
Abstract
The COVID-19 pandemic has had profound implications for continuing medical education. Travel restrictions, lockdowns and social distancing in an effort to curb spread have meant that medical conferences have been postponed or cancelled. When the Australian and New Zealand College of Anaesthetists made the decision to commit to a fully virtual 2021 Annual Scientific Meeting, the organising committee investigated the viability of presenting a virtual ‘Can’t intubate, can’t oxygenate’ workshop. A workshop was designed comprising a lecture, case scenario discussion and demonstration of emergency front-of-neck access techniques broadcast from a central hub before participants separated into Zoom® (Zoom Video Communications, San Jose, CA, USA) breakout rooms for hands-on practice, guided by facilitators working virtually from their own home studios. Kits containing equipment including a 3D printed larynx, cannula, scalpel and bougie were sent to workshop participants in the weeks before the meeting. Participants were asked to complete pre- and post-workshop surveys. Of 42 participants, 32 responded, with the majority rating the workshop ‘better than expected’. All except two respondents felt the workshop met learning objectives. Themes of positive feedback included being impressed with the airway model, the small group size, content and delivery. Feedback focused on previously unperceived advantages of virtual technical skills workshops, including convenience, equitable access and the reusable airway model. Disadvantages noted by respondents included lack of social interaction, inability to trial more expensive airway equipment, and some limitations of the ability of facilitators to review participants’ technique. Despite limitations, in our experience, virtual workshops can be planned with innovative solutions to deliver technical skills education successfully.
Introduction
The COVID-19 pandemic has disrupted the ongoing education of health professionals globally. Travel restrictions, border closures and lockdowns have made the planning and execution of conferences near impossible, with most being postponed or cancelled.1,2 Preparation for the Australian and New Zealand College of Anaesthetists (ANZCA) Annual Scientific Meeting (ASM) has a long lead time, with planning for the 2021 ASM in Melbourne beginning in June 2019. As preparation was underway, the COVID-19 pandemic unfolded, and the 2020 ASM, in Perth, Western Australia, was cancelled. Uncertainty about the progression of the pandemic meant that the 2021 ASM organisers planned for both virtual and face-to-face programmes. While Australia and New Zealand have fared better than many parts of the world during the pandemic, the shifting landscape regarding snap lockdowns, Australian interstate border restrictions, the potential for an Australian and New Zealand ‘travel bubble’, and vaccination availability led to the decision in October 2020 for a virtual-only ASM.
While most traditional lecture-style presentations have successfully been converted to online platforms as the pandemic has progressed,3,4 smaller group workshops, in particular those concentrating on technical skills training, have met greater hurdles.
The Monash Medical Centre airway group was approached in planning infancy to deliver a version of its ‘Can’t intubate, can’t oxygenate’ (CICO) workshop (comprising pre-reading, lecture and dry- and wet-lab components 5 ) for ASM participants. When it became clear that the ASM would be delivered virtually, organisers and workshop facilitators worked together to plan for a viable virtual CICO workshop. International colleagues with a special interest in airway management were approached to ascertain if anyone had previous experience delivering a virtual workshop, and while one group had experience with a hybrid-style technique, none had delivered a fully online workshop. The major hurdles to providing a virtual CICO workshop were delivering an adequate dry-lab airway kit to participants, the technical requirements to enable clear audiovisual (AV) connections during the session, and meeting strict criteria mandated by the ANZCA to ensure a high-quality and economically viable offering was approved for continuing professional development (CPD) purposes. 6 As there was little international experience to draw on, we report our experience here in the hope that it will help future groups attempting similar ventures.
Preparing for workshop delivery
An inventory of components required for a CICO kit was compiled and sourced from either existing ANZCA stock or new orders via hospital and commercial suppliers. This was based on the exact CICO kit used in all critical care areas across the Monash Health network (a public health network composing of six hospitals in Melbourne’s south-east). Three-dimensional printing of larynxes was undertaken via a commercial printer with specification of a biodegradable plastic made from cornstarch (with prototypes tested to make sure the model was robust). The 3D model used for the larynx was generated from the open-source file available on the Airway App site–an international collaboration that crowdsources data on failed airway events and provides resources for training (www.airwaycollaboration.org%2F3d-cric-trainer-1). 7 With the lower costs of a bulk order, the unit cost was approximately A$16.00.
Wooden bases for the larynx model were prepared by a facilitator with woodworking skills. Kits were assembled and posted out to participants six weeks ahead of the workshop. Appendix 1 shows the components of each CICO kit delivered to participants (Figure 3). Accompanying the CICO kit was an information sheet outlining components included in the pack, along with instructions regarding the virtual setup, recommending a laptop with inbuilt camera elevated on books or a separate webcam connected to a computer to provide a more flexible solution. Further information was given regarding a planned technical check-in time with the conference audiovisual team a week prior to the workshop, with an emailed meeting request sent to participants.
Audiovisual setup
Three separate types of AV setups were required to deliver the workshop: (a) a central studio, (b) a home studio for each facilitator and (c) facilities for each of the participants. The contracted AV company advised on the components and arrangement of each of these.
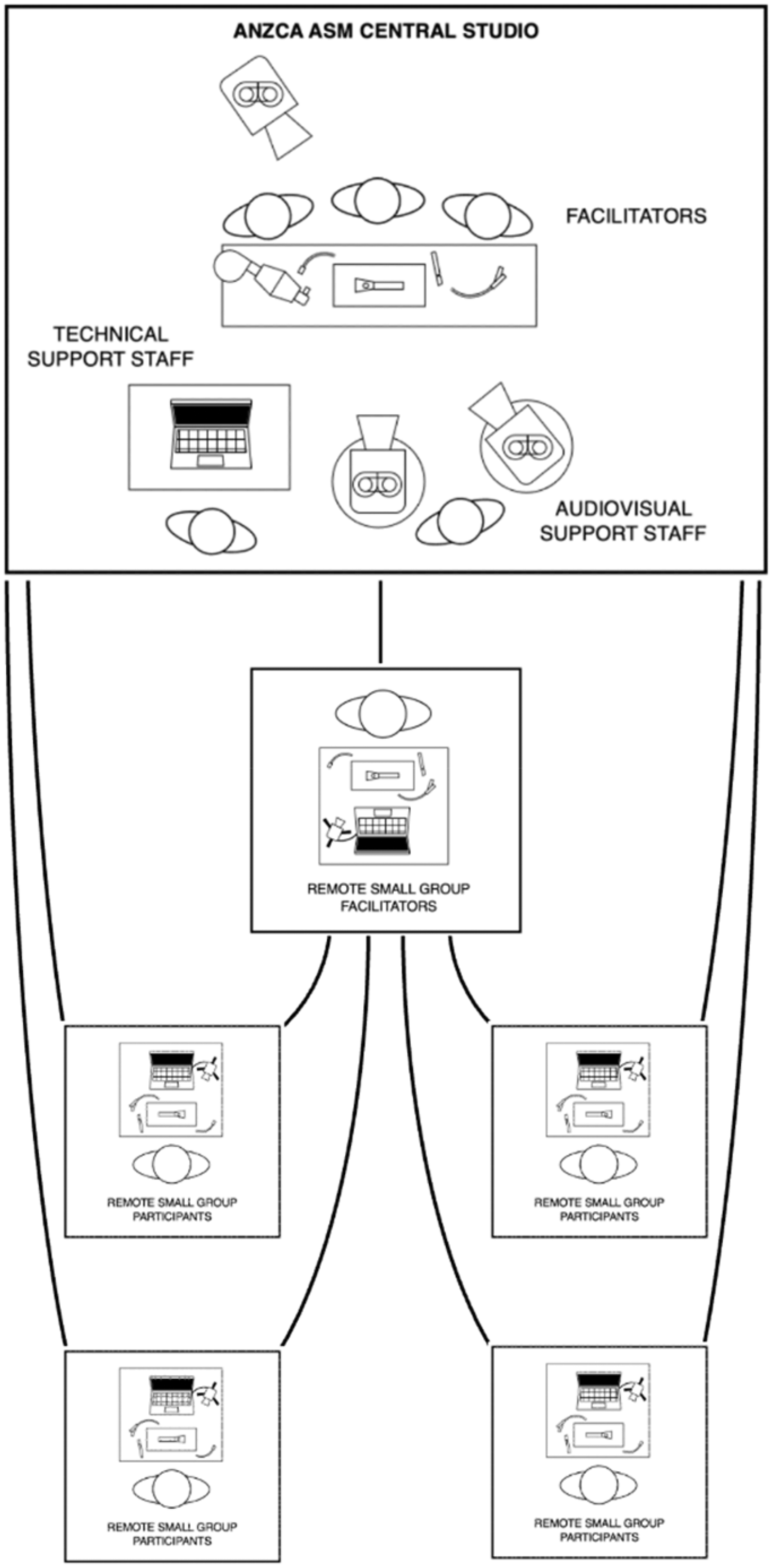
The central studio was assembled at the Melbourne Convention and Exhibition Centre similar to a television studio, with overhead and close-up vision required for the techniques on the airway model. Three podiums accommodated three facilitators with a high-definition overhead camera and two additional pan-tilt-zoom cameras in front of the facilitators (Figure 2). The technicians in the central studio mixed the AV stream for broadcast to the participants and managed the breakout rooms on the videoconferencing platform.
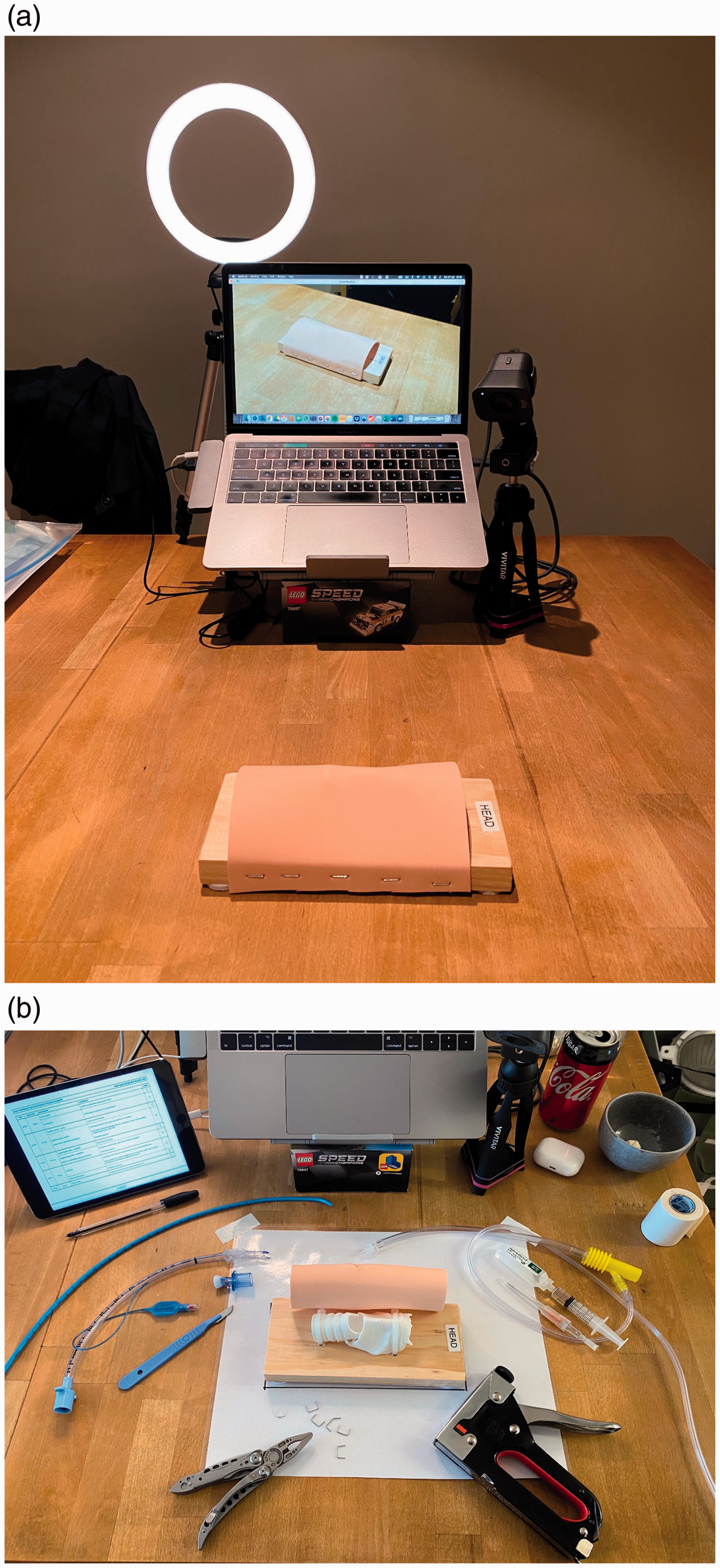
Apart from three of the facilitators in the convention centre studio, a further four facilitators presented material from their own homes. Each home studio for the facilitator was furnished with a similar setup to the participants, with the addition of a studio light, materials to refresh the airway model between sessions and notes for the session as required (Figure 1).
Finally, the participants were requested to attend a videoconference session a week prior and join the workshop 30 minutes in advance in order to guide them as to the best positioning of their cameras, lighting and audio reception by the technicians in the central studio.
Contents of the session
The 48 participants were split into three groups of 16 participants per 90-minute workshop, with three facilitators in the central studio and four facilitators at home in their AV hubs. Each workshop commenced with a live interactive lecture with accompanying PowerPoint presentation delivered from the central hub at the convention centre using the Zoom® (Zoom Video Communications, San Jose, CA, USA) platform. Pauses were allowed for questions from participants (usually raised via the chat function that was scanned by one central facilitator), with a subsequent planned clinical scenario discussion and then a live demonstration of emergency front-of-neck access (eFONA) techniques, including cannula and scalpel-bougie techniques. Multiple camera angles were used throughout this demonstration. Particular emphasis was placed on the pitfalls of each procedure, on the jet oxygenation technique using the Meditech Rapid-O2® (Meditech Systems APAC, Perth, Western Australia) insufflation device (this was delivered as part of the CICO kit with acknowledgement that most participants would not have access to an oxygen cylinder and so could not experience the feedback given if there is obstruction to flow in an inadequately placed cannula), and on the conversion of a cannula to a Melker Emergency Cricothyrotomy Catheter Set (Cook Medical LLC, Bloomington, IN, USA). This was followed by Zoom breakout groups with a maximum of four participants per instructor, facilitated remotely for the hands-on dry-lab component where participants were able to practise their skills under scrutiny. A worksheet for facilitators was developed to check that participants met the requirements for each technique. The last five minutes of the workshop saw all participants return virtually to the central hub for a debriefing session and final question time.
Schematic representation of the cameras and setup for each facilitator and presenter.
(a) Facilitator’s home studio setup for teaching of the workshop, showing ring light, elevated laptop and separate webcam. (b) Facilitator’s home setup for teaching of the workshop with ‘can’t intubate, Can’t oxygenate’ kit components.
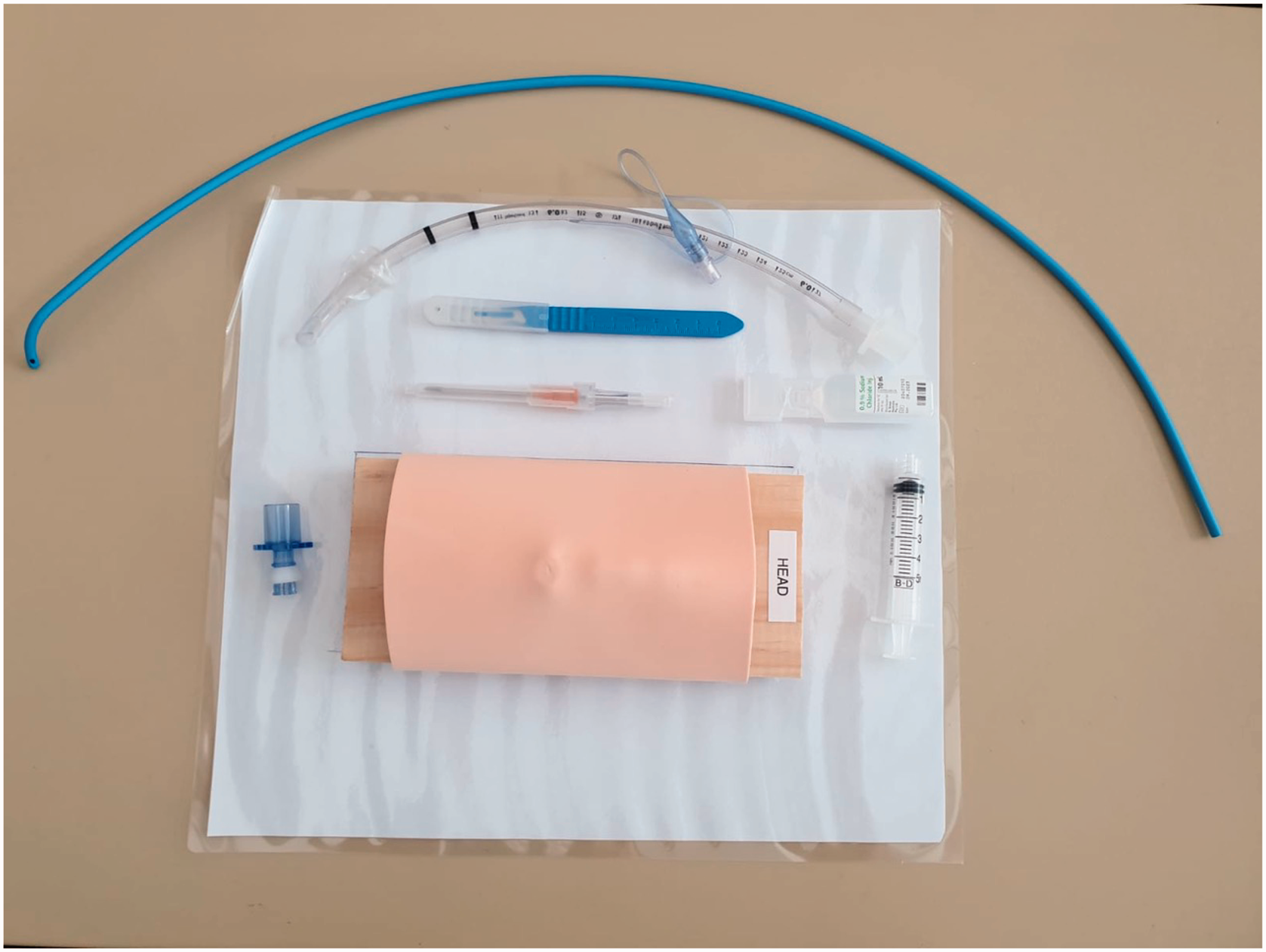
Components of the ‘Can’t intubate, can’t oxygenate’ kit as listed in Appendix 1.
A pre-workshop survey was delivered to participants via email a week before the workshop with a reminder email two days prior, with questions ranging from demographics and AV, internet and equipment setup to participant motivations and expectations of the course. A post-workshop survey was emailed to participants at the conclusion of their workshop with a verbal request to complete, and then a reminder was sent two days later. The post-workshop survey was designed to seek answers to the facilitators’ specific research questions such as whether learning objectives were clearly set out, whether these objectives met, how the workshop compared to participants’ expectations, and whether there were hurdles to the delivery of the workshop (especially logistical). Also sought were further insights into perceived advantages and disadvantages of the workshop and suggestions for improvements for future workshop delivery. As the responses were anonymous, circulated as voluntary and related solely to the conduct of the workshop, this was deemed an education quality assurance activity, and formal approval through an ethics committee was not sought. Surveys are available in the Supplemental Material.
Facilitators’ experience of the workshop
Only 10/48 participants attended the scheduled technical check online a week prior to the event. While participants were given an instruction to log on 30 minutes prior to the starting time, most attendees arrived five minutes before starting. While the central hub AV staff were quick to deal with each attendee as they logged in (often only needing to change an attendee’s camera angle, model orientation or lighting), this did impact workshop starting time and meant a slightly delayed finish.
All breakout room facilitators purchased extra equipment such as high-definition webcams and ring lights prior to the workshop (initially this was not standardised, but after the run-through the evening prior, one facilitator went out to purchase a webcam on noting their setup was inferior). We found the breakout rooms were quickly deployed by the central AV hub team, minimising delays in commencement. Prior to each session, the CICO kit was reset, with new skin surfaces attached using removable staples. A repeat demonstration of each technique was followed by sequential performance by the participants in a random order. The demonstration included commentary on potential pitfalls and strategies to mitigate or overcome these. One benefit found was that remaining participants were able to observe each other’s attempts closely along with the facilitator, reinforcing feedback on the techniques and allowing for further questions and comments based on observed outcomes. While facilitators were initially concerned that correcting technique virtually might be more challenging, asking the participant to slow their actions and talk through each step of each procedure allowed participants’ technique to be clearly demonstrated. Each session involved casual discussion around personal experiences with CICO, and in most of these breakout groups, facilitators found the discussion flowed well. All facilitators reported they encouraged participants to take the workshop’s dry-lab learning further. Discussions included strategies to conduct local CICO training in their workplace using the 3D printed model provided, trialling the supplied Rapid-O2 insufflation device and seeking out higher-fidelity options to cement their learning further. As a result of the initial technical check, most participants were readily prepared to manipulate their webcams and provide satisfactory views to assess their techniques.
The sessions ran reasonably to time, but facilitators noted the Zoom meeting time reminders were often too subtle to note, and a second personal timer was invaluable to keep to time. One breakout room facilitator, who felt their first session overran, contacted participants for a follow-up Zoom session to cover any techniques that felt rushed. Interestingly, another facilitator noted they missed the camaraderie of working with other faculty members and found the facilitator debriefs between sessions important.
Survey responses
Pre-workshop
Of 48 workshop registrants, 34 completed the emailed pre-workshop survey. All respondents practised in anaesthesia (with one also in pain medicine), with 33 consultants and one trainee. Twenty-nine respondents were from Australia, and five were from New Zealand. Only two respondents had not participated in a CICO workshop previously, which reflects the recurrent nature of this training in the continuing education requirements for practice. All respondents had received their workshop kits in the mail at least two weeks prior to the workshop. First impressions of the kit were predominantly positive. Only two respondents had not opened their kit prior to the workshop. Regarding motivation, respondents cited their reasons for registering for the CICO as ‘needing to complete an emergency response for CPD purposes’ (15/34), ‘keeping skills updated’ (16/34) or both (2/34), with one participant wanting to see ‘how it was run as a virtual workshop’. When asked how participants expected a virtual CICO workshop to compare to face-to-face teaching, the majority (25/34) anticipated little difference, three respondents thought it may be better and six thought it was unlikely to be as educational, with common themes being concerns about the potential drawbacks of inability to get good views of facilitator techniques, loss of perceived benefits of face-to-face teaching and more stilted discussion.
Post-workshop
Despite the workshop being over-subscribed with a waiting list, six registrants across the day failed to attend, meaning a total of 42, rather than the 48 expected, took part.
Of 42 participants, 32 (76.2%) completed the emailed post-workshop survey within the week following the workshop. All but two respondents participated in the workshop from home (the others participated from work). All respondents thought the AV quality was adequate for the purposes of the workshop, but one participant was unable to be heard initially, with the central technical staff quick to troubleshoot and resolve this problem. One participant reported an unstable personal internet connection, causing intermittent glitching. The majority of respondents (30/32; 93.8%) felt the equipment provided was adequate for the workshop. One respondent requested a cricothyroidotomy kit to have been incorporated into the mailed CICO kit, but the unit cost of >A$300 precluded this. All respondents reported their models could be used for practice again with extra VBM (VBM, Medizintechnik GmbH, Sulz am Neckar, Germany) skins (a synthetic material ‘skin’ used to overlie the 3D printed larynx). and 30/32 intended to do so. Of the 32 respondents, 30 reported the workshop had prompted them to trial the Rapid-O2 insufflation device provided with the kit connected to oxygen at work.
When asked how the workshop compared to expectations, 22/32 respondents answered ‘better than expected’, 9/32 ‘as expected’ and 1/32 ‘poorer than expected’, but that respondent went on to explain that the small groups worked well. All respondents felt the learning objectives had been clearly set out, but 2/32 felt all objectives had not been met, their main concerns being the inability to trial the Rapid-O2 insufflation device attached to an oxygen source and the lack of access to other pieces of airway equipment. Lack of social interaction was seen as both an advantage and disadvantage by different participants.
The majority of respondents saw some benefits to a workshop in a virtual setting. Convenience, equity of access (for participants who might not ordinarily be able to attend due to distance, work commitments or social circumstances), lack of social interaction, and the ability to reuse the model at a later date were all listed as advantages. Two respondents reported they preferred the virtual format to a face-to-face workshop. The common themes relating to disadvantages seen by participants was their inability to trial more expensive equipment such as the Seldinger technique cricothyroidotomy kit, the inability to trial the Rapid-O2 insufflation device with oxygen, and the potential for more stilted discussion (respondents noted that this did not occur during this particular workshop). Two respondents felt there were limitations in the ability of facilitators in the breakout rooms to review participants’ techniques.
When asked what could have been improved, three participants would have liked more time in the breakout rooms for the hands-on component.
Discussion
This report describes the presentation of a fully virtual workshop for an emergency response activity. Although there is some confusion in terminology, we believe this is the first time a workshop such as this has been attempted with all of the participants and most of the facilitators located remotely, either at home or (for two participants) in a work environment.
Feedback from workshop participants was generally positive, with most respondents saying the workshop had been ‘better than expected’. The 3D printed larynx and airway model components contributed to this positive feedback, along with the physical CICO kit that enables ongoing practice of eFONA technical drills.
The delivery of material from a studio allowed high-quality, high-resolution AV production to be streamed to participants. This ensured the physical skills presented in the workshop were easily explained and demonstrated. While it would be possible to undertake this without a studio, the studio and technical staff ensured that facilitators were much more able to concentrate on the delivery of material without concerns about managing breakout rooms or technical difficulties, or guaranteeing high-quality images and audio were being streamed and received.
Adequate preparation of AV, information technology and technical components was vital to delivering what the participants perceived to be a technically flawless session with no audio or video issues. Poor or inconsistent audio quality has been found to be a drawback of other online medical education events, and we strongly recommend engaging AV technicians and rehearsal to avoid this.8,9 The technical rehearsal the day prior was invaluable to facilitators, with advanced opportunity to communicate with the technical team. The rehearsal allowed improvements to be made to camera angles, lighting, positioning and fixation of the models on the demonstration table, while breakout room facilitators setups could also be checked.
Despite instructions, few registrants attended the online technical check scheduled a week prior to the workshop. In future, we would change the information regarding start time to ensure enough time was left for participants to do a technical check.
When organising an international online conference, Reshef et al. noted challenges ‘related to different emotional engagement due to the lack of in-person interaction’. 8 Our experience mirrors this. Lack of social interaction associated with virtual conference attendance was considered to be both an advantage and a drawback, depending on the participant, which may suggest individuals’ differing learning styles and personality types. Other adjustments need to be made, as the immediacy of feedback from participants to presenters can be lost in a virtual setting (e.g. eye contact, clapping), but we feel adequate preparation, facilitator effort and the small breakout groups allowed participants to engage more fully in these CICO workshops.
One respondent suggested that participants who had personal experience with CICO events (and were happy to discuss these) could submit scenarios prior to the workshop to be included in the clinical scenario section. Workshop participants are always asked about previous CICO personal experience as part of the central session, and this is coordinated into the workshop ‘on the fly’, but a more formalised approach could benefit future workshops.
COVID-19 has had an enormous impact on the healthcare system, changing the fabric of our workplace and patient care, whilst also disrupting continuing medical education (with examinations, conferences, research and clinically based teaching postponed, cancelled or materially altered4,10,11). Whilst delivery of lectures has pivoted relatively easily via online platforms, 12 more needs to be done to facilitate technical skills training 13 and the collaborative interaction that may be lost without face-to-face learning.2,11 Completely halting these components of continuing medical education is untenable. As a profession, we need to be enthusiastic and innovative with our solutions to this problem. In a time of social distancing, our airway group has been heartened by the collegiality and collaboration experienced during the planning and execution of these virtual CICO workshops. Social media has made it easier to reach out to international colleagues and share experiences,14,15 allowing access to open-source materials to enable 3D printing of airway models.
We are mindful of what cannot be delivered in a virtual workshop. There was a limitation to what equipment could be sent to participants, and no-one had access to an oxygen supply at home, but participants were encouraged to use this workshop as a springboard to investigate equipment used at their own health networks. Whilst we had extensive technical backup and good internet connections, we appreciate this might not be the case globally.
Future adaptations of this concept would, of course, involve other technical skills. While the clinical task may be different from the task that is practised at a home workshop, there is evidence that if the components are the same, then skills will be improved. Notably, in surgery, Kneebone et al. 16 used artists and craftsmen such as lacemakers to teach novice surgeons skills such as suturing techniques. While we might not need to go to these extremes, it is clear that analogous practice will result in enhanced confidence and technical ability.
The ability to deliver technical skills workshops remotely also gives rise to opportunities to teach these skills to health professionals in low- and middle-income countries. High-quality videos of the demonstrations can be provided, along with the equipment mailed to their workplace. The only prerequisite would be an adequate internet connection, which may be a hurdle in countries with inadequate infrastructure. 3
In summary, we successfully delivered a virtual technical skills training workshop that met stringent quality standards for CPD. This technique also demonstrates previously unperceived advantages to virtual learning over face-to-face conference attendance, such as improved equity of access.3,17
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X211050937 - Supplemental material for A report on virtual ‘Can’t intubate, can’t oxygenate’ conference workshops at the 2021 Annual Scientific Meeting of the Australian and New Zealand College of Anaesthetists
Supplemental material, sj-pdf-1-aic-10.1177_0310057X211050937 for A report on virtual ‘Can’t intubate, can’t oxygenate’ conference workshops at the 2021 Annual Scientific Meeting of the Australian and New Zealand College of Anaesthetists by in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X211050937 - Supplemental material for A report on virtual ‘Can’t intubate, can’t oxygenate’ conference workshops at the 2021 Annual Scientific Meeting of the Australian and New Zealand College of Anaesthetists
Supplemental material, sj-pdf-2-aic-10.1177_0310057X211050937 for A report on virtual ‘Can’t intubate, can’t oxygenate’ conference workshops at the 2021 Annual Scientific Meeting of the Australian and New Zealand College of Anaesthetists by in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-3-aic-10.1177_0310057X211050937 - Supplemental material for A report on virtual ‘Can’t intubate, can’t oxygenate’ conference workshops at the 2021 Annual Scientific Meeting of the Australian and New Zealand College of Anaesthetists
Supplemental material, sj-pdf-3-aic-10.1177_0310057X211050937 for A report on virtual ‘Can’t intubate, can’t oxygenate’ conference workshops at the 2021 Annual Scientific Meeting of the Australian and New Zealand College of Anaesthetists by in Anaesthesia and Intensive Care
Footnotes
Author Contribution(s)
Acknowledgements
The authors acknowledge and thank Ms Kate Chappell, Senior Event Officer, of ANZCA, for her logistical support for the running of these CICO workshops.
Declaration of conflicting interests
No competing interests declared.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.