
Abstract
The psychological impact (second victim effect) of in-theatre critical incidents is increasingly recognised. Different styles of psychological support programme have recently been published, including some utilising ‘near in time’ peer support. Most of these programmes either target their support to individuals, or focus on one vocational group rather than the multidisciplinary team. However, the in-theatre team consists of different craft groups who nonetheless function as a single team and are therefore ‘peers’. This paper sets out the design and implementation of a critical incident peer response programme at Waikato Hospital, New Zealand, which provides peer-led group psychological first aid to full theatre teams. The programme is administered by trained representatives from multiple in-theatre craft groups including nurses, midwives, anaesthetic technicians, recovery room nurses, surgeons and anaesthetists. It emphasises team education and peer support, and has a wholly welfare focus. The programme has voluntary participation but mandatory activation triggers so that individuals do not need to seek support actively at a time when they may not recognise the need to do so. The programme is becoming embedded in the Waikato Hospital theatre culture so that participating in psychological support is normalised following a critical event. This framework is shared in the hope that it will assist other hospitals to develop welfare interventions to support full theatre teams.
Keywords
Introduction
Most anaesthetists will be involved in several critical incidents through their career, starting during their anaesthetic training, 1 with a cumulative deleterious effect on their mental health and clinical functioning.1 –4
A critical incident is any significant event in the workplace that threatens to overwhelm the coping mechanisms of the staff members involved, with the potential to produce strong emotions, thoughts or behaviours that may result in the inability to function normally.5,6
Critical incidents are not specific to healthcare, but many examples can be seen in the work of healthcare providers. In the operating theatres, critical incidents are often challenging and distressing cases that involve unexpectedly poor outcomes for patients. In this way, they may appear similar to a ‘clinical incident’ (in which a patient suffers unintended harm during the provision of healthcare). However, patient harm and clinician error are not prerequisites for a critical incident. Other examples of critical incidents include serious injury or death of a colleague in the workplace, multicasualty incidents, known victims/patients, events involving children, and events with excessive media interest.1,6,7 Like the critical incidents that affect first responders and other emergency workers, these events occur in an occupational setting, as an expected part of usual work,3,8,9 which may lead people to minimise or underestimate their psychological impact. 10
The impact of a critical incident varies between people despite experiencing the same event, and will vary within an individual for different events. A critical incident may cause positive motivating stress (eustress) for some. For others the result may be debilitating distress. Myriad factors for an individual and a team will influence the response.1,3,5,8 A support system that gives individuals autonomy and an active role in developing their own recovery pathway is thus fitting to reflect these differing responses. 11
The impact of cumulative stressors in healthcare workers is evident,4,7,9,10,12,13 with high rates of burnout and suicide especially among anaesthetists. 3 Absenteeism, substance use, and relationship breakdown have all been attributed to work stress in emergency service workers.11,13
Our workplace, Waikato Hospital, is a tertiary referral centre with 30 operating theatres and out-of-theatre anaesthetising locations. It is a level one trauma centre, receiving trauma from the central North Island of New Zealand, and offers cardiac, neurosurgical, paediatric, and obstetric services on a single site. With over 25,000 cases per year in this complex setting, there are many clinical situations that generate critical incidents.
The impact of these events on staff had been recognised by theatre management, with the suggestion that theatre staff turnover was amplified by work stressors, consistent with the literature.8,12 The authors, who have experience delivering group ‘debriefing’ conversations as an educational tool after simulated crises, were increasingly asked to offer psychological debriefs after real-life crises in the operating theatre, both by staff and by management. The frequency of these requests, and the growing evidence base reflecting harm to those involved in providing care during critical incidents (second victims)4,5,10,11,13 made the need for a welfare intervention apparent. When the authors proposed a formal process for the support of teams after critical incidents, with appropriate training of facilitators, they received quick support from the relevant executive groups.
As a result, a multidisciplinary peer support intervention was implemented in the Waikato Hospital operating theatres to address these welfare needs. This paper describes the design and implementation of that peer support service, and reports on its first three years of operation. This framework is shared in the hope that it will assist other hospitals to develop welfare interventions to support full theatre teams.
Service design
The starting framework chosen for delivery of this service was critical incident stress management (CISM) due to the availability of a New Zealand-based training course using this method. 14 CISM is a multicomponent approach to welfare after critical incidents.5,11 The main interventions in this system are the ‘defuse’ and the ‘debrief’, 5 although the same or similar interventions occur under a range of names and terms. The CISM defuse is also called ‘immediate small group support’, 15 and is almost indistinguishable from group psychological first aid (PFA) interventions;16,17 the CISM debrief is also called ‘powerful event group support’ and critical incident stress debriefing (CISD). 15 These interventions have been used by the United Nations, World Health Organization, and by sovereign military units in war zones and humanitarian environments.18 –21 There are numerous examples of the approach in healthcare,2,10 and the recently published Australian and New Zealand College of Anaesthetists critical incident debriefing report endorses peer welfare support in this occupational setting through a CISM lens. 22
The differing terminology in use for these types of welfare interventions does make interpretation of the evidence difficult; many studies use the term ‘debriefing’ but mean myriad different approaches.11,20,23 –25 In the CISM framework, defuse and debrief are group interventions with a specific structure, length, timing and follow-up, delivered by trained individuals, and specifically intended for key occupational groups who experience critical incidents in their work environment.11,23 The literature clearly highlights the importance of these design factors for ensuring safety11,16,17,20,23,26 (see Table 1).
Key points for delivering critical incident stress managment interventions safely.

In terms of outcome, the evidence base suggests that this type of intervention may not reduce rates of post-traumatic stress disorder (PTSD),19,25 –27 but does have positive effects on absenteeism and distress, 19 with accelerated return to normal function, lower levels of alcohol use, and higher self-rated quality of life all reported in key occupational groups.7,26 It is suggested that one of the benefits of this type of intervention is meeting needs by engaging the protective effects of team camaraderie. 26 The limited data in the anaesthetic literature suggest that anaesthetic trainees who receive debriefings after critical incidents are more likely to feel supported by their senior colleagues, 1 and that to reduce the harm to members of our profession, departments need protocols that include this type of intervention after a critical incident.28,29
Despite this evidence of specific benefits in occupational groups, the overall effects of this approach, particularly ‘debriefing’ (CISD) have been debated.11,19,20,25 –27 Much of this debate stems from the use of CISD outside of its intended environment, and without application of the safety requirements stated in Table 1.20,23,25 Nevertheless, the published concerns regarding the safety of CISD have led to a reduction in its use. The subsequent void in psychological support interventions has resulted in the development and use of PFA,10,11,16,17,30 with growing evidence in support of this approach, both for individuals and for occupational groups.10,11,16,17 A 2010 New Zealand-based review of debriefing as part of CISM recommends that contemporaneous, practical peer-led support of some form should continue to be offered to at-risk occupational groups despite a lack of evidence of positive outcomes of debriefing in civilians and ‘primary victims’. 11
We have developed a critical incident peer response (CIPR) team at Waikato Hospital to provide peer-led PFA10,16,17 to the full theatre team as a group. In light of the conflicting evidence about CISM debriefing, and in recognition of organisational demands favouring a shorter and earlier intervention, we have adapted our approach to focus on the ‘defuse’ component of CISM, ensuring all key safety factors are achieved.
After a critical incident, two trained peer responders will offer a defuse. This is a group facilitated conversation that contains a brief, focused narrative description of the events from the participants’ point of view, acknowledges the strong feelings that follow a critical incident, and provides resources for managing these. Our defuse is ideally held 24–48 hours following the event, when staff are psychologically ready, and allows those involved to gather together and acknowledge the impact of the event, the range of normal responses, and identify their immediate needs. It is less than an hour’s duration and helps staff to mobilise their individual and team coping resources to mitigate the psychological effect of the event. The structure of our intervention closely mirrors published structures for early PFA as detailed in Table 2.10,11,15 –17,31
Early psychological first aid interventions.
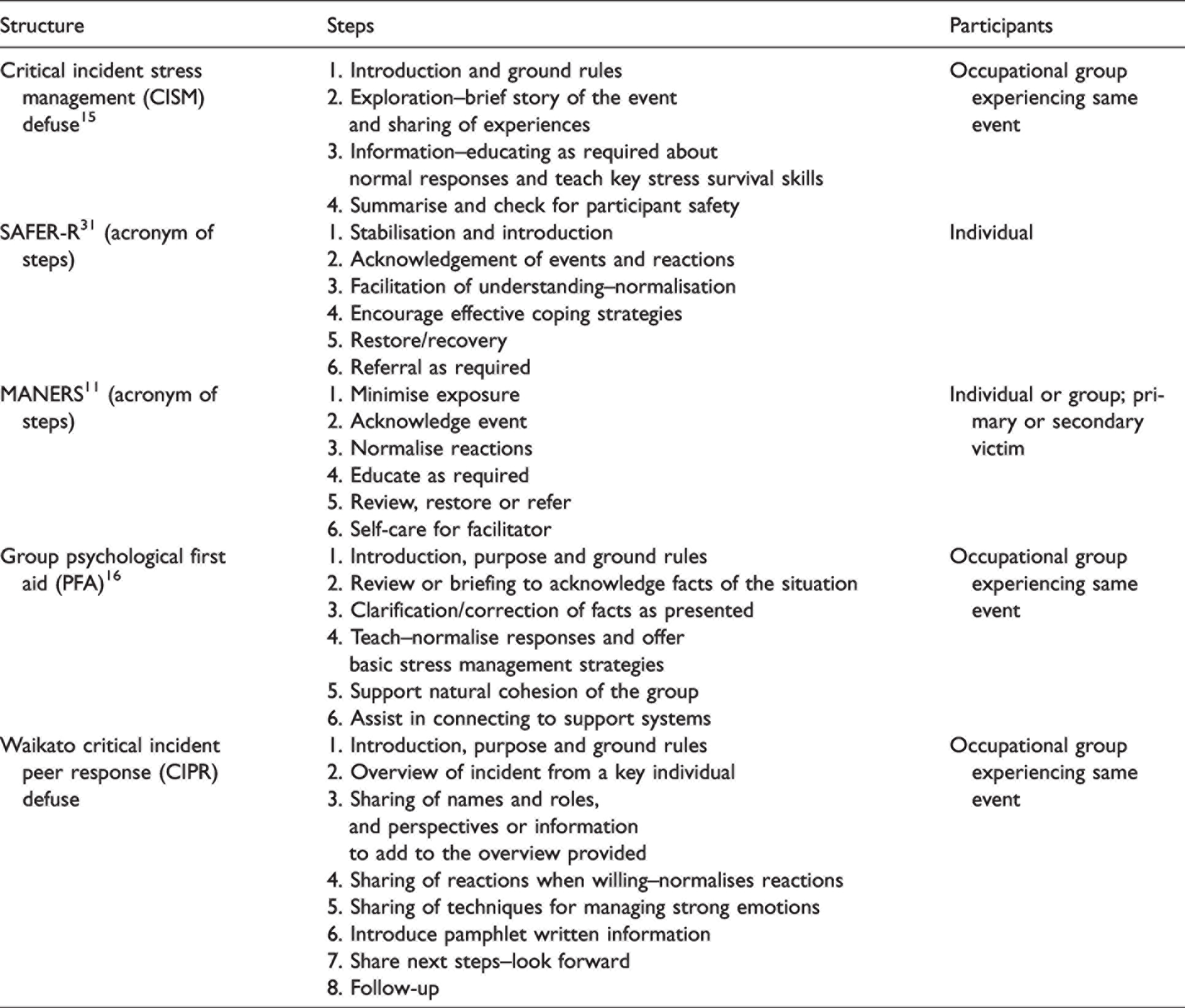
Our defuse structure heavily emphasises team education and support. Rather than ‘teaching’ about normal reactions and resources for responding to critical incident stress, the facilitators recognise the inherent resilience and knowledge within the team. The facilitators ask the team to share their reactions and their coping strategies with their colleagues.
Prior to the implementation of the current programme (2018), a more in-depth group intervention called a ‘debrief’ was held several times following critical incidents in theatre, by members of the current CIPR team who had been trained according to the CISM framework. A ‘debrief’ is held in the weeks after the event and helps staff to process the impact of the event on their lives and the way they are coping. This activity takes longer than the defuse, often two hours or more, and is designed to help people process their shared experiences. Since the implementation of the CIPR programme, this has been available as a further intervention if the staff involved request it, but has only been used rarely. Importantly, these two interventions have a wholly welfare focus. They are about reactions to the event, not about clinical decision-making, technical aspects of the case, or what could have been done differently. This distinguishes them from most ‘hot debrief’ structures. 24
Training and implementation
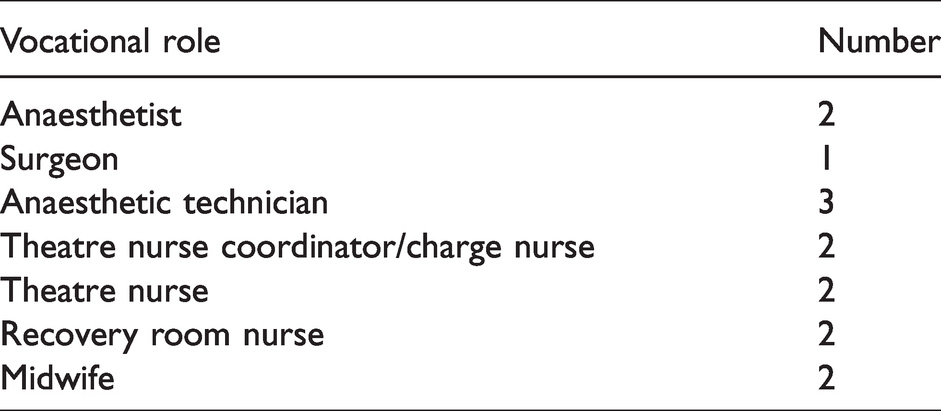
Our CIPR team consists of 14 members, carefully selected after nomination to be representative of the craft groups working in the operating theatre. Selected individuals had a perceived natural aptitude for this sort of work, including a reputation for respectful interactions, being able to hold confidences, being empathetic, and having the respect and admiration of their peers. Having a representative group has resulted in ‘buy-in’ from all groups, and with differing shift patterns, has ensured that there are almost always trained staff available on site to run a defuse (see Table 3).
Critical incident peer response team composition.
The three senior doctors in the team had previously attended a two-day group crisis intervention course provided by Critical Incident Management Australasia in mid-2018, in the pilot phases of the project. The remaining 11 CIPR team members attended a one-day bespoke CISM training course in February 2019, with the same instructor. This focused on the defuse for delivering early PFA. Professional development funding was used by the senior doctors, with the bespoke course for the wider team funded by the theatre service.
A dedicated mobile phone was provided for the service, and posters were created for the theatre suite, advertising the CIPR team telephone number and providing information about how to activate the service and what is involved. The service was promoted by way of education sessions to each of the large craft groups, and the phone number for the service was entered into the phone contact list for all the in-charge and on-call phones within the unit for easy activation.
A pamphlet was designed and printed for distribution to staff involved in a critical incident. This speaks to the typical feelings and reactions after a critical incident and how to activate support. This was created to offer at the end of a defuse, as a reference for staff themselves or their families, but it is also a useful resource for staff who are unable or unwilling to attend the defuse. Spare copies are available in the theatre coordination area for all staff to access. The pamphlet also includes a QR code to a feedback survey, which defuse participants can use to provide feedback on the service.
Process
Any member of the wider theatre and perioperative service can activate the CIPR service by phoning the CIPR team. The nominated CIPR team coordinator holds the phone and responds to calls. A clear answerphone message allows activation of the service even when the coordinator is not immediately available, with a mandate to check messages and respond a minimum of three times every 24 hours.
Once activated, a defuse is arranged. This is offered 24–48 hours after the event, but with flexibility within that time frame. Generally, the defuse is timed for a shift changeover. This allows maximal staff attendance, through a combination of early handovers to the next shift relieving participants of clinical duties, cross-cover from colleagues staying on, and some staff attending in unpaid time after completing their shift. It can be held in-hours, but most often has been held in the early morning or evening, including at weekends. The timing of a particular defuse is negotiated based on the likely availability of the majority of staff involved in the critical incident, discussion with the staff member who activated the defuse, and the availability of the potential defuse team.
The CIPR team coordinator communicates with CIPR team members by way of a WhatsApp group, to identify an appropriate and available defuse team. Two peer members of the CIPR team deliver the defuse, one in a leading role and the other available as a support person for both participants and their CIPR team colleague. The defuse is never delivered by a CIPR team member who has been involved in the critical incident themselves; on many occasions, there is a CIPR team member attending the defuse as a participant.
Once the timing and team for the defuse have been agreed on, a text message is sent to all involved staff members, inviting them to the defuse, with an explanation of what this involves and what to expect. This requires identifying the full list of individuals involved in a critical incident; the theatre management system is helpful in this regard, but is often inaccurate or incomplete in a crisis situation. Attendance at a defuse and participation in the discussion are entirely voluntary, and this message is reiterated at the start of each defuse.
Participants leave the defuse with an information pamphlet, and all are contacted again by the defuse facilitators 48 hours later. At that point, they can be directed to further support resources if required. The CIPR team coordinator then completes an audit tool, recording the date of the event and the intervention, the facilitators involved, and the number of staff attending the defuse.
Outcomes
The CIPR service has been in place at Waikato Hospital in pilot form since mid-2018 and in its full form since February 2019. Over the nearly three years of the full service, 28 defuse interventions have been delivered. This is equivalent to one every five weeks, although the critical incidents have tended to occur in waves. Thirteen of these interventions have happened in the first eight months of 2021. The requests for the longer ‘debrief’ intervention have all but disappeared, with just three held since 2018 and all in situations when a defuse was delayed or impossible due to operational requirements; none have been requested within the past 18 months. Over 200 members of staff have attended a defuse. The range of critical incidents has been broad, and has included a response to the multicasualty Whakari White Island eruption, several neonatal deaths, major trauma events including in children, and unexpected deaths in theatre.
It is difficult to assess formally the quality of the service. Feedback from participants is actively invited, and participants leave the defuse with information about how to provide that feedback anonymously. However, providing feedback is clearly not a priority for the individuals who have been involved in a psychologically challenging critical event, and we do not want to cause repeat trauma by asking individuals to recollect the event in order to provide feedback in a delayed form. These challenges are recognised in the literature.5,25,30 Fifteen responses to our simple four-question survey were received in 2021. All found the defuse ‘neutral’ through to ‘very helpful’. All would attend a defuse again in future, and all would recommend the process to a friend or colleague involved in a critical incident. Direct written feedback to CIPR team members in the form of emails and text messages has been overwhelmingly positive, and suggests that knowledge of the service, the willingness of the senior management team to support a welfare intervention, and the early contact by text message are also contributing to the wellbeing of staff.
Because attendance at a defuse is voluntary, there is a proportion of staff who do not attend. We do not collect data on the reason for this choice, so are unable to interpret whether this is due to unavailability, lack of perceived need, or because the programme is not culturally acceptable in its design. Similarly, we do not keep any permanent record about those who attend, in order to maintain the confidentiality of the session, and thus do not have demographic data. However, our impression is that participants who attend voluntarily represent the craft groups, the experience levels and the varied cultural backgrounds of our theatre team.
Discussion
This peer-led interprofessional team approach to psychological welfare following a critical incident has been called for in the anaesthetic literature 24 and more broadly in healthcare.6,9,11,13 There are well described programmes for peer support or buddy teams that provide individualised support,30,32,33 but we could not find reference to any peer support process that involved full theatre teams. We believe a peer-led team approach has merit, and is supported by the literature on PFA for groups.10,16,17
Anaesthetists do not work in isolation; they are part of a multidisciplinary theatre team. This type of intervention is understood to work more effectively when used for teams who work together regularly and have experienced the same critical incident—a ‘natural cohort’, 16 as this allows for the benefits of social support and camaraderie.16,17 The group approach also provides team members with the necessary opportunity to take an active role in their recovery from the event.11,17 It is the team that provides the support to each other through validation of shared reactions, social connection, and through role modelling to guide constructive self-help behaviours, including seeking help.16,17 It is not the facilitator who directly delivers this support. This avoids any suggestion of a victim versus hero dynamic, and is empowering for the team.
We have observed that the multidisciplinary nature of this approach reinforces the flattened hierarchy of the modern theatre team, and thus is consistent with other organisational approaches to support teamwork and communication in theatre.34,35 All staff involved have a perspective on the event that informs others. Our senior medical staff have willingly attended these sessions and shared their emotive responses to events. Often, this has been the first opportunity in their career to talk openly about the impact of critical incidents on their wellbeing. They often attend to be of support to their team, but receive benefit themselves, an observation supported by the literature. 17 All members of the team benefit from being reminded of the essential humanity of each member of the team, and in our environment this has been positively culture building.
It is our observation that the less experienced members of the team, or those not involved in the care of the patient prior to the critical incident, are most obviously affected by critical incidents. These individuals often do not have the same depth of case-specific knowledge, so what might be a semi-expected event for senior medical staff in theatre is entirely unexpected for other members of the team, and thus is more likely to be a distressing event for them. This discrepancy is often elucidated and mitigated in the defuse, and we are noticing more active sharing of likely prognosis in our surgical safety checklist time-out.
This welfare system is peer led. For success, facilitator credibility is important. 17 The facilitator should understand what is being discussed, through their own personal experience and knowledge of the ‘culture’ of the broader team.7,11,16,30 In the setting of a multidisciplinary theatre team, our peer facilitators come from across theatre craft groups, with a mix of backgrounds present at any one defuse. However, this is a key reason why requests to deliver our programme outside of the perioperative and theatre service have been declined; our CIPR team are not ‘peers’ for healthcare providers working outside of the operating theatre environment.
At times, it has been difficult for staff to recognise the emotional significance of an event at the time, and this has driven the development of some mandatory activation triggers. Several trained members of the CIPR team, including one of the authors, were involved clinically in critical incidents around the Whakari eruption, and despite being fully aware of the concept of critical incidents and availability of the service, they did not think activation of the CIPR service was necessary. A few days later, the profound need became clear, and debriefs were offered. The critical incident response is now embedded in the ‘death in theatre’ protocol with mandatory activation of the CIPR team, although attendance at any resulting defuse remains, of course, voluntary. Further, there are plans to incorporate this into the local surgical safety checklist sign-out discussion for all significant intraoperative events.
Other changes have been required since the implementation of this project. Initial contact with staff had been by staff email; however, this was not seen or responded to in a timely manner. Text contact has been more straightforward and successful, and staff have appreciated the personal touch in this. We have had to reiterate the optimal time frame for the defuse and resist requests to offer an immediate intervention, while staff are still involved in managing the aftermath of the incident.
The role of CIPR coordinator has been burdensome, and like all of the CIPR team roles, voluntary and unpaid. The move to primary use of an answerphone system has been one way to minimise the workload of the coordinator so that they are not required to be constantly available to respond to a call.
The CIPR team of 14 appears to be appropriately sized for a large tertiary hospital theatre suite. This has allowed the workload to be shared, without resulting in significant de-skilling of any members of the team. However, further development of the service requires a programme of maintenance of skills and the ability to train new members. Regular team meetings are held for both staff development and to discuss the impact of the defuse process on the emotional health of the facilitators. Moving forward, annual refresher courses and a formal process for professional supervision of team members will be vital for the long-term sustainability of the service.
It has been challenging to assess the quality of this programme rigorously. The literature on interventions for critical incident stress uses rates of PTSD as a marker of efficacy,19,25 –27 but it has been identified that the benefit of programmes such as this may not be in preventing pathological forms of distress. 26 Instead, these programmes may meet other needs, such as making social connections to improve general welfare, 26 improving quality of life,7,26 and decreasing absenteeism. 19 These are therefore useful outcome measures to review. Staff wellbeing surveys, audit of sick leave rates, and exit interviews on resignation could help to understand the impact of this programme.
The implementation and running of this service, and its ongoing sustainability, are dependent on managerial support. Beyond funding the initial training, the support of theatre management to allow flexible rostering solutions, which prioritise attendance for those who wish to participate, has been vital to facilitate the timely delivery of defuse interventions. These flexible work arrangements and the frequent out-of-hours delivery of the defuse limit the impact on clinical case load, and the literature suggests that addressing staff welfare needs after critical incidents helps to maintain the quality of clinical care provided, 2 to the benefit of patients. This, along with legal occupational health and safety requirements 11 and a potential to decrease absenteeism, 19 make compelling reasons to support a relatively low-cost, volunteer-run programme.
Recommendations
A supportive management group will simplify the establishment of a peer welfare programme and its integration into standard operating procedures. If this support is not naturally forthcoming, a pilot period to introduce the concept and generate staff endorsement may give the programme momentum. The psychological safety of all involved is paramount. The key points for delivering the service safely (Table 1) must be followed. Careful team selection is vital – both for craft group representation and for personal attributes. The coordinator role can be burdensome – simplified processes and rotating this role can help. Effort should be made to identify all team members involved in a critical incident—including allied staff such as radiographers and healthcare assistants. Theatre recording systems are often incomplete in a crisis and cannot be relied on. Contacting involved staff by personal text messages has multiple benefits—reliable communication of the invitation and expectations, an ability to receive an individualised response from that staff member, and a potential welfare benefit to this contact. Timing the delivery of the intervention is important. Staff must be psychologically ready. Pressure to deliver a defuse while staff are still dealing with aspects of the case must be resisted. Identifying situations in which a defuse is likely to be needed, and mandating activation in those situations, such as a death in theatre, offloads involved staff from having to request support. It is vital, when a defuse is arranged in that way, that staff attendance and participation remains entirely voluntary. Evaluation of a welfare service can be difficult to undertake without risking harm to participants. Participant feedback may be unreliable or incomplete. Reviewing broader measures of wellbeing such as surveys, absenteeism rates and exit interview data may help establish the value of the service. A CIPR team is only one part of a holistic strategy to address workplace wellbeing, and should be integrated into hospital critical incident management policy.
Summary
We have created a team-based welfare intervention that follows critical incident management principles with trained peer facilitators from within our theatre suite. While it is difficult truly to measure outcomes, we are receiving positive feedback and this work is developing the culture of teamwork and support at Waikato Hospital. Our programme, as described in this article, may assist others by offering a framework for developing team-based welfare interventions in other hospital departments.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank the members of the CIPR team for their ongoing contribution to the welfare of the perioperative team at Waikato Hospital, and the broader service for their support of this initiative.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.