 Antiseptic techniques were introduced in the 1860s and it was decades before they were employed routinely in the operating room. 29 As a result, infection rates remained high during the period of early anaesthesia.
Recognising the importance of the discovery of anaesthesia, many of the surgeons at MGH took care to note their patients’ reactions to ether inhalation. These records provide the first glimpse into the efficacy of ether as a general anaesthetic. They highlight the stark contrast between the psychologic state of patients undergoing major procedures with and without anaesthesia. The image of a screaming man forcibly restrained in a straitjacket is replaced by a woman in a pleasant, ether-induced dream, who will awaken without pain or recollection of her operation.
Conclusions
We have shown that the introduction of anaesthesia at MGH was accompanied by an increase in surgical volume and increase in the number of surgical staff performing operations. We cannot explain why a greater percentage of women underwent surgical operations during these early months. The small number of operations performed during this period limits our ability to comment on a discipline that would undergo dramatic changes over the ensuing decades. Pain-free surgical procedures encouraged physicians to consider surgery as a career option, and the demand for anaesthesia providers prompted surgeons to train nurses to provide anaesthetic care. It was not until the 20th century that physicians considered a full-time career as an anaesthesiologist, a process greatly facilitated by the Great War and subsequent conflicts. Antiseptic and aseptic surgical techniques in the 1870s constituted the next great advance in surgery. The primary source documents used in our investigation provide a rare glimpse of the early evolution of anaesthesia and surgery in the third-oldest hospital in America.
William TG Morton (1819–1868).
11
The Ether Dome. Photograph c. early 1900s. The surgical amphitheatre in Massachusetts General Hospital arranged as it was when the first ether operation was performed.
Footnotes
Author Contribution(s)
Acknowledgement
The authors of this paper would like to thank the staff at the Francis A. Countway Library of Medicine and the archives of Massachusetts General Hospital in Boston for providing us with access to the surgical records analysed in this study.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the University of Massachusetts Chan Medical School Research and Curriculum Exploration summer program.