
Abstract
This is a summary document that provides an Australian perspective on the Fourth Consensus Guidelines for the management of postoperative nausea and vomiting. The Australian Society of Anaesthetists has endorsed the Fourth Consensus Guidelines for the management of postoperative nausea and vomiting and has written this document with permission from the authors and the American Society for Enhanced Recovery to provide an Australia-specific summary.
Keywords
Postoperative nausea and vomiting (PONV) is a common and distressing complication following general anaesthesia and surgery. PONV results in reduced patient satisfaction and leads to increased healthcare costs through longer lengths of post-anaesthesia care unit (PACU) and hospital stays alongside resultant increased resource utilisation.
The 2020 updated consensus guidelines on PONV management provide a comprehensive review of strategies to minimise the risk of PONV through risk assessment and both pharmacological and non-pharmacological means. 1 , 2 Since the publication of the previous guidelines in 2014, novel drugs have been developed and there has been a general increase in the volume of day surgery and ambulatory anaesthesia. With these changes there has been a greater need to ensure common post-anaesthetic complications such as PONV are prevented in order to facilitate patient flow through to discharge, minimise distressing symptoms post-discharge, and prevent unplanned re-admissions to hospital.
Risk assessment
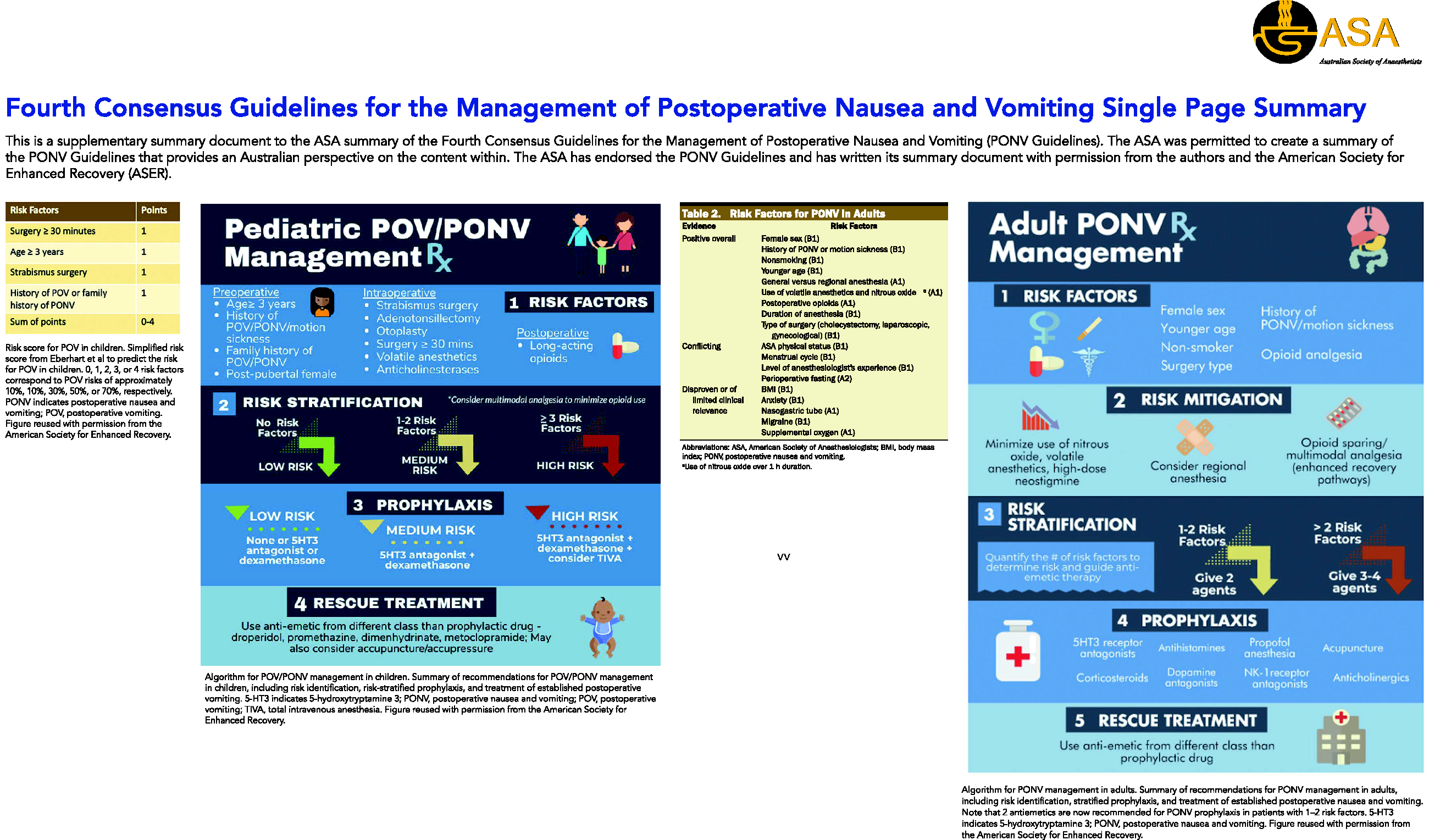
The guidelines continue to advocate for baseline patient-specific PONV risk assessment in all patients, and the incorporation of postoperative risk associated with vomiting into treatment decisions, such as in patients with raised intracranial pressure. The updated guidelines have included patient-specific risk factors, anaesthetic risk factors, and other factors that may increase the PONV risk; for example, fasting from midnight.
Patient-specific risk factors in adults (level B1 evidence):
Female gender. History of PONV and/or motion sickness. Non-smoking status. Age less than 50 years.
Patient-specific risk factors in children:
Age more than three years. History of PONV and/or motion sickness. Family history of PONV. Post-pubertal girl.
Anaesthetic and surgical factors in PONV in adults:
General (versus regional) anaesthetic. Volatile anaesthetic. Nitrous oxide for more than one hour. Duration of anaesthesia. Postoperative opioids. Type of surgery (cholecystectomy, laparoscopic gynaecological).
Anaesthetic and surgical factors in PONV in children:
Strabismus surgery. Adenotonsillectomy. Otoplasty. Surgery duration longer than 30 minutes. Volatile anaesthetic. Anticholinesterases. Long-acting opioids.
Fasting guidelines
There is good evidence to show that existing fasting guidelines, and periods of prolonged fasting, are associated with higher rates of PONV. New evidence supports relaxation of these guidelines. Administration of carbohydrate drinks up to two hours preoperatively is associated with reduced rates of PONV and no increased rates of aspiration. Liberal administration of intravenous (IV) hydration in appropriately selected paediatric patients of 30 ml/kg is associated with a reduced risk of PONV, although recent evidence suggests clear fluid intake up to one hour prior to anaesthesia may be safe, which would obviate the need for higher intraoperative fluid volumes. 3
Risk reduction techniques
While the cost-effectiveness of PONV prophylaxis remains uncertain, utilisation has been demonstrated to shorten PACU stays, reduce patient distress and prevent unplanned re-admission. Any potential cost benefit, if present, can be augmented by utilising PONV reduction strategies such as opioid minimisation, total IV anaesthesia, regional anaesthesia and optimal hydration. Regional catheter infusions are recommended when local structures and systems exist for their use.
The minimisation or avoidance of emetogenic agents such as opioids continues to be recommended to reduce PONV risk. The effect of inhaled nitrous oxide on PONV appears to be duration dependent; however, given the significant environmental impact of nitrous oxide, use should be rationalised or avoided when suitable alternatives exist.
Opioid minimisation strategies
IV paracetamol given before onset of pain reduces PONV (Level A1 evidence). IV or intramuscular non-steroidal anti-inflammatory drugs in patients with postoperative patient-controlled analgesia reduce PONV (Level A1 evidence). Systemic alpha-2 agonists reduce PONV (Level A1 evidence). Esmolol infusion can reduce PONV (cautions regarding side-effect profile and perioperative morbidity/mortality have not been included) (Level A3 evidence). Epidurals reduce PONV but intrathecal opiates may increase PONV. Bilateral transversus abdominal plane blocks reduce PONV in abdominal surgery.
Pharmacological prophylaxis
The new guidelines recommend the administration of multimodal pharmacological prophylaxis in all patients with one or more risk factors. The administration of two antiemetic agents of differing classes aims to strike the balance between maximal therapeutic potential, with minimal adverse effects, including drug interactions. There is emerging evidence for triple agent therapy, but this is not yet conclusive and the use of three agents should be weighed up against the added risks of side-effects.
The evidence for the optimal combination of anti-emetics is limited by the paucity of head-to-head studies; however, best available evidence currently recommends the first-line use of dexamethasone and a 5-hydroxytryptamine 3 (5-HT3) receptor antagonist in both adults and children. Dexamethasone continues to be recommended as a first-line agent, including in diabetes patients, in which it does not appear to result in a clinically significant effect on blood glucose levels. The recommended dose for dexamethasone has increased from 4–5 mg in the previous guidelines to 4–8 mg at induction. The doses for granisetron (0.35–3 mg IV) and ondansetron (4 mg IV, 8 mg oral dissolving tablet) remain the same in these guidelines.
There are discussions on other medications for use as prophylaxis in PONV. The discussion on the efficacy of metoclopramide centres on the fabricated studies by Fujii et al. that previously contributed to the recommendation that the 10 mg dose of metoclopramide was not effective. 4 The evidence on this is now conflicting. Cyclizine, which is used in Australia for the prophylaxis and treatment of PONV in adults, is not discussed under the antihistamines, assumingly due to it being discontinued or a lack of US Food and Drug Administration (FDA) approval in North America. 5
Midazolam has a demonstrated antiemetic effect and was included in earlier guidelines; however, its use as an antiemetic is cautioned against in these updated guidelines, given the additional and potentially undesirable sedative effect. Droperidol was previously associated with an FDA black box warning over concerns about its effects on QT interval prolongation. This has since been removed as the antiemetic dose of droperidol is not associated with an increased risk of polymorphic ventricular tachycardia and any QT prolongation is transient. The recommended antiemetic dose is 0.625 mg, although it should be avoided in patients with pre-existing QT prolongation.
All drug choices should be patient specific, taking into account pre-existing comorbidities, potential drug interactions, allergies and intolerances, such as avoiding dopaminergic antagonists in patients with Parkinson’s disease. While newer antiemetic agents such as neurokinin 1 (NK1) receptor antagonists, for example, aprepitant, have been developed and are included in these guidelines, as yet they are not widely available for therapeutic use in Australia, and prescription of these should be in accordance with current national therapeutic guidelines and drug licensing.
Non-pharmacological prophylaxis is seen as a potential additional treatment option to the baseline recommended antiemetics.
Treatment of postoperative nausea and vomiting
The recommendation remains that when there has been a failure of PONV prophylaxis, rescue treatment of PONV should consist of antiemetics from a different class of medication to what the patient has already received.
Conclusions
These consensus guidelines have provided updated, evidence-based guidance on the management of PONV in children and adults. There is a greater emphasis in these guidelines on PONV management in patients specific to their surgery type, along with acknowledgement of its importance in the Enhanced Recovery After Surgery Society (ERAS) guidelines. While these are guidelines based on the availability of medications in North America, there are important points to be utilised in the Australian setting.
Footnotes
Acknowledgement
This article has been published at the request of the Australian Society of Anaesthetists without peer review. It is accompanied by an episode of the Australian Anaesthesia podcast (available from the Society website, asa.org.au) and the one-page summary infographic included here.
Author contribution (s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.