
Abstract
Upper airway compression is one of the clinical manifestations of thoracic aortic aneurysm, which is associated with poor prognosis and high mortality. A 44-year-old patient with ascending aortic and arch aneurysm who was scheduled for Bentall surgery and total arch replacement under cardiopulmonary bypass suffered difficult ventilation after endotracheal intubation. The patient did not exhibit any positional dyspnoea or orthopnoea, did not show any difficulties in the supine position, and had no noteworthy medical history. However, we encountered unexpected hypoventilation after intubation. Isoprenaline infusion was effective while emergency cardiopulmonary bypass was established to deal with this crisis. Fibreoptic bronchoscopy revealed complete obstruction of the carina and confirmed the supracarinal position of the tube. Complete airway obstruction may occur even if there are no symptoms before surgery in patients with thoracic aortic aneurysm. Comprehensive preoperative assessment, a well-developed airway management plan, and responses to possible emergencies are essential to reduce unnecessary events or complications.
We would like to report a case of unexpected intraoperative airway obstruction after tracheal intubation in a patient with an aneurysm of the ascending aorta and aortic arch. Computed tomography angiography revealed a maximal cross-sectional aneurysm diameter of 8.4 cm, while the trachea was compressed with a minimum diameter of 0.51 cm (Figure 1). The patient did not exhibit any dyspnoea, orthopnoea, cough, or stridor in the sitting or supine position preoperatively. After routine preoperative preparation by the surgeon, nurse, perfusionist and anaesthesiologist, anaesthesia was induced and mask ventilation was initially almost normal with a fractional inspired oxygen (FiO2) level of 1.0, tidal volumes of about 400 ml, and positive airway pressure of about 15 cmH2O. However, after apparent successful intubation using a 7.0 mm (internal diameter) cuffed tracheal tube, the airway pressure increased to 40–50 cmH2O, and effective ventilation could not be achieved. No end-tidal carbon dioxide (ETCO2) was obtained. At this time the systolic blood pressure (SBP) was 170 mmHg. The anaesthesiologist initially considered the problem to be severe bronchospasm and epinephrine (adrenaline) (20 μg intravenously (i.v.)) was administered. After epinephrine administration, the SBP increased to over 200 mmHg, the heart rate to about 130 per minute, and ventilation still could not be achieved. Isoprenaline 20 μg i.v. was administered and the ventilation transiently returned to normal, with a return of the peripheral oxygen saturation (SpO2) to 100% (from a nadir of 60%). However, ventilation again became increasingly difficult with increasing airway pressures, and became impossible over a further period of about three minutes. At this stage a plan for emergency cardiopulmonary bypass (CPB) was made with peripheral access through the femoral vessels. The CPB circuit was already primed, and two surgeons were already available in the operating theatre. After administration of heparin, venous and arterial cannulae were inserted. CPB was instituted within seven minutes of the commencement of femoral cannula insertion. During this time the SpO2 dropped to 60%, but cardiac arrest did not occur. Fibreoptic bronchoscopy after the institution of CPB confirmed the correct supracarinal position of the tracheal tube, but revealed complete obstruction of the carina due to external compression. After completing a Bentall’s procedure and replacement of the ascending aorta and proximal aortic arch with an interposition graft, normal positive pressure ventilation was possible and separation from CPB was achieved uneventfully. The patient provided consent to the publication of these details and the accompanying images.
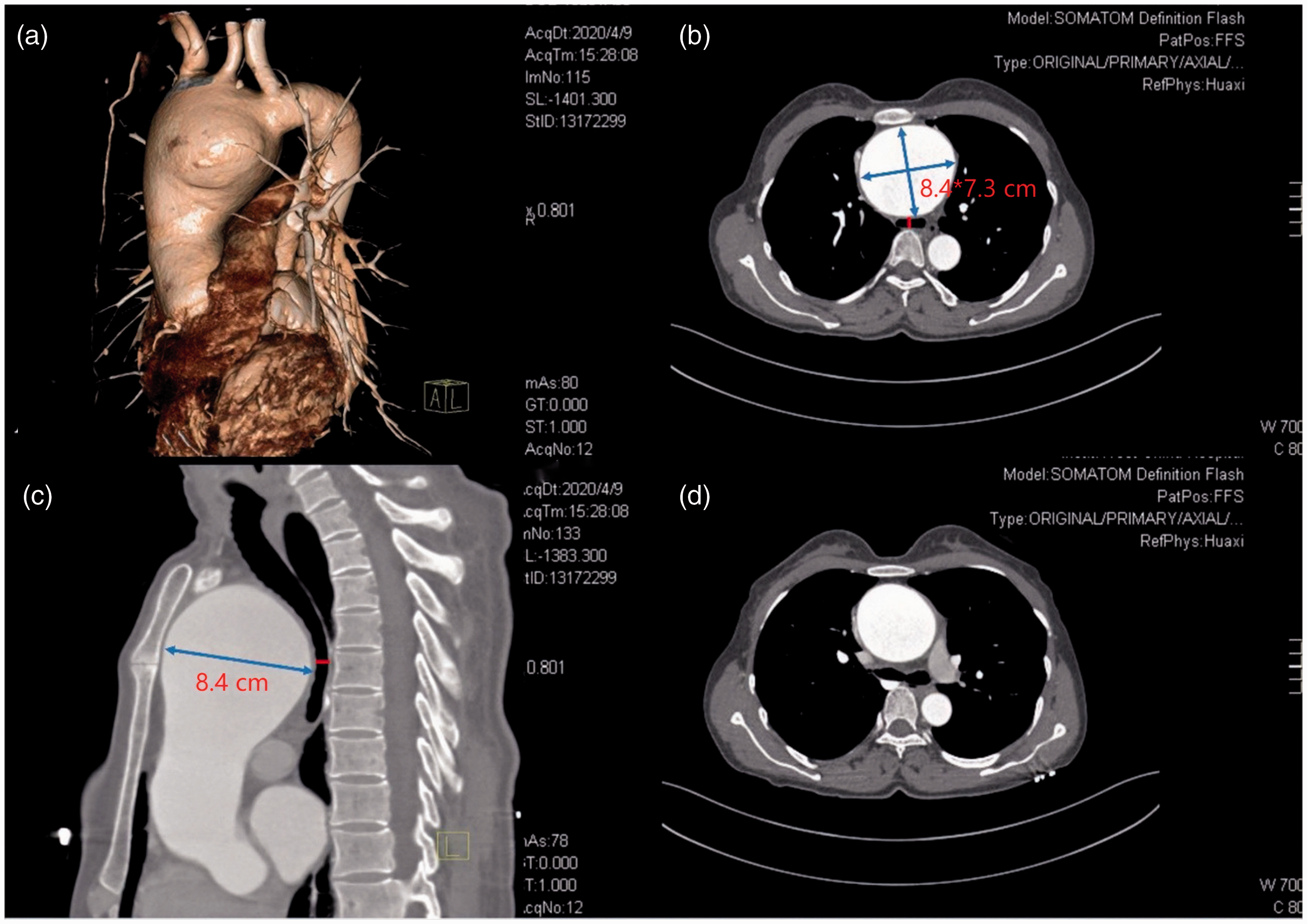
Computed tomography angiography of the aneurysm. The maximum cross-section of the aneurysm is 8.4 × 7.3 cm (arrow) and the minimum diameter of the trachea is only 0.51 cm (mark). (a) Three-dimensional reconstruction view. (b) Transverse plane of the narrow trachea. (c) Sagittal plane of the narrow trachea. (d) Transverse plane of the normal major bronchi distal to the carina.
The risks of general anaesthesia in patients with large anterior mediastinal masses have become well known, especially for patients with marked symptoms of airway compromise such as dyspnoea at rest, postural dyspnoea, orthopnoea, or even stridor. 1 When the cross-sectional area of the trachea is compressed more than 50% of predicted, the patient may be more vulnerable to airway obstruction despite the absence of symptoms preoperatively.2,3 Although three-dimensional reconstructions are currently possible, there are no data on predicting airway compression based on aneurysm size alone. A more recent paper has suggested adding a functional approach to the radiological studies, using pulmonary function tests (PFTs) with a careful history for any subtle symptoms of airway compromise. 4 Other reports favour an algorithm approach, and advocate flow/volume loop analysis, specifically the peak expiratory flow rate (PEFR), as a predictor of adverse anaesthetic outcome. 2 A PEFR of less than 50% of the predicted value by the comprehensive PFT and supine/upright flow volume loop spirometry should raise concerns about potential complications due to tracheal compression. 2 Most analyses show substantial correlation between PEFR and anatomical findings of airway narrowing. 4
General anaesthesia has been shown to affect pulmonary mechanics by reducing functional residual capacity and by relaxing airway smooth muscles. 1 In addition, there is loss of the normal negative inspiratory pressure.4,5 However, the size and the location of the aneurysm are the most important factors influencing the likelihood of airway compression. 6 More importantly, an ascending aortic aneurysm may dilate further as SBP rises, which could lead to greater airway compression. In combination, these influences could provoke severe airway obstruction after the induction of anaesthesia, which we consider was the most likely cause for the dynamic airway compression in our patient.
We recommend careful history taking for symptoms of dynamic airway compression in all patients with aneurysms of the ascending aorta, and PFTs with flow/volume loop studies in elective cases if airway compression is suspected. Avoiding hypertension is critical for all patients with ascending aortic aneurysms, but particularly if they have radiographical or other evidence of airway compression. In all cases with large ascending aortic and arch aneursyms there should be contingency plans to manage possible airway compression, and this should include early preparation for CPB if necessary.
Footnotes
Author Contribution(s)
Acknowledgements
The author(s) would like to thank the patient for allowing them to publish the case and to use the images taken.
Declaration of conflicting interests
The author(s) have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.