
Abstract
Point-of-care ultrasound can be used at the bedside to assess the haemodynamic status and fluid responsiveness of a pregnant woman. Previous studies demonstrated that views from the apical and parasternal windows are readily obtainable in labouring women. However, using the subcostal window to assess the inferior vena cava can be challenging because of the gravid uterus. A potential alternative is the right upper quadrant transhepatic window. We sought to compare visualisation of the inferior vena cava via the subcostal and right upper quadrant windows, in full-term pregnant women. This was a prospective pilot study carried out in a tertiary academic obstetric centre. Thirty pregnant non-labouring women at full term were recruited. In each patient, the inferior vena cava was visualised through both the subcostal and the right upper quadrant windows. Time to acquire each image, acquisition success rates and ease of obtaining images were compared for both approaches. Image quality was then reviewed and rated by two independent expert reviewers. There was a significant difference in the time required to obtain each view; subcostal median (interquartile range): 52 (35–59) seconds, right upper quadrant median (interquartile range): 23 (11–55) seconds (P=0.0045). Operator-defined successful image acquisition was 100% for the right upper quadrant window compared to 80% for the subcostal window. Ease of obtaining the view, as rated by the operator, was significantly easier in the right upper quadrant window compared to the subcostal window (P <0.0001). Both reviewers independently rated image adequacy to be significantly greater in the right upper quadrant window (73% and 57%) compared to the subcostal window (40% and 10%) (P=0.0213 and P=0.0005, respectively). Inter-rater agreement ranged between good (Cohen’s kappa coefficient 0.64) for right upper quadrant windows to fair (Cohen’s kappa coefficient 0.29) for subcostal windows. Inferior vena cava visualisation in term pregnant patients may take less time, be easier and provide better quality images when the right upper quadrant window is used compared to the subcostal window.
Keywords
Introduction
Point-of-care cardiac ultrasound (POCUS) is a non-invasive, safe and expedient modality of cardiac assessment in real time. Despite its demonstrated utility in assessing volume status, cardiac function and valvular pathology, focused transthoracic echocardiography remains mostly underutilised in the obstetric population. 1 POCUS, or more specifically, rapid obstetric screening echocardiography, has been recommended for the assessment of obstetric patients presenting with cardiorespiratory compromise. Patients presenting with dyspnoea and/or hypotension, or patients in whom guidance is needed for fluid management (e.g. haemorrhage or pre-eclampsia) may particularly benefit from this assessment modality. 2
Ultrasonography is ideally suited to guide fluid resuscitation in critically ill patients. A composite assessment of the left ventricle, aortic outflow, inferior vena cava (IVC), right ventricle and lungs can guide fluid management. 3 Static measurements and dynamic variables based on heart–lung interactions can be corroborated to estimate fluid status and assess response to intravenous fluid resuscitation. IVC diameter is one of the parameters used to help with the decisions in fluid management in hypotensive patients. 4 IVC visualisation, however, can be challenging in full-term pregnant women because of the gravid uterus. Apical and parasternal views have been demonstrated to be readily obtainable in labouring parturients, 5 while subcostal views may pose a challenge in the presence of uterine enlargement. 6 , 7 The right upper quadrant (RUQ) window, also known as a transhepatic or mid-axillary window, may therefore offer a viable alternative to the subcostal window for IVC visualisation.
We carried out this prospective single-centre cohort study to assess the feasibility of IVC imaging using the RUQ view. Our primary aim was to compare the RUQ with the subcostal windows in terms of time to obtain an adequate view of the IVC, successful image acquisition, ease of obtaining the view and quality of the acquired image in term, non-labouring haemodynamically stable obstetric patients.
Methods
The Western University Research Ethics Board approved this prospective observational study (approval number 103637), and the study was registered in the ClinicalTrials.gov database before commencing enrolment (NCT02584803). This study was carried out at a tertiary level academic centre. Written informed consent was obtained from all recruited individuals. A convenience sample of non-labouring women with a full-term singleton pregnancy scheduled for elective caesarean delivery or induction of labour were recruited for the study. Patients in labour, less than 18 years old, having multiple gestations, fetal distress, and those who were unable to provide informed consent were excluded from the study. Demographic data collected included age, height, weight, body mass index (BMI), gestational age and American Society of Anesthesiologists (ASA) physical status classification.
Patients were positioned in a semi-sitting position (30° angle) to avoid potential compression of the IVC by the gravid uterus and supine hypotension syndrome. An anaesthesiologist with extensive ultrasound experience, specifically trained in obtaining cardiac images in pregnant women, performed the scans using a SonoSite MicroMaxx phased-array probe, frequency 2–7.5 MHz (SonoSite Inc., Bothell, WA, USA). The RUQ window was obtained first. The probe was initially placed in the mid-axillary line at the level of the ninth or tenth intercostal space, close to the costal margin, and tilted anteriorly to display the long axis of the IVC through the liver (probe index mark directed cephalad). If no view of the IVC was obtained from that position, further back and forth anteroposterior tilting of the probe was undertaken, while maintaining skin contact. If still not visible, the probe was slid anteriorly and cephalad across interspaces until a view of the IVC as it entered the right atrium was obtained (Figure 1). Another investigator witnessed the examination and used a stopwatch to time the acquisition of images. Following the successful acquisition of the RUQ window, the stopwatch was reset and the operator removed the probe. The operator then proceeded to acquire a subcostal view of the IVC again, in a timed fashion. For the subcostal window, the probe was initially placed in the midline immediately caudal to the xiphoid process, also in a longitudinal orientation (index mark directed cephalad). If no view was obtained, the probe was moved slowly or tilted to the patient’s right side until a view of the IVC as it entered the right atrium was visible (Figure 2).
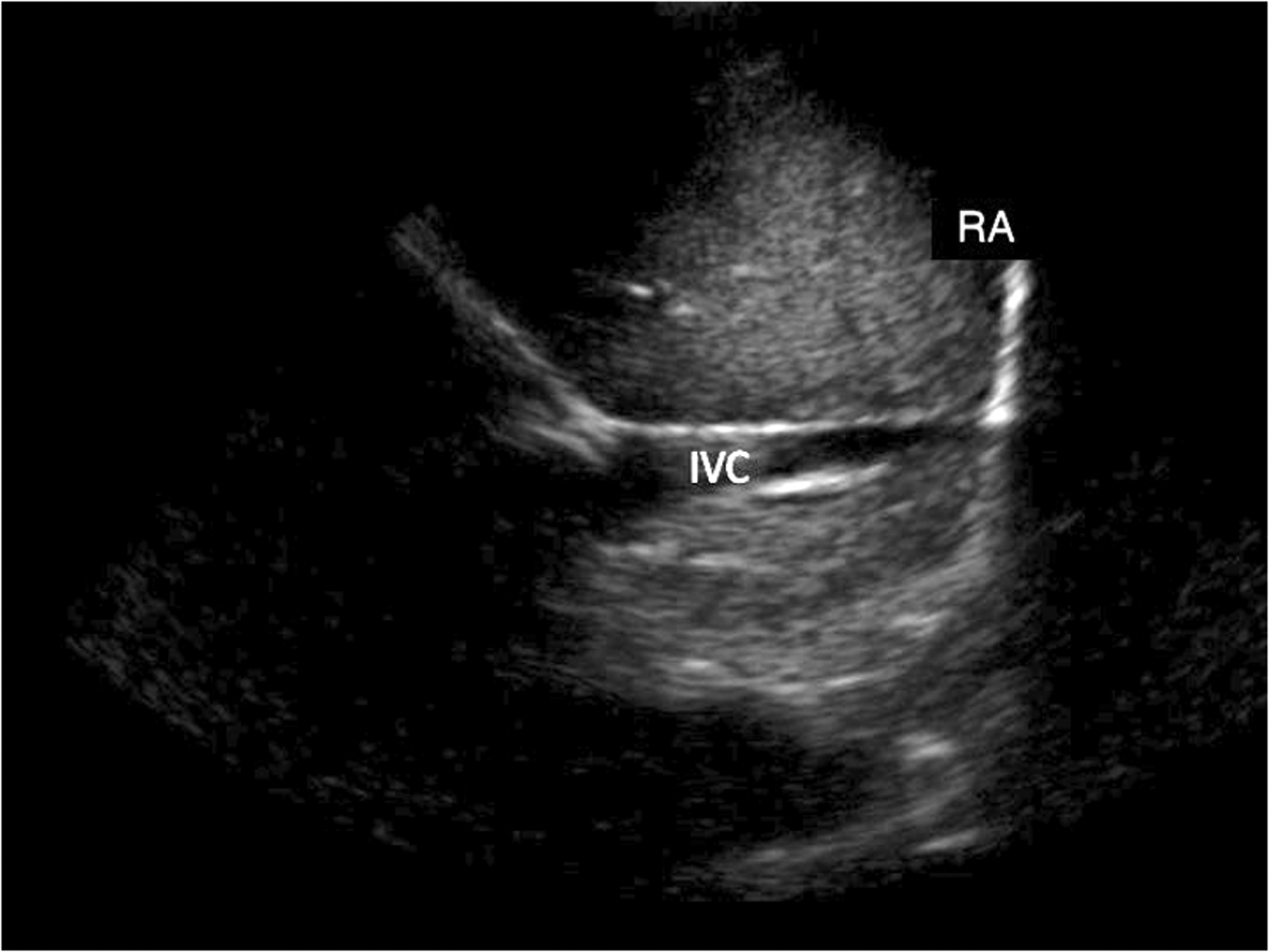
Right upper quadrant window of the inferior vena cava (IVC) as it enters the right atrium (RA) in full-term pregnancy.
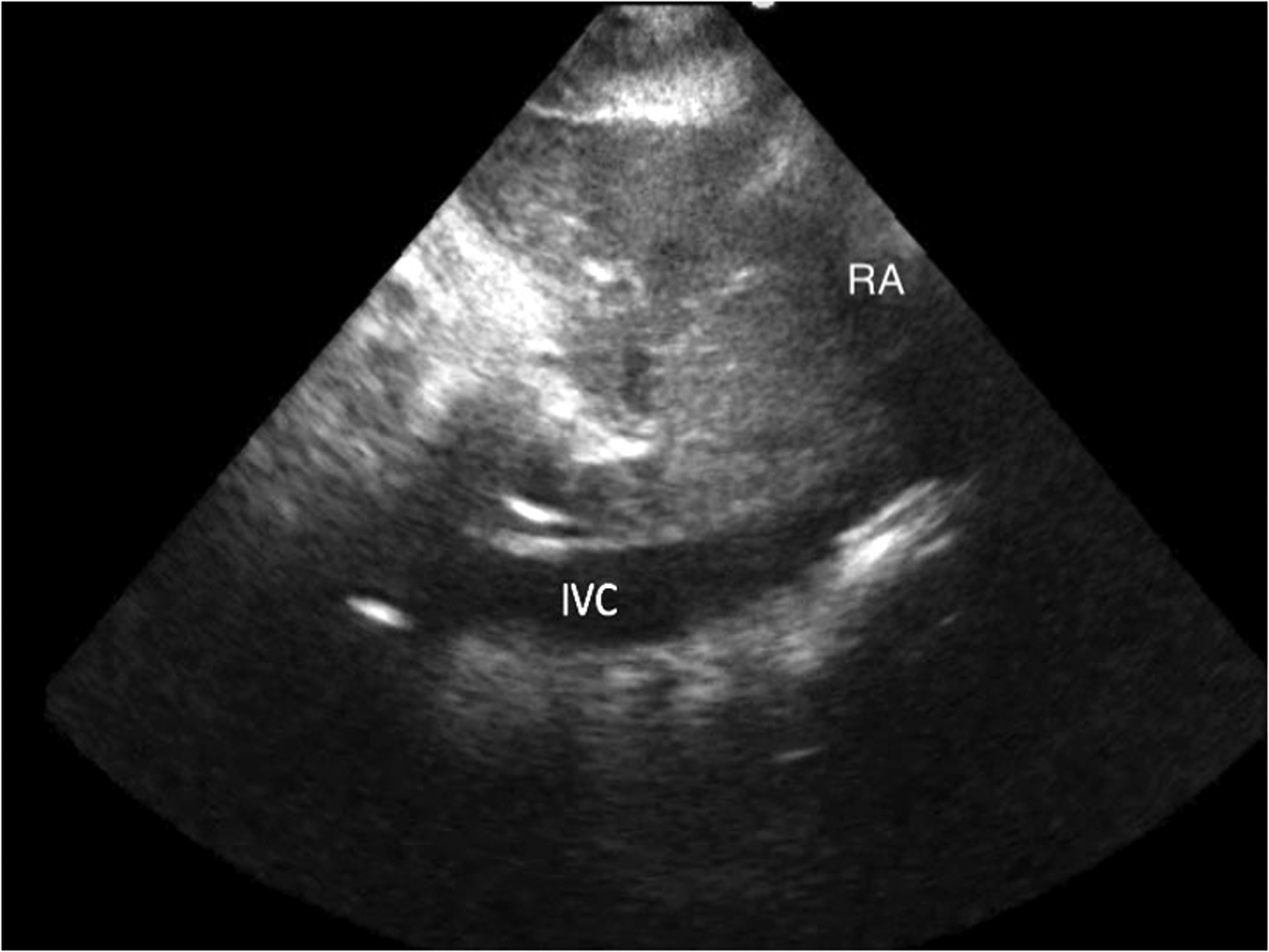
Subcostal window of the inferior vena cava (IVC) as it enters the right atrium (RA) in full-term pregnancy.
The primary outcome was the time required to obtain an image by the operator. If the duration of scanning exceeded ten minutes, the scan was discontinued and labelled as failed. Secondary endpoints included: (a) Ease of exam as rated by the operator: ease of imaging the IVC via both windows was rated on a 5-point Likert scale: (5) very easy, (4) easy, (3) equivocal, (2) difficult, (1) impossible; (b) Success rates for attaining adequate imaging of the IVC from each window, as defined by the operator, and rated as successful or unsuccessful; (c) Image adequacy for both windows.
Each acquired image was independently reviewed by two different investigators (raters), each of whom was blinded to their peer’s assessment. Both reviewers were known experts in the field of point-of-care ultrasound. Images were rated by the reviewers in a binary fashion as adequate or inadequate. The adequacy of an image was defined as the clear demonstration of the IVC lumen with any one of the following: (a) IVC demonstrated to join the right atrium; (b) the hepatic vein demonstrated to join the IVC; or (c) demonstration of a clear intrahepatic course of the IVC lumen. 8
Categorical variables were summarised as frequencies, and continuous variables were summarised depending on their underlying distribution. Normally distributed variables were described as means and standard deviations (SDs) and non-normally distributed variables were described as medians and interquartile ranges (IQRs). The normality of data distribution was assessed by examining its distribution histogram. The study protocol stated that examinations exceeding the ten-minute mark would be aborted and labelled as failed. No scans exceeded ten minutes in duration so none had to be censored. Times to obtaining images were hence compared using a Wilcoxon signed-rank test. Comparisons involving normally distributed variables were undertaken using a paired-sample t-test. McNemar’s test was used for comparing operator-defined success for both windows as well as rater-defined success. Chance-adjusted agreement rates (Cohen’s kappa coefficient) were calculated for image adequacy assessments by the two raters. As per the Landis and Koch cut-off values, a kappa coefficient less than 0 would be taken to indicate no agreement, 0–0.20 as slight, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial and 0.81–1 as excellent. 8 All statistical analysis was performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). A convenience sample size of 30 patients was chosen for this pilot study given that we were assessing the feasibility of using the RUQ window to image the IVC without taking any measurements. 9
Results
Thirty-two patients were approached for this study, of whom two refused to participate. Data from 30 patients were analysed. None of the scans had to be suspended due to patient discomfort. All patients were medically stable at the time of the scan, and most had an ASA physical status of 2 (22 patients). Eight patients were ASA physical status 3, of whom three had gestational diabetes mellitus, three had gestational hypertension and two had pre-eclampsia. Table 1 shows the baseline demographics of the participants.
Patients demographics.
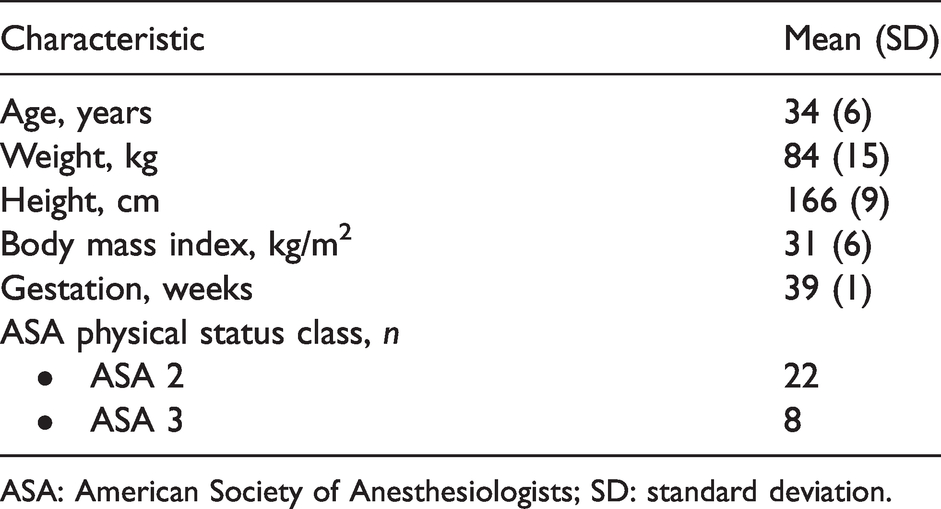
ASA: American Society of Anesthesiologists; SD: standard deviation.
There was a significant difference in the time required to achieve visualisation from the different windows; subcostal median (IQR): 52 (35–59) seconds, RUQ median (IQR): 23 (11–55) seconds (P=0.0045). Also, it was significantly easier to obtain the view via the RUQ window than the subcostal window as per operator assessment, five-point scale mean (SD) 4.0 (1.1) and 2.9 (1.1), respectively (P <0.0001). Operator-defined successful image acquisition was 100% for the RUQ window compared to 80% for the subcostal window. For patients in whom a subcostal window view was not attainable (n=6), no views were saved, and no scan times were recorded. Inter-rater agreement ranged between good (Cohen’s kappa coefficient 0.64) for RUQ windows to fair (Cohen’s kappa coefficient 0.29) for subcostal windows (Table 2).
Comparison of subcostal and right upper quadrant windows.
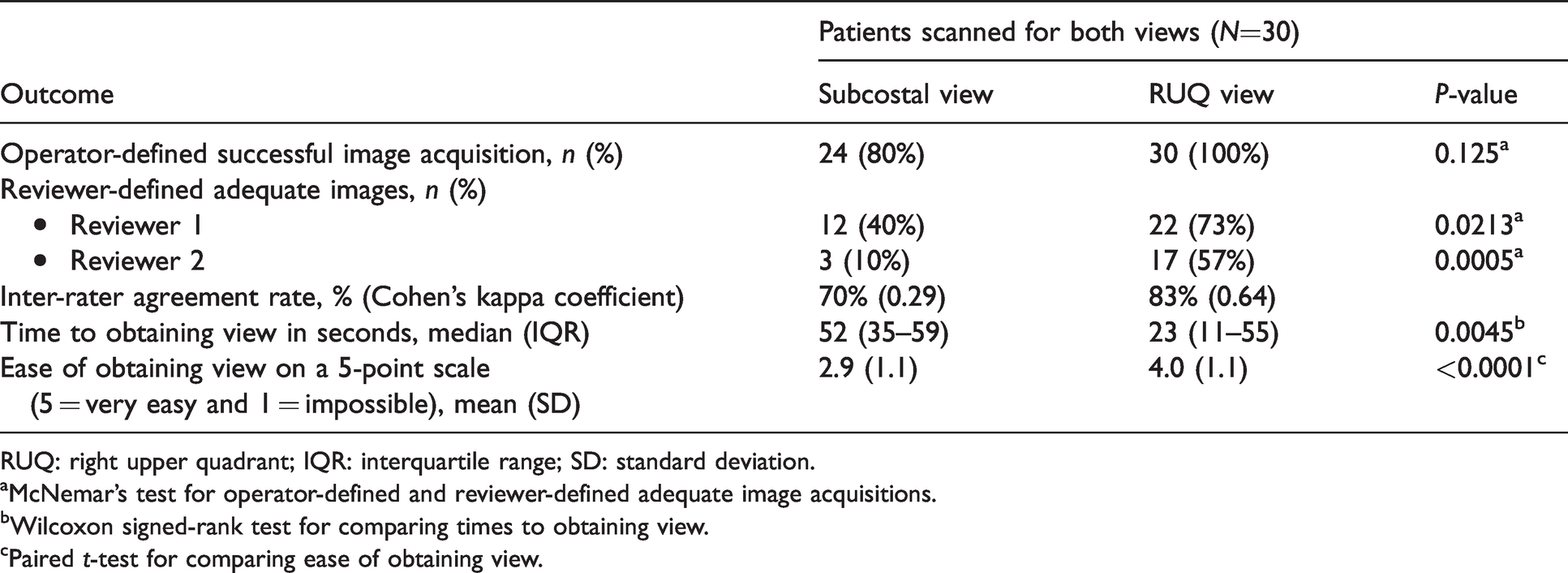
RUQ: right upper quadrant; IQR: interquartile range; SD: standard deviation.
aMcNemar’s test for operator-defined and reviewer-defined adequate image acquisitions.
bWilcoxon signed-rank test for comparing times to obtaining view.
cPaired t-test for comparing ease of obtaining view.
A post hoc exploratory analysis was performed to examine whether operator-rated ease of obtaining the view correlated with the patient’s BMI. No correlation was found between the ease of obtaining the subcostal view and BMI (Pearson correlation coefficient 0.1208, P=0.525). Furthermore, we did not find a correlation between operator-defined ease of obtaining the RUQ view with BMI (Pearson correlation coefficient 0.1223, P=0.520).
Discussion
Ultrasound evaluation of the IVC at the bedside can be helpful to a clinician when assessing a patient’s haemodynamic status and fluid responsiveness. As obtaining the traditional subcostal window of the IVC can be technically difficult in pregnant patients, the alternative RUQ view was assessed in this prospective cohort study of non-labouring pregnant women. Our results suggest that the RUQ window may provide more timely, better quality images of the IVC compared to the subcostal window.
The authors do not advocate employing IVC assessments as a sole parameter to assess fluid responsiveness; rather, IVC findings are best viewed in the clinical context. 10 Examination findings, markers of end-organ perfusion and other sonographic findings (e.g. end-systolic effacement of the left ventricle on the parasternal short-axis view, left ventricular outflow tract flow reduction, A-line predominance on lung ultrasound) should all be corroborated with IVC findings when assessing for volume responsiveness. Long and colleagues found that respiratory variation in IVC diameter as a sole parameter has limited ability to predict fluid responsiveness, particularly in spontaneously ventilating patients. 11 Based on the findings of Long et al.,11 a negative test cannot rule out hypovolaemic shock, but a positive test is highly sensitive. IVC assessment is also a vital component of the evaluation of tamponade physiology or right heart failure. 12 A plethoric non-varying IVC can be strongly suggestive of these diagnoses. Conversely, a small collapsible IVC with significant respiratory variation effectively rules out tamponade physiology or right heart failure. 13 Interrogation of the IVC will therefore remain an essential component of any POCUS examination, obstetric or otherwise.
Previous studies showed that IVC diameter measurements could be useful along with transthoracic echocardiography for the assessment of fluid responsiveness in shocked patients. 2 , 14 Finnerty and colleagues described the RUQ view (which they referred to as the transabdominal coronal long axis view) as a ‘rescue view’ in their quest to find the best view and mode to measure IVC diameter. 15 Unlike the findings reported in the literature, in which the subcostal window was generally thought to be the best viewpoint to assess the IVC,15–19 the RUQ window may be the better option in pregnant women based on our findings. Also, we noted less inter-rater agreement by the reviewers on view adequacy for the subcostal window. This further suggests the problematic nature of the subcostal view in pregnant patients.
The subcostal window has classically been thought to be more challenging in term pregnant patients due to anatomical and sonographic considerations. The contents of a gravid uterus despite being mostly sonolucent (i.e. of a low attenuation coefficient), are quite voluminous and are likely to dissipate ultrasound enough to hinder deep structure visualisation. 19 Besides, the convexity of the abdominal wall in late pregnancy creates an angle where the epigastrium meets the xiphisternum. This makes probe placement particularly challenging and alters the insonation angle, making alignment with the IVC difficult. Our findings are therefore plausible from both an anatomical and sonographic standpoint and confirm what is currently thought to be ‘conventional wisdom’ in obstetric point-of-care ultrasound.
Study strengths include imaging by an experienced ultrasonographer, as well as verification of the adequacy of obtained images by qualified ultrasound reviewers in a completely independent fashion. Each rater was blinded to the assessment of their peer. This assured an objective assessment of image quality and supported the validity of our findings. Also, to our knowledge, this is the first study to compare directly the efficiency of IVC visualisation via the subcostal and RUQ windows in this unique patient population. 9 It therefore forms an essential stepping stone in point-of-care ultrasound in the obstetric population. A previous study has also noted the feasibility of the RUQ or intercostal window in pregnant patients but did not compare the efficiency or image quality of this window with the subcostal window. 20 Finally, this study focused on assessing timely image acquisition, which in certain clinical settings may be of paramount importance. In the context of obstetric emergencies, expeditious assessments are crucial as relatively small delays in management may adversely affect both maternal and fetal outcomes. 4 , 12
This study has several limitations. All ultrasound exams were performed by a single trained and experienced operator (FQ), with a skill level similar to anaesthesiologists skilled in IVC visualisation. Her extensive POCUS experience would not be comparable to anaesthesiologists less experienced with ultrasound. Generalisation of study findings may therefore be limited to operators with a similar skill set. Inter-observer variability was also noted to be significant, especially with the subcostal window, between the sonographer obtaining the view and the quality assessors, and even between the independent quality assessors themselves. Previous echocardiography studies examining quantitative parameters for mitral regurgitation severity demonstrated similarly significant inter-observer variability among experienced echocardiographers. 21 Our study was more prone to disagreement by the blinded reviewers, given the more qualitative nature of image adequacy assessment. This wide inter-rater variability with the subcostal window suggests that obtaining images of the IVC can be more challenging and potentially less accurate in pregnant patients and may be more so for less experienced POCUS users. Furthermore, POCUS learners may find it more challenging to identify whether they have obtained an adequate image by way of the subcostal approach.
Another limitation is the possibility of operator bias, given that some of the outcomes (e.g. ease of obtaining view) were subjective. Blinding the investigator performing the scan to the views they are obtaining, however, would not be feasible. The study also examined haemodynamically stable pregnant patients, which limits the generalisability of our findings to less stable patients. We excluded some common conditions such as multiple gestations, which also affects the generalisability of our findings. Finally, our study only examined the feasibility of image acquisition via the RUQ and subcostal windows without comparing the obtained IVC diameters. Further research is needed to substantiate and expand our findings.
Conclusion
IVC visualisation using the conventional subcostal window in term pregnant patients can be difficult and time-consuming. The alternative RUQ approach may offer a less challenging window for IVC assessment in term pregnant women. These findings may bear significance in guiding the approach to point-of-care ultrasound image acquisition in emergency obstetric settings where timely assessment and management is required.
Footnotes
Author Contribution(s)
Acknowledgement
This study was a poster presentation at the 50th Annual Meeting of the Society of Obstetric Anesthesia and Perinatology, May 2018 (Miami, FL, USA).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.