
Abstract
Management of the difficult paediatric airway is challenging due to anatomical differences, congenital anomalies, paucity of paediatric airway management algorithms, and the limited availability of paediatric-sized airway devices. In this case report, we describe two cases highlighting the potential use of seemingly oversized videolaryngoscopes in the management of the difficult paediatric airway. Recognising the cause of difficult airway in the paediatric population is potentially useful in the selection of a larger videolaryngoscope blade to aid laryngoscopy and intubation.
Introduction
There are limited resources to guide the management of a difficult airway in paediatric patients. Unlike well-established difficult airway algorithms in adults, algorithms for paediatric populations are only emerging in recent years. The fundamental principle of difficult airway management published by the Difficult Airway Society is to maintain oxygenation and to maximise the likelihood of successful intubation at the first attempt, or failing that, to limit the number and duration of attempts at laryngoscopy to prevent airway trauma and progression to a ‘can’t intubate can’t oxygenate’ situation. 1 The airway algorithm emphasised the importance of change (technique, equipment, operator) following each failed attempt at difficult laryngoscopy. A recent analysis from the Pediatric Difficult Intubation Registry suggests that there is a lack of emphasis on use of videolaryngoscopes in this population. In children with difficult airways, 46% of anaesthetists selected direct laryngoscopy as their first-choice airway technique, and only 18% chose videolaryngoscopy. 2 The success rates for these two techniques were 3% and 55%, respectively.
Conventionally, the choice of airway devices in the paediatric population is guided by the patient’s weight or age. While the concept of using a larger-sized laryngoscope blade in children is not novel, it is not considered routine in the management of difficult paediatric airways. In 1997, the adult Bullard laryngoscope (Cricon ACMI, Stamford, CT, USA) was reported to be effective in facilitating tracheal intubation in children older than 12 months, with a mean (standard deviation) intubation time of 38 (13) seconds. 3 A more recent report by Lean and King in 2016 described the successful management of paediatric patients with Nager syndrome and mandibular hypoplasia using the C-MAC® adult D-blade (Karl Storz, Tuttlingen, Germany). 4 Despite half the blade protruding externally, it follows the airway curvature optimally, producing a superior laryngeal view. These findings suggest the potential use of larger laryngoscopes as an effective alternative tool in the management of the paediatric airway.
In this case report, we present two cases describing the use of seemingly oversized videolaryngoscopes in the management of difficult paediatric airways and the possible reasons for improved laryngeal views in these patients. We recognise that the choice of paediatric airway device is highly individualised and is influenced by other factors such as availability of the equipment and familiarity of the anaesthetist. In the event of a failed intubation attempt with conventionally sized airway devices, it may be worth considering sizing up the blades in suitable patients. The parents of both cases have given consent for publication.
Cases
Case 1
A seven-year-old 30 kg boy was admitted for acute onset stridor and dyspnoea triggered by an upper respiratory tract infection. He had a history of extensive aerodigestive tract lymphangioma with multiple previous resections. His condition had previously warranted a tracheostomy, which had been successfully decannulated at the age of four years, and he was currently undergoing chemotherapy. In view of acute desaturation despite maximum oxygen supplementation, immediate airway intervention was required. The patient underwent inhalational induction, and laryngoscopy was attempted by a consultant anaesthetist with both C-MAC size 2 and McGrath (Medtronic, Minneapolis, MN, USA) size 2 blades. The laryngeal view was impeded by the lateral superiorly located lymphangioma which overhung and obscured the laryngeal outlet. External laryngeal pressure and repositioning of the head did not improve the laryngeal view.
Subsequent intubation attempts made by the consultant surgeon using a 1.9 mm Micro-laryngo-bronchoscope (0 and 30-degree; Karl Storz, Tuttlingen, Germany) and a 2.8 mm fibreoptic bronchoscope (Karl Storz, Tuttlingen, Germany) also failed to visualise the larynx. Hence, a decision was made to secure the airway with a tracheostomy. A size 3 supraglottic airway was inserted and spontaneous ventilation was maintained. Tracheostomy was performed successfully, and the child remained stable throughout the procedure. In view of multiple intubation attempts, we performed surveillance of the airway using a C-MAC size 3 blade and C-MAC adult D-blade. Incidentally, we found that while the visualisation of the glottic opening was poor with the C-MAC size 3 blade, it was significantly improved from a Cormack–Lehane grade 4 to a grade 2B by using the C-MAC adult D-blade with the aid of external laryngeal pressure. In this patient, the C-MAC adult D-blade was chosen as the C-MAC D-blade Ped was not available at the centre during the time of the incident (see Figure 1).
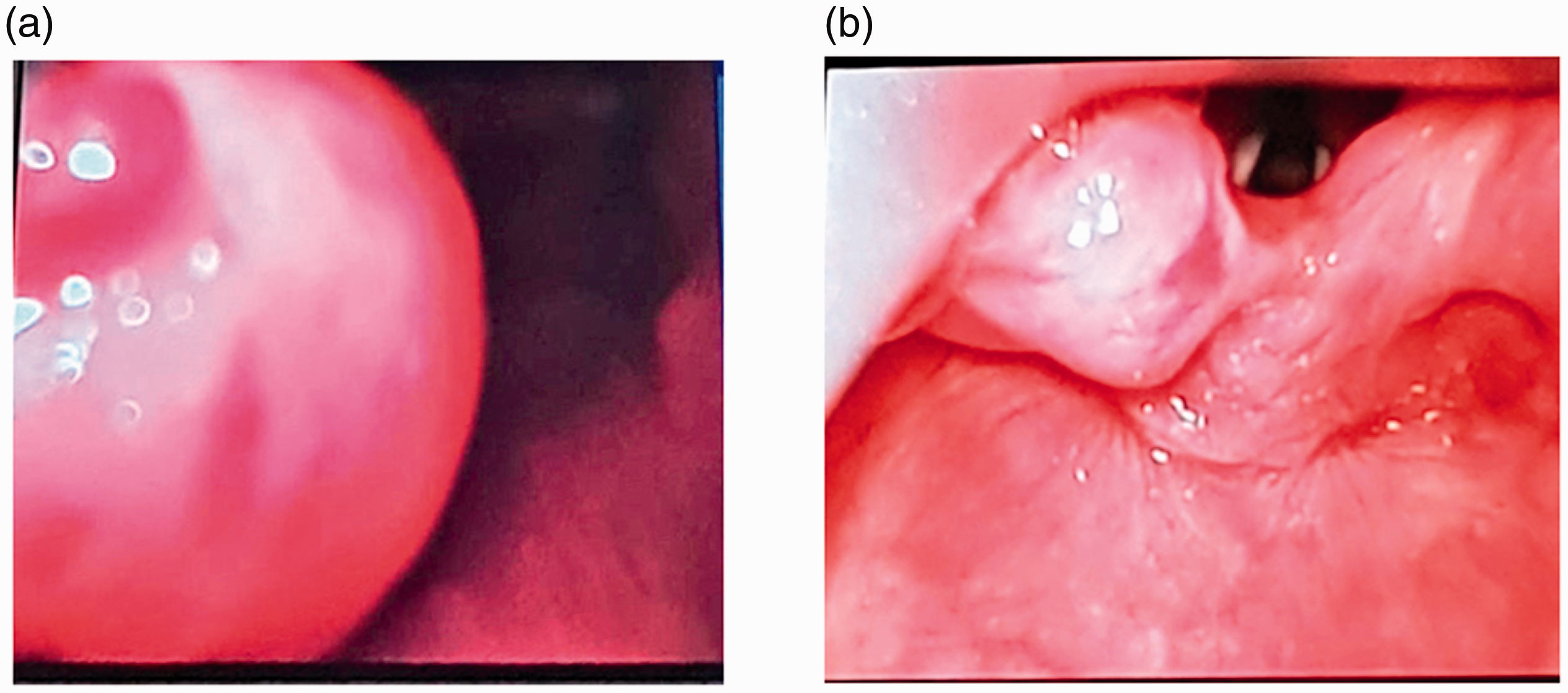
Comparison between the laryngeal views using (a) C-MAC size 3 blade and (b) C-MAC adult D-blade in a patient with aerodigestive tract lymphangioma (C-MAC®, Karl Storz, Tuttlingen, Germany).
After the procedure, the child remained stable without any oxygen supplementation and was transferred to intensive care. Postoperative magnetic resonance imaging, which was performed to evaluate the extent of lymphangioma, demonstrated significant narrowing of the hypopharynx and pharynx from cystic changes along the epiglottis. He was subsequently discharged with the tracheostomy and was planned for decannulation later after completion of chemotherapy.
Case 2
A 15 kg three-year-old girl presented for elective microlaryngeal bronchoscopy, examination of ears under anaesthesia, and somatosensory evoked potential testing. She had a medical history of Fraser syndrome with multiple congenital anomalies, including anterior laryngeal web and subglottic stenosis. A difficult airway had been noted during anaesthesia at another hospital although no laryngeal grade had been recorded. On examination, the patient had a depressed nasal bridge, hypertelorism and microstomia. Inhalational induction was performed, and the patient was maintained on spontaneous ventilation with sevoflurane. Anticipating a potential difficult airway, the C-MAC D-blade Ped was chosen to visualise the vocal cords for topicalisation. However, due to her microstomia, the blade did not fit fully into her mouth. Despite being inappropriately large, we were able to obtain a Cormack–Lehane grade 1 view of the vocal cords (see Figures 2 and 3).

Image of C-Mac D-blade Ped used for visualisation of vocal cords for topicalisation. Note that the blade did not fit fully into the oral cavity (C-MAC®, Karl Storz, Tuttlingen, Germany).
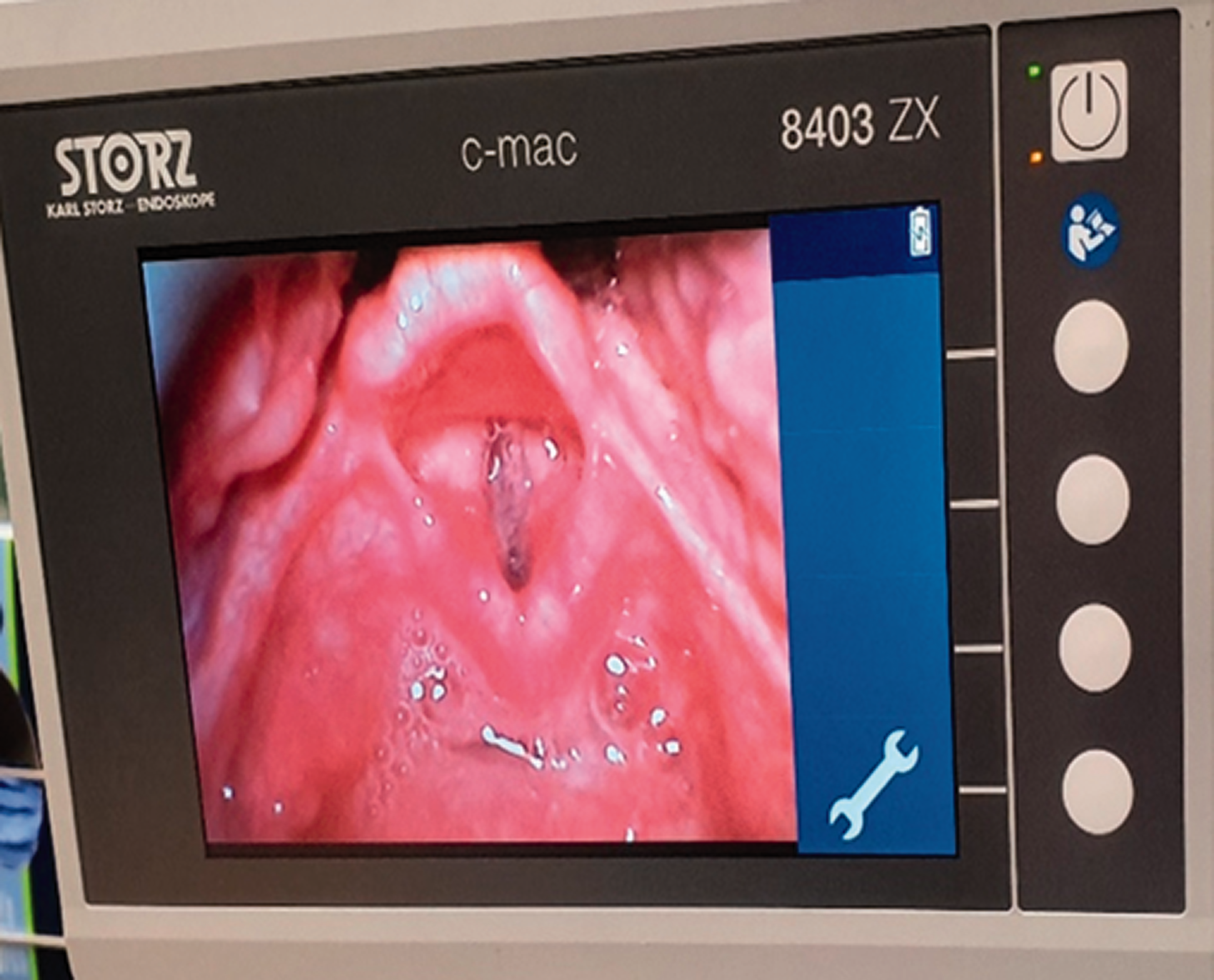
Cormack–Lehane grade 1 view of the vocal cords using C-MAC® D-blade Ped (Karl Storz, Tuttlingen, Germany).
Following bronchoscopy, a supraglottic airway was used for ventilation for the rest of the surgery and the procedure was completed uneventfully.
Discussion
Videolaryngoscopy is emerging as a tool of choice for endotracheal intubation as it provides higher success rates with potentially lower complication rates. 5 It has a faster learning curve as compared to direct laryngoscopy, improving the chance of successful intubation even in untrained medical personnel. 6
The C-MAC D-blade videolaryngoscope has a hyperangulated blade with an increase in angulation from 18° in the conventional C-MAC size 3 blade to 40° in the C-MAC D-blade. This allows better alignment of the airway axis with minimal neck extension. In a randomised crossover study of simulated patients with cervical immobilisation, the C-MAC D-blade videolaryngoscope caused less upper cervical spine motion than the Macintosh laryngoscope during tracheal intubation. 7 Our cases highlight other scenarios in which the use of a C-MAC D-blade may be applicable even in situations when blades are seemingly inappropriately sized.
In paediatric anaesthesia, such considerations assume even greater importance as the use of awake fibreoptic bronchoscopy, the gold standard for difficult adult airways, is extremely challenging.
In the first case, the C-MAC adult D-blade would have been considered inappropriately large for a seven-year-old child. However, it produced a superior laryngeal view compared to other paediatric-sized blades by displacing the extrinsic mass that obliterated the laryngeal view. We postulate that the spatial dimension produced by the length and depth of the C-MAC adult D-blade provided the optimal leverage to scoop and lift the mass from the laryngeal outlet, resulting in the improved view which was not achieved with the standard C-MAC, McGrath blades or fibreoptic scopes. This suggests that the C-MAC D-blade may be worth considering in patients with a difficult airway due to the presence of airway masses, which could potentially be displaced by lifting the mass, thus avoiding the need for an invasive airway.
In the second case, despite limited placement of the blade in the oral cavity, the C-MAC D-blade Ped was able to yield a better laryngeal view. In patients with microstomia, the C-MAC D-blade Ped may not be an obvious choice due to the inability to fit the blade fully in the mouth. However, despite half of the blade protruding externally, we were able to obtain a superior laryngeal view. This could be explained by the fact that the hyperangulated nature of the C-MAC D-blade Ped allows alignment of the airway axis without the need to insert the blade fully in the oral cavity. We note that this supports the findings described by Lean and King 4 in their management of patients with mandibular hypoplasia.
However, we recognise that a good laryngeal view does not necessarily guarantee a successful tracheal intubation, as the position of the camera on a hyperangulated D-blade videolaryngoscope may impede tube placement with the endotracheal tube abutting the area posterior to the glottis. In this case, withdrawing the blade partially provides a bird’s eye view which could facilitate tube insertion. In patients with airway masses which could be displaced by the blade, there is significant risk of airway bleeding if tissue is friable. This is catastrophic against the background of a difficult airway. Prior to the attempt, it is crucial to ensure that equipment and expertise for front-of-neck access are readily available. In patients with microstomia, the risk of soft tissue trauma may be inevitable due to inappropriate leverage exerted by the laryngoscope blade. Due to reduced space in the oral cavity, airway adjuncts, such as a bougie, may be essential to aid intubation. In spite of the possible limitations of oversized laryngoscope blades in paediatric patients, with careful patient selection, their use may avoid the need for an invasive airway.
Conclusion
In both cases, seemingly oversized laryngoscopes were useful in producing better laryngeal views. We suggest that in cases in which conventionally sized blades fail to facilitate intubation, it may be worth considering sizing up the blade in selected patients. However, appropriate patient selection and careful airway manipulation are important to improve the success of intubation.
Footnotes
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author Contribution(s)
Acknowledgements
The author(s) wish to thank the patients and their families for participating in this study and allowing them to share their medical history and images.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.