
Abstract
Opioid misuse is common, as is opioid agonist treatment of opioid dependence. Almost 3% of Australians and over 3.5% of those living in New Zealand report misuse of analgesics. Over 50,000 Australians receive opioid agonist treatment with methadone or buprenorphine for management of severe opioid use disorder.
The perioperative period is an opportunity to identify pre-existing opioid misuse, and to introduce interventions to reduce the risk of development of opioid use disorder. Challenges of acute perioperative pain management or intensive care management of patients receiving opioid agonist treatment include opioid tolerance and ongoing prescribing of methadone or buprenorphine. There has been some ambiguity about the optimal perioperative management of buprenorphine, a partial agonist at the mu receptor.
In this article, a framework to identify emerging opioid misuse problems, identify risk of overdose and to manage the opioid-dependent patient on opioid agonist treatment perioperatively or in the intensive care unit is provided. Diagnostic criteria and risk stratification criteria are presented. Management strategies include trauma-informed care, care planning and care coordination with community practitioners and opioid agonist treatment providers. Continuing methadone or buprenorphine perioperatively with additional opioid and non-opioid analgesia is generally recommended. Increased opioid agonist treatment doses may be required on discharge. An algorithm for decisions about opioid agonist treatment management in the intensive care unit based on the risks of opioid withdrawal and toxicity is considered. Strategies for managing the opioid-dependent patient who is not in treatment are also discussed.
Keywords
Introduction
As the opioid epidemic has evolved, it has been recognised that opioid use initiated for the management of both chronic and acute pain can lead to long-term problems with misuse.1–3 As a result, postoperative opioid management has become a focus of primary prevention of opioid use disorder (OUD). Identification of patients at risk of developing OUD and modifying opioid exposure while maintaining adequate analgesia are core concepts in this.
In a public health framework, secondary prevention implies early detection of disease such that premorbid functioning can be regained, while tertiary prevention indicates ensuring diagnosis and management such that quality of life can be optimised while living with a disease or disorder. These principles can be applied to OUD: early diagnosis of an emerging OUD or diagnosis of mild OUD would sit within secondary prevention. Tertiary prevention strategies would include diagnosis of a previously unidentified but established OUD to allow intervention to prevent progression and harms. The preoperative assessment and perioperative period provide a unique opportunity for primary, secondary and tertiary prevention of OUD. 4
Many of the challenges of acute pain management in patients with an established OUD relate to opioid tolerance. Opioid agonist treatment (OAT) with methadone or buprenorphine is standard care for opioid dependence. There are higher rates of hospitalisations in people who inject drugs compared to the general population, 5 and as this cohort ages, this will likely increase further. There is therefore a need for increased understanding of the optimal management in the perioperative and critical care settings of opioid-tolerant and opioid-dependent patients.
This article will examine how to identify the patient at risk of developing an OUD and how to identify the patient with an established OUD. The principles of OAT will be discussed, and strategies for managing this patient cohort in the perioperative and critical care setting will be proposed.
There are some inconsistencies in terminology across specialty medical groups used to describe problematic opioid use. The International Classification of Diseases, 11th revision (ICD-11), comprises a large, complex set of combination codes to describe opioid use and its many manifestations, consequences and related conditions. 6 The features of opioid dependence are a compulsion to use opioids, indicated by loss of control over use and priority given to opioid use over other activities. There is continuing use despite harm or negative consequences. Craving to use opioids may also be experienced. There is often tolerance to the effects of opioids, and withdrawal symptoms experienced following cessation or reduction of use. Opioids or similar substances are used repeatedly to prevent or reduce withdrawal symptoms. 6
The ICD-11 codes are broadly in keeping with the clinical definitions and descriptions of the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5). 7 The preferred diagnostic term for problematic opioid use is ‘opioid use disorder’. It is widely agreed that the use of terms such as ‘narcotics’ or ‘drug or narcotic addiction’ is not appropriate in any clinical setting as these terms are value laden and stigmatising. According to DSM-5, the diagnosis of OUD requires a ‘problematic pattern of opioid use leading to clinically significant impairment or distress’. The diagnosis and severity of OUD is determined by the presence of at least two of 11 diagnostic criteria described by the DSM-5 (Figure 1). 7 However, the tolerance and withdrawal criteria are different for patients who are on prescription opioids and taking them as prescribed. If such patients do not meet two or more other criteria, they do not have OUD. In this text, ICD-11 and DSM-5 terminology will be used, with severe OUD (DSM-5) and opioid dependence (ICD-11) being used interchangeably. Substance use disorder (SUD) is an overarching term defined in DSM-5 to indicate a problematic pattern of use of any substance (e.g. tobacco or alcohol). 7
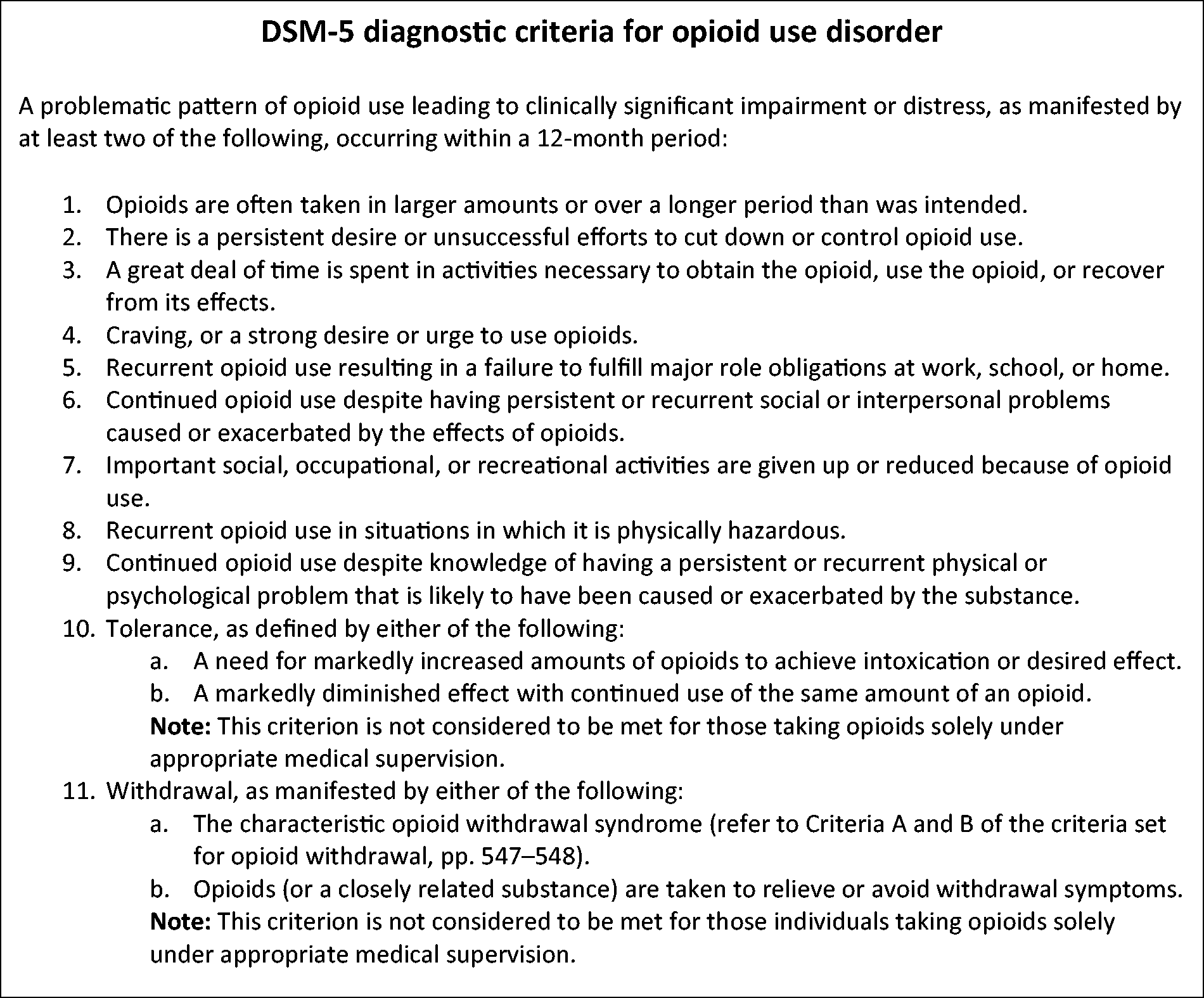
American Psychiatric Association Diagnostic and Statistical Manual V (DSM-5) criteria for opioid use disorder. A score of 2 indicates mild disorder, a score greater than 6 indicates severe disorder. (Reproduced with permission from the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, (Copyright 2013). American Psychiatric Association. All Rights Reserved.) 7
Patient characteristics and treatment structure
Who develops opioid dependence?
Globally, it is estimated that over 26 million people are affected by OUD, with more than 100,000 deaths annually attributed to opioids.8 In 2016, the USA had the highest prevalence of Opioid Use Disorder.8 However, direct comparisons between countries are difficult as different methodologies are used to estimate prevalence.8 In 2019, 2.8% of the Australian population had used analgesics for non-medical purposes.9 There is a paucity of data on the population prevalence of non-medical use of opioids in New Zealand, with the most recent estimate being 3.6% of the adult population.10 The prevalence of opioid use and dependency varies by age and gender. Seventy to 80% of illicit opioid users are men who also comprise the majority of opioid-related overdoses. When it comes to misuse of prescription opioids the gender difference in OUD prevalence tends to disappear. 11
The development of any SUD is generally considered to be an interplay between genetic and environmental factors and drug availability. These relationships hold true for OUD. Genetic factors are thought to contribute a significant proportion of risk for OUD. Candidate genes include those associated with dopamine as this neurotransmitter is central to reward circuitry, opioid receptor polymorphisms and neurotrophic factors. 12 Epigenetic changes are associated with long-term opioid exposure, 13 and emerging data suggest that epigenetic changes can be seen even with short-term opioid exposure. 14 Disruptions in functioning of the glucocorticoid, oxytocin and dopaminergic neuroendocrine systems as a result of poor infant attachment are hypothesised to contribute to the development and intergenerational perpetuation of SUD. 15
An association between adverse childhood experiences, age of opioid initiation, injection and overdose has been demonstrated. 16 Other social and environmental factors include childhood trauma and neglect, permissive parental attitudes, observing others use drugs when a child, as well as peer pressure. 17
In Australasia, people living in socioeconomic disadvantage and those living remotely were more likely to use analgesics non-medically. First Nations People are similarly at greater risk. 9 As they share common risk factors, people with a history of untreated psychiatric illness tend to be over-represented among people with OUD. 18 Opioid exposure and availability impact on the development of opioid misuse. Year 12 school students exposed to opioids perioperatively have a 33% increase in misuse/harms. 19
Who is at risk in the perioperative setting?
As discussed extensively in other articles in this issue, a number of risk factors for developing prolonged opioid use in the context of opioid initiation in the perioperative period are identified. Preoperative opioid use and pre-existing SUD increase the risk. 20 Younger people may have a particular vulnerability, 21 as do those with mental health disorders. 20 As with many health problems, disadvantageous social determinants of health predict increased likelihood of opioid misuse after perioperative use. 17
What is being used?
The National Drug Strategy Household Survey is undertaken in Australia every three years. For a number of years, this survey has included questions on recent and lifetime use of ‘pain-killers/pain-relievers and opioids’. In 2019, 2.8% of the Australian population used analgesics for non-medical purposes. Less than 0.1% of Australians used heroin and over 11% used cannabis over the same time period. 9 There were over five million prescriptions for oxycodone preparations in Australia in the 12 months to June 2019. 22 While oxycodone is the most commonly prescribed opioid in Australia, fentanyl prescribing is also increasing. 23
The proportion of new psychoactive substances (NPSs) that are opioids has increased from 2% to 9% since 2014, with many being highly potent fentanyl analogues. 24 While there are occasional reports of fentanyl analogue use in Australia, 25 rates of detection of fentanyl and its analogues in regular opioid injectors is low. 26
Similarly, in 2019, the illicit drug reporting system (IDRS) identified that only 2% of this population had used NPSs that were opioid mimetic. 27 The IDRS interviews representative samples of people in all jurisdictions in Australia who regularly inject drugs. In contrast to NPSs, around 20% of IDRS interviewees were using non-prescribed morphine and 9% were using non-prescribed fentanyl. Eighteen percent were using non-prescribed pregabalin and one-third were using benzodiazepines. 27
Assessment of OUD
There are multiple tools available to assess the risk of developing dependence prior to initiation of chronic opioid treatment and others for identifying dependence developing during opioid treatment in chronic non-cancer pain. With predictive tools, a history of any SUD and/or significant mental health comorbidity are consistent predictors. The Australian opioid-related behaviours in treatment (ORBIT) scale is a brief 10 item scale which can prompt further exploration for possible OUD in those already using opioids (Figure 2). 28 When making an opioid use diagnosis, there is excellent concordance across ICD-10, ICD-11 and DSM-IVR criteria for dependence when applied to an Australian cohort. 29 DSM-5 classification of moderate and severe SUD concordance was good. It may overestimate dependence at levels of mild OUD. 29
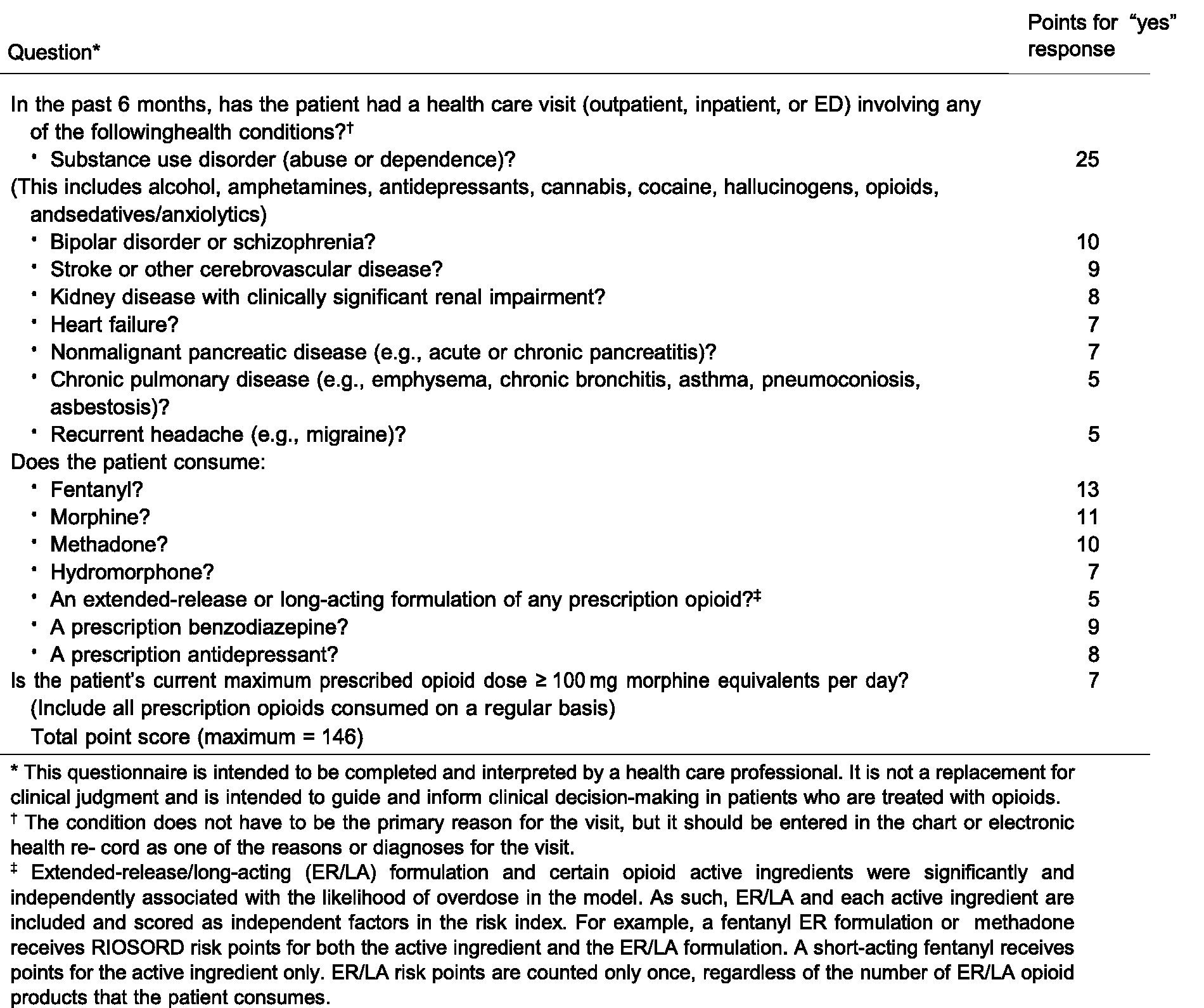
Questions of the risk of serious opioid induced respiratory depression tool which gives a numerical risk score. (Reproduced from Zedler et al., 2018 31 by permission of Oxford University Press.)
Medication reconciliation using real-time prescription monitoring and other electronic health documents can be used to corroborate patient history, as can discussion with community prescribers and pharmacies. 30 In addition to tools predicting the development of OUD, the risk index for overdose or serious opioid-induced respiratory depression (RIOSORD) (Figure 2) is a validated tool that predicts and stratifies risk of overdose by looking at a number of pathophysiological and medication characteristics. 31
What are the harms of OUD?
OUD is associated with a substantial health burden due to the morbidity and mortality related to non-lethal and lethal overdose.5,32 People with OUD have an increased risk of a range of other social and health-related harms, including incarceration, injuries, suicide, homicide and blood-borne virus infections, compared with the general population. 8 The route of administration impacts on harms such as infections related to injection drug use or pulmonary disease related to inhalation. Unsterile drug injecting also increases the risk of a range of other injection-related injuries and diseases such as thrombosis, cellulitis and bacterial endocarditis. 33
In Australia in 2018, opioids were present in nearly two-thirds of drug overdose deaths (64.5% or 1123 deaths) – a rate of 4.6 per 100,000 population. 34 In almost two-thirds (n = 708 deaths) of opioid-induced deaths, benzodiazepines were also present. 34 The majority (80%) of opioid-induced deaths were accidental. The rate of opioid-induced deaths involving synthetic opioids has increased over the past decade. 34
In prescription opioid users, the risk of overdose increases with opioid dose, with one US study showing that those on a 100 mg or more oral morphine equivalent daily dose have a nine-fold increase in risk of overdose compared to those on a 20 mg or less oral morphine equivalent daily dose. 35 Nielsen et al. (2018) demonstrated that in an Australian population of prescription opioid users undergoing OAT with methadone or buprenorphine, 45% had experienced an overdose event. 11 Increasingly, gabapentinoids are identified in post-mortem studies of those dying from opioid overdose. 36 Canadian data identify that co-prescription of either gabapentin or pregabalin with opioid significantly increases the risk of fatal overdose when compared to opioid prescription alone.37,38
Treatment structure in Australia and New Zealand
Although there are some jurisdictional variations in providing OAT, the overarching principles are substitution with long half-life full or partial agonists with supervision of some or all doses of OAT. Psychosocial support is also provided. 39 While treatment is generally initially provided as supervised daily dosing in a clinic or pharmacy, many jurisdictions have provision for takeaway dosing after a period of stability in treatment. 39 Some reductions in this supervision have been adopted during the COVID pandemic to reduce the public health risks. 40 The two medications available for OAT in Australia and New Zealand are methadone and buprenorphine.41,42 Methadone used in OAT is generally oral liquid at 5 mg/ml, although other dilutions are available in New Zealand. Buprenorphine for sublingual dosing is provided as buprenorphine tablets or the abuse-deterrent formulation of buprenorphine/naloxone films. More recently, depot buprenorphine has become available in Australia with weekly or monthly dosing frequencies. 41 At the time of writing, these formulations were not yet listed on the New Zealand pharmaceutical schedule. 42
Regulatory requirements vary across jurisdictions but are broadly similar. Countries sign international treaties, which are enacted at a national or state level. Prescribers should know and adhere to the jurisdictional requirements for controlled substance prescribing. There are often specific additional requirements in OAT programmes.
Who is receiving medication-assisted treatment of opioid dependence?
The Australian 2019 national pharmacotherapy statistics profile of current use as a snapshot on a day in June 2019 showed that almost 51,000 people received OAT, of whom 10% were Aboriginal or Torres Strait Islander, 64% were men and the median age was 43 years. This cohort is ageing. Methadone is the most prescribed OAT in Australia, being used in 61% of patients, the residual being buprenorphine alone or the combination product of buprenorphine with naloxone. Estimates in Australia suggest that only 50% of those who need treatment are receiving OAT. 43
How to manage
Patient approach
Many people with SUD have experienced physical or psychological trauma and adverse childhood events, with very high rates of violence, abuse and neglect. 16 It is useful for the practitioner to recognise that experiencing stressful situations may precipitate maladaptive responses in patients with complex trauma. This can create conflict between patient/family and healthcare providers, and there is a risk of re-traumatising or disengagement.
The role of trauma-informed care (TIC) to improve psychological outcomes has been appreciated in paediatric intensive care units (ICUs) for some time, and there is increasing recognition of the psychological challenges in adult ICUs and the need for strategies to deal with this. 44 It is standard care in psychiatric and addiction services. While there is some emerging literature recognising the importance of this approach, the optimal use of TIC in the perioperative setting is still unclear. 45 Key components of TIC are safety, trustworthiness, choice, collaboration and empowerment and respect for diversity. Approaching the SUD patient in a TIC framework may allow more empathic and collaborative care and reduce conflict between the patient and the caring teams.
There are high rates of social disadvantage in patients receiving OAT, and patients may have limited literacy. This should be considered if providing complex written instructions. Illiteracy can be stigmatising and may not be revealed. 46 Many patients with OUD feel or experience stigma, and this is a barrier to accessing healthcare. 47
Diagnosing OUD in the pre- or perioperative setting
Assessment of preoperative opioid use is the first step in diagnosing OUD. This should be assessed routinely as a component of preadmission questionnaires and in the preoperative assessment. Diagnosis of OUD should be considered if patients give a history of high-dose opioid use. The ORBIT scale is validated in an Australian population and can be used to screen for at-risk behaviour as that might prompt further assessment or referral (Figure 3). 28 Examination identifying signs of intoxication or withdrawal or signs of injecting drug use should prompt further discussion.
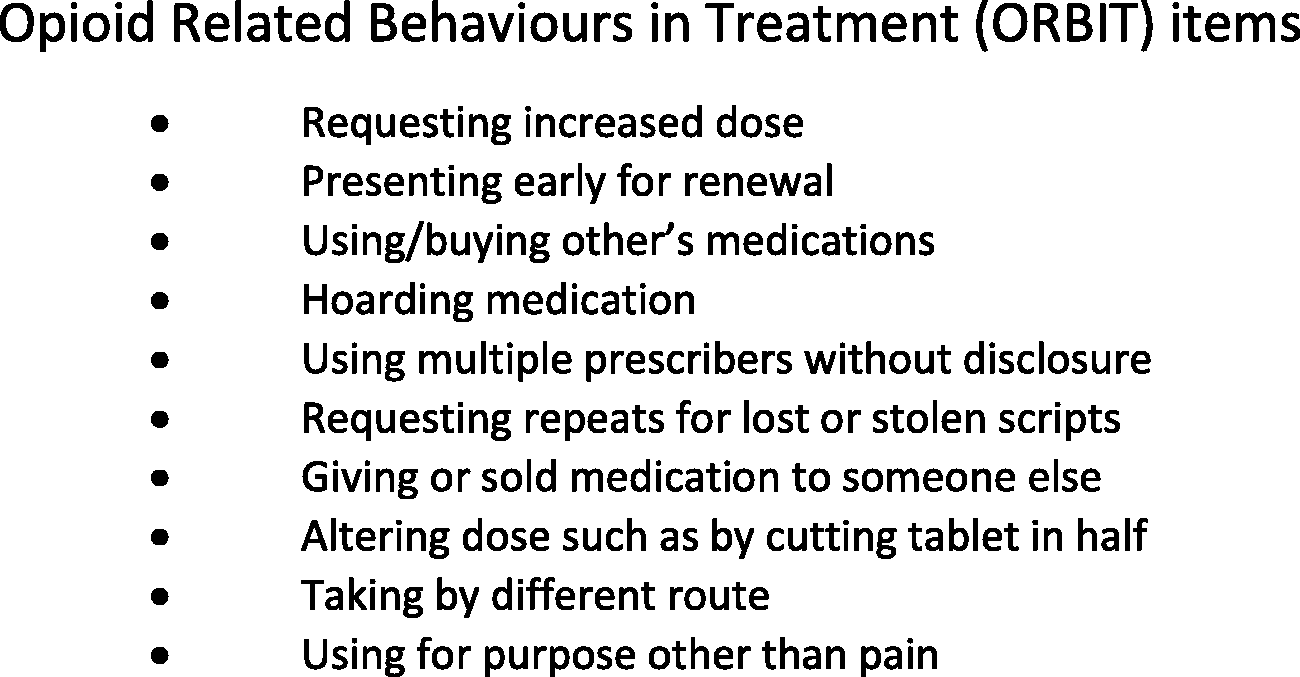
The ten domains assessed in the opioid-related behaviours in treatment (ORBIT) tool (adapted from Larance et al., 2016). 28
Consumption of particularly high doses of opioid postoperatively suggests a need for further assessment of opioid use. High-dose opioid use alone does not meet the criteria for opioid dependence but may be an indicator of risk of progression. Further assessment for dependence includes identification of ICD-116 criteria for dependence or DSM-57 criteria for OUD (Figure 1). Tools such as RIOSORD (Figure 2) may help identify risk of overdose. 31 Communication with community practitioners and referral to drug and alcohol services is necessary if concerns are identified. Each state and territory in Australia has a Drug and Alcohol Specialist Advisory Service which can be consulted (Figure 4).
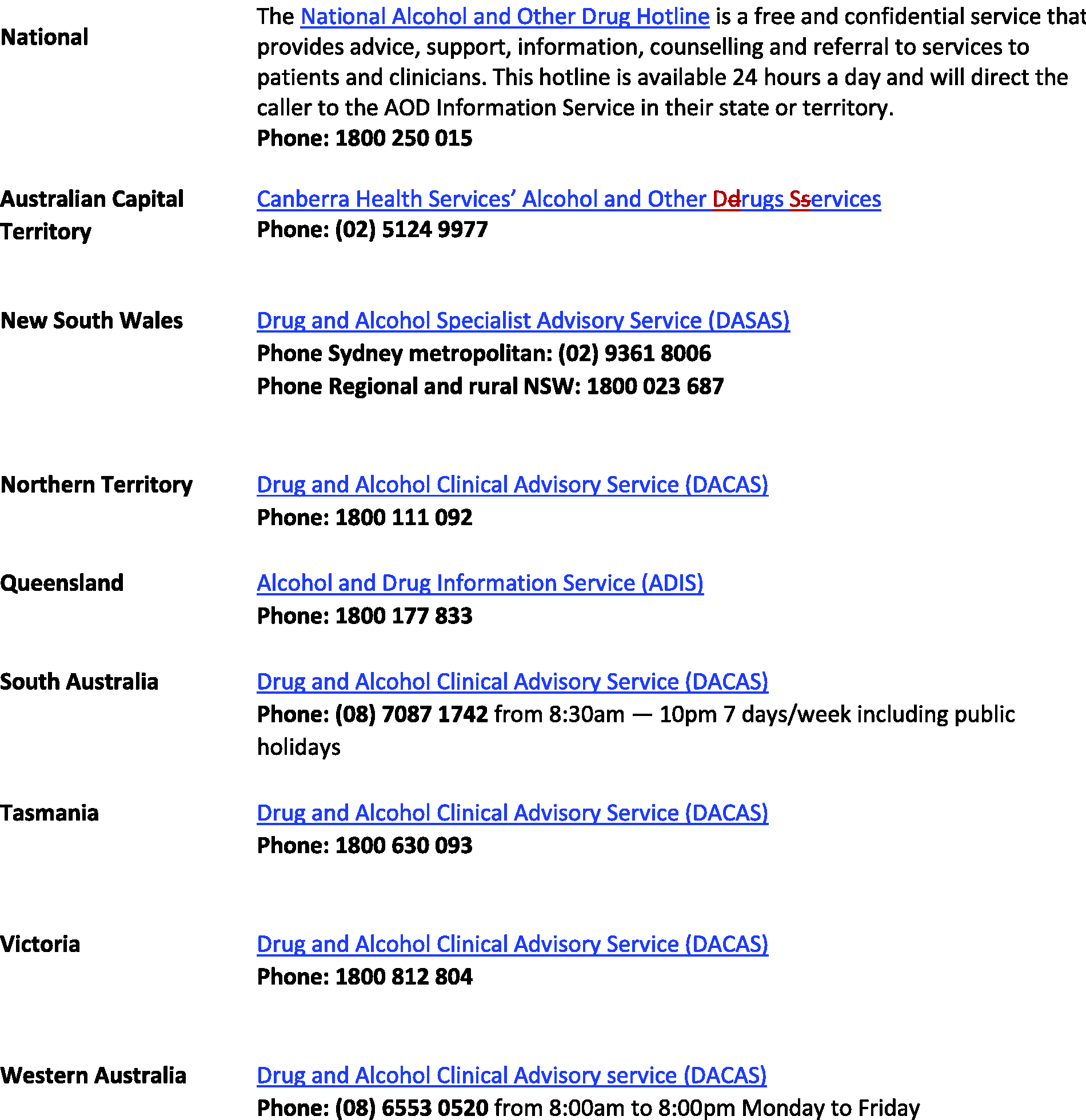
Phone numbers for expert advice in Australia.
OAT medication management perioperatively
There is wide interindividual variability in opioid doses used in OAT. It is recommended that last dose details are confirmed with the dispensing point and/or prescriber. Particular care should be taken to ascertain the number and whereabouts of any takeaway doses that have been provided.
While some authors suggest preoperative opioid dose reduction in patients on long-term opioid treatment 48 there is no evidence indicating that reducing doses of OAT preoperatively in preparation for elective surgery improves outcomes. Dose reduction risks relapse to OUD, and therefore is not recommended. 49 Any consideration of reduction of OAT dose should be undertaken collaboratively with the patient and the community prescriber.
In general, perioperatively, methadone should be continued, non-opioid analgesics initiated and additional full agonist opioid added. 4 Often quite high doses of additional opioid will be needed because of tolerance. 50 Patient-controlled analgesia can be used effectively in people with OUD.4,51
The optimal perioperative management of patients on buprenorphine or buprenorphine/naloxone treatment is more vexed. There is a theoretical concern that buprenorphine’s high affinity but low efficacy at the mu receptor will prevent full agonist opioids being effective. This led to recommendations that buprenorphine be ceased preoperatively and that the elective patient should be transferred to methadone. 52 However, a number of studies have demonstrated benefit in continuing buprenorphine with an additional full agonist opioid such as morphine or fentanyl via patient-controlled analgesia or intermittent bolus being prescribed.50,51 Therefore, the current advice is to continue buprenorphine and add additional full agonist opioid. 52
As with the non opioid-dependent population, there may be a need for a brief period of additional opioid analgesia after discharge. The options are either to increase doses of the usual OAT or use a non-OAT opioid. Discharge planning for community opioid management should consider:
the nature of the surgery and likely need for opioid analgesia after discharge as indicated by opioid use in the day or two pre-discharge; the stability of the patient with regard to their OUD; answers to the first two points above will identify whether additional discharge opioid will be provided as increased OAT or another opioid; how to increase OAT safely: steady state is achieved after three to five half-lives, so methadone safety and efficacy may not be apparent for three to five days; a plan for weaning OAT as the episode of acute pain resolves; the regulatory requirements which may vary with jurisdiction; communication with the patient, the community prescriber and dosing point; whether or not the patient can mobilise to a community dispensing point as there is often a need for frequent pick-ups; if unsupervised take-home doses have been provided preoperatively and the dose has changed in the postoperative period, this should be addressed. This will require communication with the prescriber and dosing point for decisions about provision of new or additional takeaways and destruction of the old takeaway supply.
In general, early planning either during the admission or in the pre-admission clinic will facilitate care transitions.
ICU management
Despite the prevalence of OUD there are limited data to guide the intensivist in managing these patients in the ICU. A 2019 paper identified that few units have guidelines for managing patients with OUD or patients on OAT, although the majority of respondents to this survey, who were predominantly ICU nurses, reported that methadone was continued in ICUs.
53
Therefore our recommendations are empirical. The major considerations are
the clinical situation in terms of the need for sedation/analgesia; the clinical situation in terms of the need for rapid control of level of sedation/respiratory drive; the risks of opioid withdrawal, in particular sympathetic overdrive; the risk of inadequate pain management from opioid withdrawal due to inadequate opioid replacement.
On the basis of the above four points, a decision can be made to continue, reduce or withhold OAT.
In general, the authors recommend continuing OAT. The most recent methadone or buprenorphine dosing details (dose, frequency of dosing and adherence) should be confirmed before prescribing. Decisions about dose reduction or cessation should also be considered in the context of usual ICU practices about whether or not a short half-life parenteral opioid will be used for analgesia/sedation, and the depth of sedation required.
Thus, for example, if a patient has an intracerebral haemorrhage or unstable cardiac rhythm when there are clear clinical reasons to avoid hypertension or tachycardia, minimising opioid withdrawal is judicious. Continuing OAT at its usual dose would be for the most part recommended along with the use of adequate additional opioid for analgesia/sedation. Methadone can be administered orally or parenterally (intramuscular or subcutaneous) with minimal dose adjustment as it has high oral bioavailability. 54 Buprenorphine is administered sublingually daily, and by depot injection weekly or monthly.
In contrast, should a patient be intubated to facilitate management of type 2 respiratory failure in which extubation may be fraught, discontinuing or reducing OAT and temporising with a short half-life opioid may be prudent. These short half-life opioids can be dose adjusted more rapidly to facilitate extubation and maintenance of respiratory effort post-extubation. In fulminant hepatic failure, temporary cessation or dose reduction of OAT is often necessary as hepatic metabolic capacity is impaired and high sedative loads may contribute to encephalopathy.
Recommencing/uptitrating OAT
Consideration should be given to the clinical scenario and ICU opioid exposure when making decisions about dose and timing of the reintroduction of OAT after a period of reduction or cessation. New Zealand and Australian jurisdictional guidelines are broadly in agreement about reinitiating OAT after missed doses and should be consulted when patients have missed doses. For example, when four to five methadone doses have been missed, both NSW and New Zealand guidelines recommend recommencing at 50% of the usual dose and titrating to the usual dose within seven days.55,56
When a patient is sufficiently unwell to require OAT cessation or dose reduction in the ICU, reintroduction of methadone or re-escalation of methadone or buprenorphine dose should be done cautiously with close observation for respiratory or central nervous system depression.
Reintroduction of buprenorphine after a period when full agonist opioids have been used carries the risk of precipitated withdrawal. A pragmatic approach is to transfer from short half-life full agonist opioids only when the clinical situation is stable and the patient can tolerate some increased sympathetic drive as there may be a brief period of symptomatic opioid withdrawal prior to reinduction.
In the situation in which buprenorphine has been ceased and full agonist opioids have been used for a period of time longer than two or three days, reinduction to buprenorphine will probably be necessary. As this is induction from a short half-life full agonist opioid in the inpatient setting, the short half-life opioid can be ceased and the patient observed for opioid withdrawal, which will usually develop in two to three half-lives. The clinical opioid withdrawal scale (COWS) (Figure 5) can be used to assess the severity of withdrawal. 57 Buprenorphine can be introduced when the patient is experiencing mild to moderate withdrawal (COWS of 8) at a dose of 0.2 mg to 2 mg as needed to a maximum of 8 mg to 16 mg on day one. 39 The COWS score should be monitored before and after medicating to ensure there is no worsening of opioid withdrawal that might indicate precipitated withdrawal. The complex and prolonged microdosing regimens that are sometimes recommended for community transfer to buprenorphine have limited supporting data. 58 This may not be necessary when buprenorphine induction is from a short half-life opioid in the inpatient setting where a full agonist opioid can be ceased and buprenorphine reintroduced after two to three half-lives as described above.
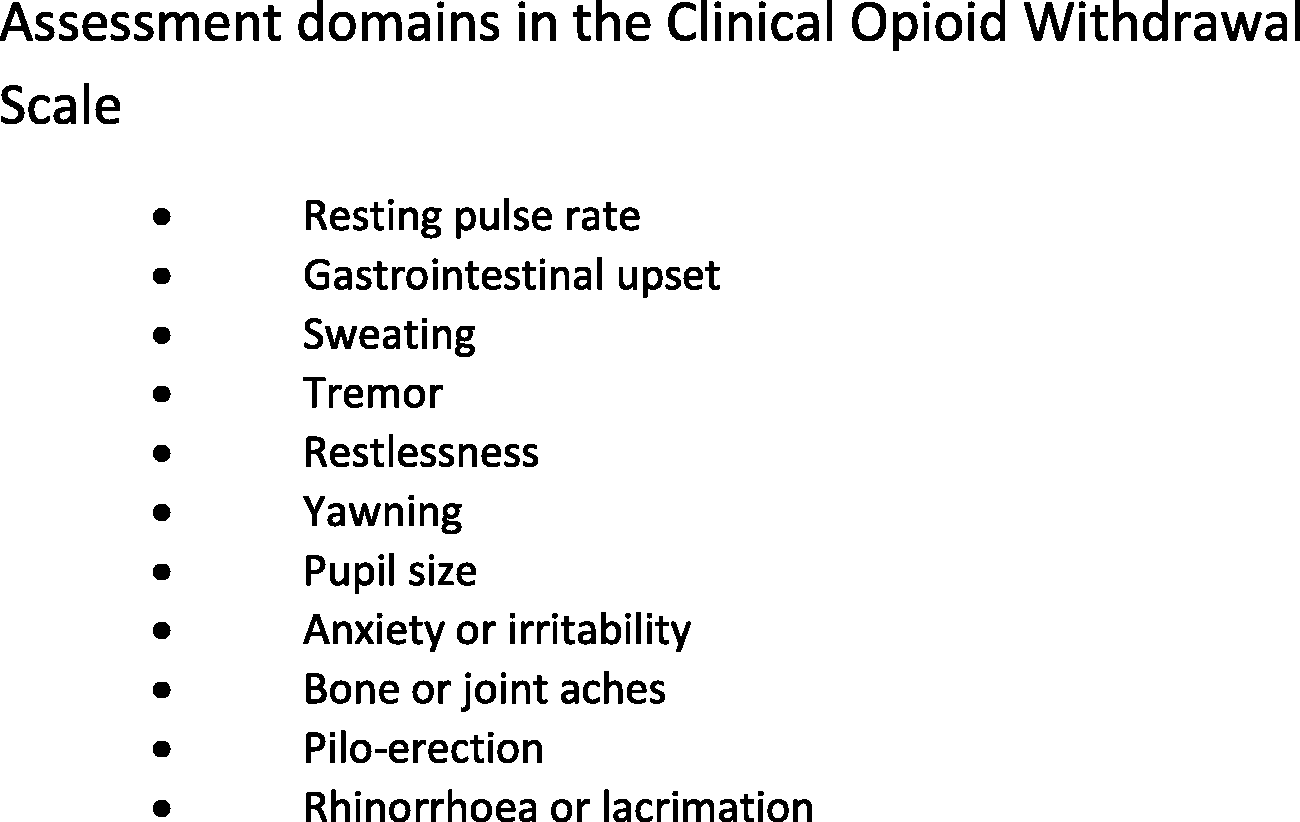
Domains of the clinical opioid withdrawal scale (adapted from Wesson and Ling, 2003). 57
QTc prolongation
Methadone use is associated with QTc prolongation and the development of torsades de pointes in a dose-dependent fashion. 59 Management includes addressing electrolyte abnormalities, identifying and modifying use of other QT-prolonging agents (e.g. tricyclic antidepressants, neuroleptics and macrolide antibiotics) and reduction of methadone dose or rotation to another opioid. 59
Patient with OUD not receiving OAT
For patients not in treatment, the perioperative or ICU setting provides an opportunity to discuss treatment options and link with services. For those who refuse treatment for OUD, inpatient management can be negotiated to balance the needs of inpatient treatment of the pathology causing admission with the need for OUD treatment. For example, a patient admitted for elective or emergency management with unmanaged OUD may not wish to continue on OAT in the long term, but may be happy to accept it while an inpatient. Discharge planning and communicating with community opioid prescribers is clearly critical to optimising treatment. When high-risk opioid use is likely to continue after discharge, naloxone for peer administration should be provided as a harm minimisation strategy. 30 Details of the Australian Take Home Naloxone trial can be found at https://www.health.gov.au/initiatives-and-programs/take-home-naloxone-pilot. 60 In this programme, intranasal or intramuscular naloxone is provided to community members who are likely to witness an opioid overdose, along with education on how to respond to the overdose and administer naloxone.
Patients at risk of developing OUD
This group includes people who fall into high-risk categories, such as young men or those with prior OUD who are now in remission. Discussion with patients about potential risk, and communication of a pain management plan and opioid weaning plans with both patients and community practitioners is recommended as a component of opioid stewardship. 61 Recommendations for monitoring for persistent opioid use or emerging misuse and referral to pain or addiction services should be a component of this plan.
Opioid antagonists
If naloxone is required, over-reversal should be avoided as this can precipitate withdrawal. 53 Precipitated withdrawal is unpleasant for the patient and carries some risk from sympathetic overactivity.
The competitive mu opioid receptor antagonist naltrexone is not subsidised in Australia or New Zealand for the management of OUD, although it is included in US guidelines for OUD treatment. 62 Outcomes with naltrexone are poor. 63 As a competitive agonist, receptor blockade is theoretically surmountable. 64 Practically, however, this means high and variable doses of opioids are probably required. Loss of opioid tolerance and the unpredictable rate of loss of competitive antagonism make this a high overdose risk scenario. Non-opioid analgesic strategies should be maximised, and if opioid analgesia is provided, this should be done with caution and an appropriate level of monitoring in a high dependency unit.
Linking with care
Linking patients to longer-term care is important for the above patient groups. For patients established on OAT, communication with community OAT prescribers, dosing point and general practitioners about pain management plans, opioid management plans and OAT dose changes is necessary.
For patients who have OAT initiated during an acute episode of care, discharge planning should include identifying dosing points, a community prescriber who can comply with the regulatory requirements and communication with general practitioners. For those not wanting to continue with OAT, information about treatment options and available services should be provided.
For at-risk patients, it is particularly important to communicate with community practitioners about pain management plans, the need for reviewing progress with opioids, the likely time frame for opioid cessation and what to do if opioid use persists.
Conclusion
As the rate of OUD in the community increases, it is likely that anaesthetists and intensivists will have greater exposure to this patient group. There are clear opportunities for optimising diagnosis and immediate care and engaging with longer-term treatment. Moreover, there are also opportunities to help prevent the development of OUD in at-risk populations. There is a clear need to improve the evidence base from which we provide treatment for this complex population.