
Abstract
Over the last decades public discussion of opioids has changed radically. Opioid was once a word largely restricted to professional medical and pharmacological use for the treatment and management of pain. But propelled by the rapidly growing international wave of opioid use and overuse, it is now part of a much wider public discussion that covers more than pain medicine: dependency, addiction, over-prescription and oversupply, recreational drug use, and criminal drug trafficking. The word opioid is now controversial and value-laden. A key component of the developing views and values about opioids is carried by language, both written and spoken: on radio and television, in the social media, but also between healthcare professionals and patients, where communicating about pain in a context of emotionally and value-charged images of opioids can be challenging. This paper analyses aspects of the language of opioids. We document the shift from medical to addiction meanings and uses in the key term opioid, together with narcotic, drug, heroin, and to a lesser degree opiate and morphine. These changes follow four chronological phases in attitudes to pain and its treatment: traditional medical approaches to pain; pain being recognised as an under-treated ‘fifth vital sign’; the pharmacological and medical promotion of opioid use for treating pain, especially chronic pain; and the current reaction where opioid has become a pejorative and emotive term, closely connected to words like epidemic and addiction. We investigate whether and how a less charged and more balanced discourse might be possible.
Introduction
Unfortunately […] opium has gathered a disgraceful public image since Victorian times.1
2018 data shows that every day, 128 people in the United States die after overdosing on opioids. The misuse of and addiction to opioids […] is a serious national crisis that affects public health as well as social and economic welfare.2
There is a war on opioids in this country [USA].3
Pain has a long history of relative neglect in the medical disciplines.4 Both acute and chronic pain have long been treated with opium and more recently opioids, whose use is more commonly accepted in post-surgical pain management, cancer, and end-of-life pain. Opioids have a more controversial role in treating other kinds of chronic pain, especially chronic non-cancer pain (CNCP). However, the last three decades have seen a major shift around chronic pain. It has finally been fully recognised in ICD-11, the International Classification of Diseases.5 There have also been major shifts in how we talk about chronic pain, and how to manage it. These ‘discourses’ about CNCP are the focus of this investigation. When such matters are taken up by public debate they can become politicised and emotional, and the discussion space can become confused and messy, to the detriment of objective debate. Such is the case with contemporary discussions over topics like abortion, euthanasia, genetic engineering of foods, and climate change. It is also true of the current controversy over the role of opioids in medicine, public health and drugs of addiction, especially but not solely for CNCP.
Opioids: Chronology and attitudes
The history of opioids and ‘painkillers’ has been comprehensively covered elsewhere.6–9 For our present purposes we need only document selected indicative dates and events to identify the major chronological moments for the language analysis to follow.
The various opium-related substances all began as medicines, narcotics, soporifics and analgesics, and as early means of anaesthesia.10 The medical history of opium goes back at least to the ancient Sumerians in the 5th millennium BC, and has long been established in the Western world, for instance in the form of laudanum (opium mixed with alcohol) used by the physician Paracelsus in the 16th century (c). The English poet Coleridge started taking laudanum for pain, and became addicted. De Quincey’s Confessions of an English Opium-eater documented both the highs and lows of the opium experience.11 Clive of India took opium regularly as a relaxant. Over the 19c opioids became increasingly more involved in social and recreational use. The addictive properties of opium were widely known after the infamous Opium Wars (1839–1842, 1856–1860), where the Western powers used their military and economic dominance to exploit the opium trade into China. Morphine was discovered in 1817, and heroin in the late 19c. Pharmaceutical companies in the 19c and 20c regularly added opioids to their formulae. And even Coca-Cola, invented in the USA in 1886, originally contained cocaine, which, though not an opioid, is certainly addictive. The gradual adoption of opioid substances like morphine, and more recently of synthetic forms like heroin and then fentanyl, have led to addiction and a range of personal, social and epidemiological problems.
The medical use of opioids has been closely related to the history of pain. Bourke documents the progression of pain from ‘prayer to painkillers’, as pain has been gradually passed from being a matter of theology and divine punishment to a symptom susceptible to human intervention and substantial control.4 Most recently pain has become recognised not merely as a symptom of other medical dysfunction, but as a medical condition in its own right, especially in CNCP. This reconceptualisation is captured in the July 2020 revision of the definition of pain by the International Association for the Study of Pain.12 Such a revision, however, would not have been possible without a major shift of perspective on CNCP in the 1990s.
The recent history of pain in medicine, public health and ‘big pharma’ has been dominated by developments in the USA. The gathering realisation that pain was being medically under-treated was marked by the 1996 declaration by the President of the American Pain Society that pain is the ‘fifth vital sign’, a body condition ranking with body temperature, blood pressure, heart rate and breathing, as a key indicator to be checked by physicians in medical examinations. This declaration was shortly followed in 2000 by the introduction of new pain management standards by the Joint Commission on the Accreditation of Healthcare Organizations, which relaxed key restrictions on physicians in the prescribing of pain-controlling drugs, thereby creating another problem.13
This relaxation included opioids. During the 1990s a number of large pharmaceutical companies, mainly in the USA, developed and aggressively marketed new ranges of opioid drugs for the treatment of pain, especially targeted at the market for non-cancer pain. This advertising push followed a long tradition of medical advertising in the USA, some of which in days of yore was doubtless closer to snake oil than the real oil,14,15 and some of which certainly contained disclosed or undisclosed quantities of substances like morphine. The 1990s opioid campaigns, however, were motivated by ambitious financial rewards. Propelled by opioids like oxycodone, now revised in a slow-release formulation called OxyContin, the drug companies spent US$3.6bn on advertising in 2006. Their primary target was physicians, who responded by writing 6.2 million prescriptions for opioids in 2002.15
The advertising tone was upbeat and reassuring, as illustrated in one OxyContin television advertisement from its multi-billion-dollar manufacturer Purdue Pharma,16 which was sent to 15,000 doctors in 1998 with reassuring endorsements from patients who reported ‘getting their lives back’ thanks to OxyContin. Other Purdue advertising material at this time claimed that less than 1% of patients who took opioids became addicted;17 van Zee claims that the real lifetime figure is between 3% and 16%,18 though firm data are still lacking. According to Manchikanti et al.,13 ‘These positions are based on unsound science and blatant misinformation, and accompanied by the dangerous assumptions that opioids are highly effective and safe, and devoid of adverse events when prescribed by physicians’.
In 2019, 71,130 Americans died from drug-related overdoses or 21.6 per 100,000 of population (the parallel figures for Australia were 2,227 deaths and 8.7 per 100,000).19,20 Eventually the situation became intolerable. Purdue Pharma was faced with multiple class actions, and eventually filed for Chapter 11 bankruptcy in 2019,21 a category of bankruptcy that dissolved the company and re-established it as a public trust to respond to claimants and their communities. From the point of view of ‘big pharma’, the first, less regulated phase of the opioid boom was over.
But much damage had already been done. The growth of opioid use has been particularly marked and disquieting in the USA, where 5% of the world’s population is now consuming 80% of the world’s prescribed opioids. As a result, the involvement of opioids was publicly declared an ‘epidemic’ by the USA’s Centers for Disease Control and Prevention (CDC).22–24 This position, and the language accompanying it, has been supported by a number of other American institutions like the Food and Drug Administration and the National Institute on Drug Abuse.2,25
This theme was picked by up the Trump administration, which declared a ‘Public Health Emergency’,2 and produced an important programme of legislation in 2018: the Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment (SUPPORT) for Patients and Communities Act, with goals including teaching addiction medicine and standardising delivery of treatment. This initiative was endorsed by the American Society of Addiction Medicine;27 (see also Boyles28). It was reported to be the ‘single largest legislative package addressing a single drug crisis in history’.26 And the STOP Act, in full the ‘Synthetics Trafficking and Overdose Prevention Act of 2018’, included US$6bn of funding to target opioid abuse, and over US$1bn for research into opioids and pain issues.29
Epidemic, pandemic, Covid and opioids
By an unanticipated piece of serendipity, the status of the ‘epidemic of opioids’ has potentially been furthered by the pandemic of Covid-19. The world has not experienced a pandemic since the ‘Spanish Flu’ of 1918–1919, which is beyond the memory of almost anyone alive today. But Covid-19 has imposed on our lives the constraints, threats, risks and privations, and in some cases the mortality, of a genuine pandemic that crosses national boundaries. True, the opioid ‘epidemic’ is indeed more serious in the USA, where public policy allows the direct marketing of named drugs to the general public. And it is American public policy and medical bodies that have been leading the campaign against the opioid problem, which they have framed as an ‘epidemic’, since they are addressing it as an American problem, even though in geographical outreach it is an international pandemic.
Both pandemics and epidemics come equipped with metaphors: war and struggle, victors and vanquished, sacrifice, deprivation of liberty and movement, and more. In the opioid domain, different countries and jurisdictions are moving, though with only limited signs of coordination, to restrict over-the-counter access to medicines containing opioids, to tackle the problems of populations with opioid abuse, and to address the problem of illegal drug supply. The language is often aggressive and confrontational, sometimes apocalyptic. There is an undeniable stigma that is increasingly being attached to users of opioids in our communities.
But unlike Covid—at least, as Covid has played out in the USA—the opioid epidemic has not polarised the public at large. It was not politicised, at least initially. At the governmental level, judging by public statements from major parties, concern over the opioid epidemic looks to have bipartisan support. But as we shall see below, there is a major split among the medical profession, and among the people living with pain who are directly impacted by the arguments directed against opioids.
Language, denotation, connotation and values
We now turn to the resources provided by language for the formation and negotiation of themes and attitudes, both in general and with a special focus on opioids, the word opioid itself, and the ways it is used in current public and professional language. The details of this controversy are not well understood by the general public, nor by some policymakers. There are assumptions that all opioids can cause dependence, which can lead to addiction (true), that all addictive substances are opioids (false), and there is much fuzzy rhetoric, often impassioned, around addiction and epidemics. As we shall see later, the use of language has a lot to do with this, and with the ways in which the word opioid has been made pejorative, negative and a target for criticism.
One of the fundamental burdens of this communication of attitudes falls to words, and words combined with other words. In the discipline of semantics—the study of meaning—a key distinction is drawn between denotation, or the literal, objective meaning-content of words, and their connotation, or subjective and emotional overtones. The word table, for instance, denotes an object of furniture with three or more legs, a surface, and with certain social functions like dining, discussion and so on. Its connotations are relatively restricted. Other words have a high connotative load. Rape, murder, and torture all denote different varieties of violent behaviour, and have strongly negative evaluative connotations. Virtue, compassion, mercy and empathy all show strongly positive connotations, though forgiveness, while meritorious in Christian value systems, would have been negatively evaluated in warlike cultures like the Vikings. Time and cultural value systems can therefore influence connotations. And over time words can undergo ‘pejoration’, which means that they become less favourably evaluated; or they can undergo the reverse, known as ‘melioration’, when they become more favourably evaluated. For example, bourgeois and capitalist were strongly pejorative under Stalinist communism, while communist and socialist were positive. The emotional orientation of this pairing was radically reversed when communism came to an end in Europe in 1989–1991. Throughout Eastern Europe and the Soviet Union words like bourgeois and capitalist underwent extensive melioration to become positive and approved terms, while communist and socialist have suffered pejoration and are no longer respected as they once were. As we shall shortly see, opioid is a word that has recently undergone substantial pejoration.
The word pain, and its synonyms and near synonyms like ache, hurt and sore, all carry negative connotations in English. Furthermore, pain words occur typically with other words that have negative overtones. These word combinations are called collocations. One suffers pain, and the verb suffer only occurs with words that also have negative implications: one suffers a fall, a loss, betrayal or bereavement. Except in the context of sadism and masochism, and some religious texts involving pain as a means of overcoming human misdeeds and sins, there are few joyful expressions involving pain.4,30
Language data can also be used to reveal attitudes and shifts in public discourse relating to the opioid ‘epidemic’. But more than just revealing these aspects, language use is central to the delivery and management of appropriate medical care for people in pain, and this language use around opioid now finds itself enmeshed in a complex web of negatively charged rhetoric related to the opioid epidemic, and ways of tackling it. The war metaphor is highly relevant, and has been used to heighten awareness of the nature and seriousness of the epidemic, and the need to combat it vigorously and, for some in public life, ruthlessly. And opioid discourses are all the more difficult because they inevitably inherit the complexities, taboos, stigma and interpersonal problems of talking about pain.
Pain, communication and the ‘epidemic’ of opioids
The vocabulary and tone used in these messages about opioids is characterised by dramatic language: epidemic (CDC), disorder, emergency, crisis, trafficking and overdose.26,29 In part this echoed emerging themes in the media. But it also set the tone of public debate and confrontation. There had been a widespread and rapid increase of concern and discussion from political sources, the media and social media, as well as in the professional literature. In many cases the shift to a strong, emotive and accusatory discourse was certainly justified. But as a result it was not always balanced, and has now captured most of the debate about opioids, to the point where its shadow is seen in the long medical tradition of using opioids to treat certain types of acute, cancer and end-of-life pain in ways that have established therapeutic validation. This language use both reflects and shapes public and professional attitudes and beliefs, and those of people involved in pain, professionally and as patients. It has become difficult to talk about these matters in an objective, constructive and informed way.
Communicating about pain itself is seldom straightforward. Its private and subjective nature interposes problems of description and communication, for instance between patients and pain physicians. Pain is further compromised by its different interpretation in different languages and cultures. Communication—and under-communication—about pain has also only recently begun to attract serious research interest,31–34 and understanding pain talk remains an under-investigated area of medicine. This situation is substantially exacerbated by the current aggravated public controversy over opioids.
To address these issues, we will draw eclectically on a number of sources:
the medical, clinical, pharmacological and related literatures on pain and opioids; the more restricted research literature on communication and pain and opioids; the extensive material in the media, information media, social media, public policy and medical policy about opioids and their current social use, misuse and consequences; material addressing what is often referred to as the ‘epidemic’ of opioid use in our society, and policy initiatives aimed at getting control of it.
The ultimate target audience of this paper is practising healthcare professionals treating people with pain, the people in pain themselves, and those engaged in public health policy and its discussion. The goal of the paper is to help clarify the now thoroughly confused discussion space of opioids in pain medicine, and to help these stakeholders establish a basis for productive working communication about opioids and their potential role in the management of pain.
As a linguist with no medical qualifications, I take no position for or against opioids in their medical role. In the medical literature there are those who advocate for a medically supervised and controlled use of opioids for specific purposes, especially the control of cancer pain or pain in a palliative setting and select acute pain contexts; for example,35 ‘The success of carefully controlled and monitored narcotics for the benefit of cancer patients in pain spread to other problems, such as the control of postoperative pain and pain in childbirth’.
Patients undergoing such therapeutic regimens can feel ambivalent about their treatment because of the widespread negative public rhetoric about opioids. Others argue strongly against opioids. And there is a growing body of people, including medical professionals who are concerned that not enough is being done to help people with opioid problems to address them and hopefully give up their addiction. These groups are currently talking in substantially different ways. So my goal is to identify different ways of talking about opioids in contemporary public discourse, using the medical literature on opioids and attitudes towards them, together with large databases of public English; to associate these different ways of talking about opioids with different evaluations of the role of opioids in medicine and epidemiology; and to analyse how these different ways of talking influence the ability of language to capture and project different positions on the role of opioids in contemporary life.
The vocabulary of drug-related terms
In the USA, and increasingly in Australia, there is a special acronym ‘OUD’ standing for ‘opioid use disorder’, parallel to ‘AUD’ for ‘alcohol use disorder’. ‘Disorder’ refers to an illness that disrupts normal physical or mental functions. It is not inherently severely prejudicial, except insofar as it picks up the idea of departure from ‘normal’ patterns. But as we will see below in discussing stigma, OUD is involved in significant judgements of social negativity in the USA.
Before we investigate the connotation fate of opioid, together with narcotic, drug, opiate, heroin and morphine, we need to assemble some related key terms and definitions. The key terms in this domain are often not well understood, particularly by the non-medical public. And the range of their meanings is not always clearly delineated, even in medical dictionaries.
The use of drugs or opioids is accompanied by tolerance, dependence and withdrawal, and addiction, which form a scale of increasing severity: Tolerance, tolerant Tolerance occurs when the body shows a diminished response to a drug after continued use. Larger doses of the drug are needed to achieve the same effect as before.
Dependence, dependency
Dependence (less commonly dependency) usually refers to physical dependence or reliance on a substance, accompanied by tolerance and withdrawal. But dependence need not imply addiction. A diabetic on insulin is dependent on the insulin for maintaining their levels of health, but is not addicted.
Withdrawal
The process of ceasing to take a substance to which a person has become addicted, together with the accompanying physical and mental responses. Addict, addiction, addictive An addict is someone who is physically and mentally dependent on a substance or drug. Addiction is the property of having that dependency. The adjective addictive, however, describes
Recreational has undergone pejoration, in that its original innocent meaning of ‘something done for pleasure away from work’ has now become enmeshed with illegal activity: Recreational, illegal, misuse, abuse In the non-therapeutic sense, recreational refers to a substance from the pharmacological domain used, and misused, outside the reach of prescribed medicines. In its new second sense recreational has become approximately synonymous with illegal, misuse and abuse.
There are obvious overtones of negativity and condemnation. In order to mitigate these effects, the American Psychiatric Association, in the 5th edition of their authoritative Diagnostic and Statistical Manual of Mental Disorders (DSM-5),36 abandoned the use of substance abuse and substance dependence in favour of substance use disorder, with three levels: mild, moderate, and severe. This is not so much a euphemism as an attempt to avoid discriminatory language that could negatively colour diagnosis. Since the present paper is principally concerned with public discourse about opioids and their interpretation, we will not focus specially on the phrase substance use disorder, which is found mainly in technical and professional usage.
Opioid and substances of addiction
In terms of the English lexicon there are six typical English words of special interest in the current context.1 One, and the most recent, is opioid. The others are narcotic, drug, opiate, morphine and heroin. All were originally medical and pharmacological terms, descriptive, denotative and professional. Their connotative load was if anything positive, as for a therapeutically effective medication. Examples include, ‘Boetius holds it to be a good narcotick, and that it safely may be given to procure sleep’. (1677),10 and ‘The whole art and mystery of opium-taking’ in De Quincey’s Confessions of an English Opium-eater.11
In order to reveal the current standing of these terms in relation to their medical and addictive meanings, we list their definitions in five representative current dictionaries, one British, two American and two Australian: Lexico.com, an English dictionary (online, British)37 Thefreedictionary, a large English dictionary (online, American)38 Merriam-Webster, an English dictionary: (online, American)39 Australian Oxford Dictionary (hardcopy, Australian)40 Macquarie Dictionary (hardcopy, Australian)41
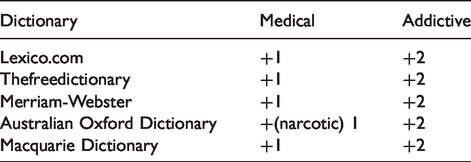
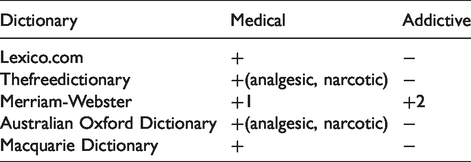
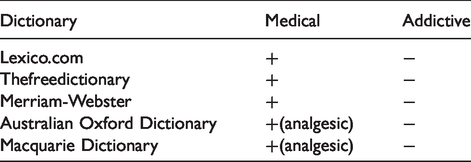
Dictionaries by convention list the most common current meanings first, and other meanings in decreasing order of frequency and prominence. Our goal here is to investigate whether there is any pattern in the relative ranking of medical/pharmaceutical versus addictive meanings, bearing in mind that all these terms were originally medical definitions relating to pharmacology and physiology. In the tables that follow ‘+’ indicates that there is a dictionary listing under a given category, ‘−’ that there is no listing, and ‘1’ and ‘2’ show whether a given meaning is given first place (and so is a preferred reading) or second (ranked below ‘1’).
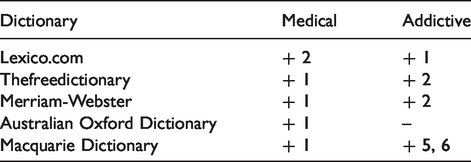
Meaning: Originally, a drug inducing drowsiness, stupor or insensibility. But nowadays the most common non-technical meaning is of an addictive drug, especially illegal, affecting mood and behaviour. Extensively used illegally.
Meaning: A medication to treat disease, but also one that can affect a living organism and induce addiction. In the USA, drug is commonly used for medication, and there is the standard term drugstore for which Commonwealth countries prefer pharmacy or chemist/chemist’s. In the USA, drug also means a medication or an addictive substance with narcotic or stimulant effects (to be on drugs). In Commonwealth countries the earlier meaning of drug involved the addictive substance, but the American pharmacological sense is now increasing strongly.
Meaning: A substance naturally derived from opium or related to it, and used medically for the relief of pain or for its soporific properties. Opiate has preserved its medical use better than opioid. It is also used metaphorically to denote something that induces a false sense of contentment, as in Karl Marx’s famous Opium des Volks, translated into English in the famous phrase ‘[religion is the] opiate of the masses’.
Meaning: Medicine, narcotic analgesic, but can create dependency. Laudanum is a tincture of morphine in alcohol (Paracelsus, 16c). Like opiate, it has preserved its medical meaning better than the other four terms.
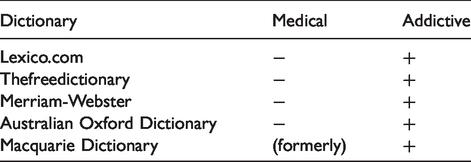
Meaning: First marketed by the German pharmaceutical company Bayer in 1895 as a non-addictive cough suppressant, and as an alternative to morphine. The name was chosen because heroin made one feel heroic (German heroisch). The addictive properties of heroin soon became evident, and its medical use is now less common, except in the UK. The word is now used almost exclusively to refer to a drug of addiction.
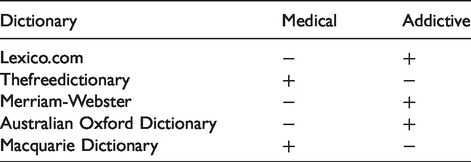
Meaning: A substance like opium: -oid is a suffix meaning ‘similar to or having the properties of’ – see words like ovoid ‘similar to a round object’. Opioids have a similar molecular structure to opium and bind to similar receptors. The word opioid is often used loosely in a way that is more or less coterminous with drug.
These definition profiles across the five dictionaries allow us to establish a ranking of the six terms between medical and addictive definitions, bearing in mind that all six terms were originally medical in nature. In addition, it is important to remember that dictionaries are descriptive instruments. They describe current usage, though people often use dictionaries in prescriptive (what you should say and write) and proscriptive (what you should not) ways. There is an inevitable delay as dictionaries track changes in usage, and incorporate into their consolidated listings the changes that have shown themselves to be clearly established.
Morphine and opiate are strongly medical in usage. They are less frequent than the other words, principally by virtue of being primarily restricted to medical and professional use. At the other end of the spectrum is heroin, once marketed as a medicine but now virtually only used as a substance of addiction. Drug is a difficult word. It uncomfortably straddles both meanings, with its medical sense doubtless reinforced by its use in this sense in the USA, including the common term drugstore. The middle ground in terms of medical/addictive use is occupied by opioid and narcotic. Of these, narcotic has been almost completely taken over by the addiction sense. Opioid is in transition from the medical towards the addiction sense. We will argue below, on the basis of textual evidence, that the ‘addiction’ sense of opioid is already dominant. And because of the key position of opioid in the current debate on OUD, these changes have important consequences for the ways in which opioids can and are being used, and the question of what steps should be taken to combat this.
Opioid: lexical properties and usage
This brings us to the word opioid. It is related to the word opium, and the suffix -oid denotes form or resemblance. As we have seen, the original denotation of opioid is uncontroversial. It is an artificially synthesised chemical that resembles opium in its pharmaceutical, physiological or addictive effects. Opium has been known as a narcotic for seven millennia. In this medical and pharmacological use opioid had rather few connotations. Current English shows some neutral collocations like administer opioids, and even some positive ones like medical benefits of opioids. But opioid has a second and compromised side involving its addictive properties. For much of its history the medical use of opioids was not substantially contaminated by their social and socio-psychological use as an addictive drug. Morphine (the name derives from the Greek god Morpheus, the god of dreams and sleep) was used medically as a valuable analgesic and soporific. Heroin (see above) was so named because it made one feel like a hero. Opioids are narcotic, in the technical sense of numbness-producing, derived from the Greek medical word narkotikos from the verb narkoun ‘make numb’. But as we have seen, the word narcotic has now acquired the primary meaning of an addictive drug affecting moods and behaviour, and this association with drugs of addiction tends to muddy the discussion and public rhetoric about opioids and the term opioid. It also works to complicate and confuse discussions at all levels about the nature and role of opioids in medical practice and the treatment of pain.
Indeed, a number of terms relating to OUD are not well understood by people outside the ranks of medical professionals. Opiate and opioid are commonly used, especially in the popular and social media, in a roughly interchangeable way, although as we have seen, opiate has a strictly medical sense in the dictionaries. Three other terms that are confused are tolerance, dependence and addiction (see above). The terminology in this area has been regulated for professional use by the American Psychiatric Association’s DSM-536. As stated, the terms substance abuse and substance dependence were replaced by the less pejorative substance use disorder, which is now the recommended term for addiction. In earlier editions of the DSM, abuse was less severe, and dependence covered more severe levels of addiction. The move away from using addiction in favour of disorder was intended to reduce the stigma (see below) attached to people dependent on addictive substances and in need of help. Substance use disorder is now graded from mild to severe. Unfortunately, neither the clarity nor the compassionate connotations of this change have so far shown a coherent impact on general usage.
And finally, as I have heard from a number of practising pain physicians, the word painkiller is itself misleading. Patients—and many in the general public— take ‘killer’ to imply ‘removal’. This is often not possible, especially with CNCP, where multiple causes and histories mean that the best outcome that can be hoped for is containment, reduction and management of pain. Painkiller, ranked the #13,626th most common word in English in the 10-billion-word iWeb corpus,40 has only two pejorative terms in the 20 most commonly associated themes (overdose, abuse). Its overwhelming use is medical. But it does contribute to patient expectations in ways that can be counter-productive. Something like pain management medication would be preferable, but the established position of painkiller in the advertising wing of pharmaceuticals makes this unlikely.
The language of the opioid ‘epidemic’
This ‘epidemic’ status of opioid and opioids has been accompanied by a strong developing upsurge in negative connotations around both the word opioid and the discourses where it appears. We can investigate these features through raw counts of words and word combinations from the very large text databases of English that are maintained at Brigham Young University in Utah:42 GloWeB: 1.9 billion words, 1.8 million web pages, 340,000 websites, 20 different English-speaking countries iWeb: 10.6 billion words of web news since 2010 NOW: 12.3 billion words of journalistic English from the web.
With data sources as large as these we can be reasonably confident that skewing effects related to sample selection and distribution will be minimised. The different databases offer different analytical tools, which we use selectively for the purposes of the present analysis.
The NOW dataset, taken from web-accessible journalism, shows that the word opioid has exhibited an intriguing profile over the last decade. We can plot the number of times opioid was used, which gives an indicative measure of the relative profile in public discourse. But since these numbers could simply be the result of larger corpora (and more text being collected), the words per million metric is a valuable additional means of estimating the density of citations of opioid in the data.
From 2011 to 2014 opioid was in a broadly steady state. In 2015 it began a sudden upswing, which gathered pace until 2019. The use of opioid increased more than 20-fold between 2014 and 2019. Although the words per million number is not as dramatic, it also shows a significant increase of approximately five-fold: people were writing a great deal more about opioids (Table 1).
Incidence of the word opioid from 2010 to 2020.
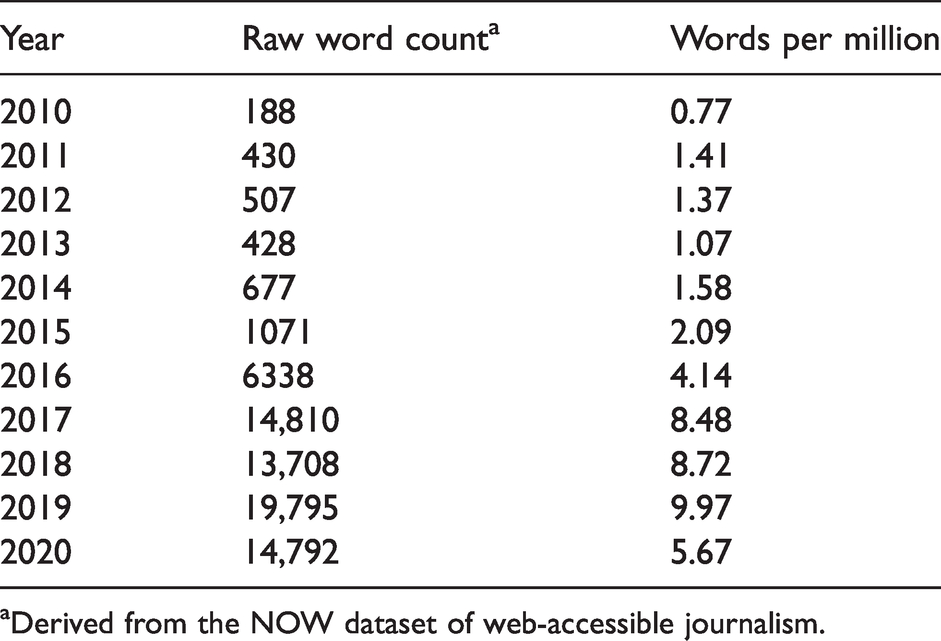
aDerived from the NOW dataset of web-accessible journalism.
Let us concentrate first on what happened up to and including 2019. It is not difficult, using key public pronouncements about opioid, to assemble convincing evidence for the increasingly pejorative and negative tone of the texts in which opioid is used from the NOW dataset. The software allows us to ask what are the most common words (‘collocates’) that occur most often with opioid, including four words to the left and four words to the right of opioid:
crisis, epidemic, addiction, overdose, use, overdoses, abuse, treatment, deaths, prescription, fentanyl, drug, synthetic, pain, prescriptions, painkillers, disorder, drugs, heroin, prescribing, powerful, died, medication, address, fight, dependence, combat.
he discovered that the connections between the patients’ prefrontal lobes and their opioid systems had been damaged (Wired.com, 24 August, 2009). marketing trumped science and helped fuel the rapid increase in opioid use throughout the country (Healthnewsreview.org, 11 September, 2012). world's wealthiest country, the United States, faces an epidemic of suicide and opioid addiction – clear symptoms of rising unhappiness (newsroom.co.nz, 20 July, 2020). Although it’s rare in Canada to charge dealers with killing customers, the number of cases is increasing due to the opioid epidemic. Murder charges are much more common in the United States (https://www.cbc.ca/news/canada/london/london-ontairo-fentanyl-should-dealers-be-charged-with-manslaughter-1.5120166; 3 May, 2019). Struggling parents, domestic violence survivors, opioid users, and individuals with mental illness are hauled off to jail without treatment or assistance (https://slate.com/news-and-politics/2020/07/the-case-for-elizabeth-warren-for-vp.html, 10 July, 2020).
From 2020, however, there is a significant change: opioid has declined appreciably by around 25% in total citations. The words per million scores have proportionately declined even more by approximately 43%, showing a lower density of discussion of opioids in the journalistic space. One factor may be that the White House’s SUPPORT and STOP initiatives may be working, since prescriptions for opioids have declined by 16% in the USA, though doctors and dentists are still writing more opioid prescriptions than in the 1990s.43 One obvious major player in this decline in the profile of opioid discussion is Coronavirus, with virtually zero presence before 2020 and a hugely dominant presence throughout the year, with 1,942,095 citations and a per million words score of 744.71. There is, however, little evidence that the edginess has gone out of the opioid debate.
Implications for clinical practice and public health
The word opioid has therefore undergone substantial semantic modification and pejoration, especially since the middle of the last century. These compromised areas of communication primarily concern prescribing physicians and people in pain. Many of these problems are already being addressed by caring, compassionate health physicians and cooperative patients, working together in a ‘therapeutic alliance’. But it is worth setting out in more detail some of the desired parameters for effective pain communication involving opioids.
First, if we agree that a more dispassionate tenor of discourse on opioids is desirable, it is necessary to moderate the current demonisation of opioids, while not discounting the dangerous effects of their use and misuse. This means counter-balancing the misinformation, stigma, rhetoric, rumour, taboo, shame, and embarrassment often associated with attitudes to opioids and discussions about them.
A related issue concerns placebos. There is already substantial experimental evidence of the efficacy of the placebo effect, though its actual mechanisms of operation are still being worked out. Part of the emotional domain of placebos has to do with the role of patient expectations.44 As I have argued,45 it is necessary to distinguish three kinds of placebo: Placebo1, the traditional ineffective medicine given in the hope that the patient’s belief will be therapeutically effective; Placebo2, an inert medication used in randomised trials; Placebo3, as part of caring interactions in routine clinical care.
If the placebo effect is to be allowed to work, it is necessary to address the stigma associated with opioids—in the spirit and actions of the DSM-5.36 The theme of working on alleviating the stigma associated with opioids has already surfaced explicitly in a number of places. Carter and Battaglino note that 47,000 died in the USA from opioid overdose in 2017 alone,52 and that only two out of ten seeking OUD treatment could access it when they needed it. Women, with their heavier pain load than men,53,54 are more likely to be prescribed opioids. Olsen and Sharfstein identify four areas where people seeking treatment for OUD are disadvantaged by stigma;55
OUD is seen not as a medical illness but as the consequence of moral weakness or willful choice; separating OUD treatment from the rest of health care can deflect the attention of the treating physician from other mental and physical conditions; language use: urine tests are ‘clean’ or ‘dirty’, as are patients; patients seeking to wind back their opioid use are described as ‘detoxifying’; people with OUD are called ‘junkies’; the criminal justice system often disallows access to methadone or buprenorphine as part of patients reducing their reliance on opioids.
These and other issues are addressed in the report of the American Medical Association’s Opioid Task Force,56,57 ‘The key to recovery is support and compassion. Patients in pain and patients with a substance use disorder need comprehensive treatment, not judgment’.56
And as Perry et al. report from a national survey58 while Americans do not consider OUD prescription disorder holders responsible for their addiction, they do subject them to social exclusion, including from jobs. And there is a washback effect from illegal or overuse patients to the clinical context, where bona fide doctors and patients are trying to achieve empathy and responsible strategies to address pain.
In this context, is it possible to talk about opioids in an objective and enabling light? First, and especially in public debate, it is necessary to modify the nexus between opioid and terms like addiction and epidemic. In the NOW corpus the co-occurrence of the word opioid with a non-negative term like benefit is 29. The corresponding figure for opioid and epidemic is 7495. This has an inevitable flow-on effect to the tenor of public discourse about opioids, and to medical consultations, where it must currently be difficult to talk carefully through concepts like dependence, tolerance and addiction—which are still very current, in spite of the advocacy in favour of substance use disorder from the DSM-5.36 It could be helpful, for instance, if opioid had a status that picked up some of the properties of a term like alcohol, which is accepted as a social practice, but which, when abused, also has widely recognised negative medical, social, psychological, and economic consequences. In the conversations between healthcare professionals and patients during medical consultations, in the follow-up procedures, in responses to people with opioid problems seeking help from addiction hotlines, can it be possible to talk about opioids in terms of chemical substances and their interactions with physical, neurological, and psychological factors, and in terms that are not de facto prejudicial or damning?
Dissension in the medical profession
Establishing a more dispassionate baseline for discussion about opioids and their place in pain medicine may of itself be insufficient, as is demonstrated by a bitter recent interchange between pain physicians and patients in the professional literature.
In 2015 two pain specialists, Professor Jane Ballantyne and Dr Mark Sullivan, from the University of Washington’s School of Medicine, published a paper entitled ‘Intensity of CNCP – the wrong metric?’ in the prestigious New England Journal of Medicine.59 The core of their argument was that evaluating CNCP on quantitative bases, and then treating the pain accordingly with opioids, on the model of opioid use for acute pain and ‘titrate to effect’, was not only failing to provide sustained pain relief, but was also producing patients addicted to opioids. In their view, CNCP is not only nociceptive, rather ‘over time, pain intensity becomes linked less with nociception and more with emotional and psychosocial factors’.
In their view it is therefore necessary to step back from the prescription of opioids, and look for more holistic solutions, certainly including suffering and quality of life rather than just numerical assessments of pain. They conclude that ‘For this purpose, nothing is more revealing or therapeutic than a conversation between a patient and a clinician, which allows the patient to be heard and the clinician to appreciate the patient's experiences and offer empathy, encouragement, mentorship, and hope’.59
There was an immediate and angry response from fellow pain specialists and people living with pain. Some of them even called for Ballantyne and Sullivan to be removed from their university positions, and were severely critical of their professional and ethical position as pain physicians; Ballantyne being President, and Sullivan a board member, of Physicians for Responsible Opioid Prescribing (PROP). One prominent pain physician was quoted as saying ‘To suggest that physicians should no longer treat pain intensity and let patients suffer goes beyond any sort of decency or concern for humanity’.60
This was far from being the end of what became a very public disagreement. Having professional bodies saying different things like this can only muddy the waters of discussion, and for people outside the healthcare domain, must surely be highly confusing.
PROP has advocated that opioids should not be used for long-term pain (Letter from Physicians 2021), and they attack the ‘scourge’ (their word) of the epidemic of opioids and deaths through overdoses from prescription opioids.61
The CDC has been focused more on controlling the epidemic and avoiding the overuse of opioids. Their 2016 Guideline25 included this important paragraph:
Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain. Clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient. If opioids are used, they should be combined with nonpharmacologic therapy and nonopioid pharmacologic therapy, as appropriate.
The situation has been exacerbated by the other epidemic, actually pandemic: Covid-19. Patients have been unable to attend face-to-face consultations with their physicians to ensure continuing supplies of medications. The various regulatory bodies have scrambled to make these requirements more flexible, albeit with delays and again with opposition from PROP.
In addition, all of this has to be managed in the specific topology of medicine in the USA, with the need to synchronise federal and state governments, professional medical bodies, and insurance companies—who are reported to be less ready to go along with policy changes.
Looking back, there are some positive signs. From 2014 to 2019 opioid prescriptions fell by 37.1% in the USA.57 The American Medical Association’s Roadmap reports that from 2015 to 2019 deaths from the misuse of prescription opioids in the USA actually fell slightly, from 12,269 to 11,973. But deaths from the misuse of illegally acquired drugs were ominously gathering pace: fentanyl and derivatives (5,766 rising to 36,705), stimulants like methamphetamines (4,402 to 16,353), cocaine (5,486 to 16,055), and heroin (10,788 to 14,151). The media continue to write about the opioid ‘epidemic’, which is useful as a scare word, but without always separating prescription opioids from illegal opioids. The tone is confrontational, sometimes alarmist. For example, Yerby62 states, This catastrophe has unleashed death and misery across the country for over two decades, yet only recently have policymakers and the public begun to devote attention and greater resources to the problem. Opioid addiction is a terrible and life-threatening burden, one which no one chooses to bear.
Ultimately the common difficulty is the continuing lack of non-addictive pain medications, especially for CNCP. There are some early hopeful indications from EPPIC-Net, the Early Phase Pain Intervention Clinical Network.63 But these medications may take years to reach the market, unless they are propelled by the kind of shared purpose and urgency that accompanied the development of Coronavirus vaccines. That was one area where, at least in terms of the science, there was substantial consensus and sensible reporting. In contrast, the following health policies were mainly disasters of messaging, in different ways in different countries. If ‘disasters’ is apocalyptic, it is also arguably true. And it may well be what is needed to energise public discussion.
Conclusion
Opioids have different roles for different medical conditions. For the short-term relief of severe acute pain, for cancer pain, and for end-of-life pain, opioids administered under close medical supervision have a long and recognised role. Opioids are more controversial for other kinds of pain, especially CNCP. But opioids can unfortunately be misused in pain treatment by healthcare professionals and by patients, and misuse can shift to abuse. And in the domain of recreational drugs, opioid use can become opioid abuse. This has been picked up by a strong public and journalistic pushback against opioids in general over the last decade.
In current usage and in text databases the word opioid is primarily associated with negative terms like epidemic and addiction. But the epidemic of addiction is actually associated with opioid abuse. We tolerate and welcome alcohol, which is also an addictive substance, in our social lives, but we also condemn its abuse. Our language for talking about the different social roles of alcohol is differentiated between accepted behaviour and addiction. We may therefore pose the question: should we be doing the same for opioids?
Footnotes
Author Contribution(s)
Acknowledgements
I warmly acknowledge critical contributions and advice from Meredith Craigie, Susan Evans, Damien Finniss, Laura Hamilton, Helen Keates, Geoffrey Mitchell, Frank New, Graham Rice and Joanna Sussex.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.