
Abstract
We examined the influence of age in beach chair position shoulder surgery and postoperative quality of recovery by conducting a single-site, observational, cohort study comparing younger aged (18–40 years) versus older aged (at least 60 years) patients admitted for elective shoulder surgery in the beach chair position. Endpoints were dichotomous return of function to each patient’s individual preoperative baseline as assessed using the postoperative quality of recovery scale; measuring cognition, nociception, physiological, emotional, functional activities and overall perspective. We recruited 112 (41 younger and 71 older aged) patients. There was no statistical difference in cognitive recovery at day three postoperatively (primary outcome): 26/32 younger patients (81%) versus 43/60 (72%) older patients, P=0.45. Rates of recovery were age-dependent on domain and time frame (secondary outcomes), with older patients recovering faster in the nociceptive domain (P=0.02), slower in the emotional domain (P=0.02) and not different in the physiological, functional activities and overall perspective domains (all P >0.35). In conclusion, we did not show any statistically significant difference in cognitive outcomes between younger and older patients using our perioperative anaesthesia and analgesia management protocol. Irrespective of age, 70% of patients recovered by three months in all domains.
Introduction
Shoulder surgery is a common procedure. In 2006, more than 530,000 shoulder arthroscopies, with or without rotator cuff repairs, were performed in the United States alone, 1 and this number does not account for open shoulder surgeries. Shoulder surgery is performed in the lateral decubitus or in the beach chair position (BCP). The BCP for shoulder surgery was introduced in the 1980s, and has the following perceived advantages: less traction on the brachial plexus; easier identification of anatomical structures and orientation; easier manipulation of the arm during surgery; improved surgical access; and easier conversion to open surgery. 2
Surgery is also being increasingly performed on older patients, with implications for postoperative outcomes. For example, older age at time of surgery has long been recognised as a major factor in morbidity and mortality.3–5 This is due to a combination of normal ageing reducing physiological reserve of all major organs, and an increased burden of disease coexisting with ageing. 6
In particular, age is the strongest risk factor for neurocognitive complications: in non-cardiac surgery, age of 60 years or older is associated with 25% higher risk of delayed neurocognitive recovery and 10% higher risk of postoperative neurocognitive disorder compared to their age-matched controls who did not have surgery and anaesthesia.7,8 Reasons include: reduction in brain volumes and neuroplasticity; fewer protective mechanisms for perioperative inflammatory changes; increased incidence of vascular disease such as hypertension; age-related impairment of cerebrovascular autoregulatory reflexes; and reduced functional cognitive reserve.9,10 Further reductions in cerebral perfusion may occur in BCP shoulder surgery due to orthostatic changes from upright positioning and from controlled hypotension used to minimise surgical blood loss and improve arthroscopic visualisation. 11
Traditional morbidity endpoints measure organ-specific complication rates, but they do not necessarily measure endpoints pertinent to our patients. Instead, patient-centred outcomes track when and if return of function occurs to preoperative baseline, while avoiding new functional disability. To our knowledge, no previous study has investigated the effects of age on patient-centred functional outcomes after BCP shoulder surgery.
We therefore performed a study comparing the functional outcomes of younger versus older patients admitted for elective BCP shoulder surgery. We used the postoperative quality of recovery scale (PostopQRS), a patient-centred outcome measurement tool that systematically assesses functional recovery up to three months postoperatively. This tool measures five domains important for recovery: cognitive, nociceptive (pain and nausea), physiological, emotive (anxiety and depression) and functional (activities of daily living). We defined our primary outcome as the proportion of younger aged patients (18–40 years) who recovered to preoperative baseline in the cognitive domain at day three postoperatively, compared to the proportion who recovered in older aged (≥60 years) patients. Secondary outcomes were the proportion of younger versus older aged patients who recovered to baseline in the other four domains within three months of surgery.
Materials and methods
Design and study subjects
This was a prospective, single-site, observational study performed in Kareena Private Hospital, Sydney, Australia. This was a planned substudy of the larger Recovery Outcomes, and Chronic post-surgical pain after Shoulder surgery (ROCS) study, which is an observational cohort study investigating surgical, anaesthetic and patient factors that may predispose to the development of chronic pain after elective shoulder surgery in adult (≥18 years) patients. For the age-dependent recovery outcomes substudy (this paper), patients who were aged 18–40 years inclusive and 60 years or older were asked also to complete the PostopQRS questionnaire.
The aims and protocols of both components of the ROCS study were explained to eligible patients, and they were recruited after providing written informed consent. Inclusion criteria for this recovery outcomes substudy was BCP positioning for shoulder surgery. Exclusion criteria included known psychiatric illness and insufficient verbal English proficiency to complete study questionnaires. Ethics approval was granted by the Ramsay Hospitals National HREC (NSPHEC-2016-005, dated 29 July 2016) and registered with the Australian and New Zealand Clinical Trials Registry (ACTRN12616000878471).
Postoperative quality of recovery measurement
The PostopQRS is a validated patient-centred outcome questionnaire (Appendix 1) and compares favourably to similar quality of recovery scales. 12 The PostopQRS is completed using direct and telephone interviews at specified postoperative timepoints up to three months after surgery.13–15 Unlike other quality of recovery tools, recovery in any PostopQRS domain is dichotomous and is defined as return to the individual patient’s preoperative baseline function; it is thus recorded as ‘recovered’ or ‘not recovered’. As an example, a patient must perform equal to or exceed their baseline cognitive score to be postoperatively recovered in the cognitive domain.
PostopQRS has been used to measure rates of cognitive recovery as a primary outcome in cardiac 16 and major non-cardiac 17 surgery; and for overall quality of recovery after orthopaedic surgery.15,18 More specifically, the five questions in the cognitive domain test working memory and executive function. 19 These questions are: orientation, digits forward, digits backwards, word recall and word generation. Questions were adapted from the Mini-Mental State Examination, Weschler Adult Intelligence Scale, Rey Auditory Verbal Learning Test, and Controlled Word Association Test. A tolerance algorithm is used to adjust for normal variability observed in cognitive scoring.20,21 Patients with poor preoperative cognitive function or impairment are automatically excluded from analysis as ‘low baseline’; in an orthopaedic surgical patient population, this rate is estimated at between 5% and 15%. 18
A researcher collected baseline function in five PostopQRS domains using the standardised questionnaires prior to surgery and premedication. To assist with numerical and verbal scoring, a faces chart which visually depicts the emotive state is shown to patients. A copy of this faces chart is also provided at discharge to improve scoring consistency when interviews are conducted over the telephone. Sociodemographic data and comorbidities were also recorded. Recovery was assessed at 15 minutes and 40 minutes after tracheal extubation, and at one day, three days and three months after surgery. Variations include: recovery in the physiological domain is assessed from 15 minutes to one day, while recovery in the functional domain is assessed from one day onwards.
The overall patient perspectives domain includes four self-reported items on ability to work, activities of daily living, clarity of thinking and satisfaction with anaesthesia care. These answers were collected at one day, three days and three months after surgery.
Perioperative management
Anaesthesia management was guided by a pragmatic, standardised protocol. Cerebral oximetry was measured using non-invasive infrared spectroscopy (SenSmart X-100 system and Equanox 8004C dual emitter/dual detector sensors; Nonin Medical, Plymouth, MN, USA). Sensors were placed on the cerebral hemisphere ipsilateral to the operative shoulder, avoiding the sagittal venous sinus, frontal air sinus and temporalis muscles. On room air, at rest and prior to any sedative premedications, the baseline regional cerebral saturation (rSO2) was recorded.
After obtaining intravenous access and commencing haemodynamic monitoring, patients received intravenous midazolam 1–3 mg for conscious procedural sedation. An ultrasound-guided interscalene brachial plexus block was performed using a 22G or 21G Stimuplex nerve block needle (B Braun, Melsungen, Germany). A volume of 0.75% ropivacaine injected was at the anaesthetist’s discretion and was recorded. Following brachial plexus blockade, general anaesthesia was induced using propofol and tracheal intubation facilitated by rocuronium. Anaesthesia was maintained using desflurane in an oxygen/air mix, and mechanical ventilation to normocapnia as measured using end-tidal capnography.
After tracheal intubation, patients were positioned into approximately 40°–60° upright BCP. The patient’s head and neck were secured in the neutral position using a specialised headrest attachment and foam facemask. The patient’s arm ipsilateral to the operated shoulder was secured to the Spider pneumatic limb positioner (Smith & Nephew, Watford, UK). Intraoperative blood pressure was measured using an appropriately sized, non-invasive oscillometric cuff on the non-operative upper arm; or invasively measured via a radial arterial cannula with the transducer placed at the level of the tragus of the ear. Using either method, controlled hypotension to a preferred target systolic blood pressure range between 90 and 100 mmHg was used; however, a higher blood pressure was permitted to ensure intraoperative rSO2 was kept to ±10% of preoperative baseline. Vasopressor (metaraminol or ephedrine) and antihypertensive agent (metoprolol) boluses were administered to titrate blood pressure and recorded.
All patients received intravenous 4 mg dexamethasone, 1 g paracetamol and 40 mg parecoxib unless contraindicated. Intravenous rescue fentanyl boluses were allowed as deemed clinically necessary for analgesia, and doses were recorded. Sugammadex was administered at conclusion of surgery to reverse muscle relaxation prior to tracheal extubation. Regular oral paracetamol, non-steroidal anti-inflammatory drugs, sustained-release oxycodone and breakthrough oxycodone were provided for all patients unless contraindicated.
Statistical analysis and sample size calculation
The primary outcome of cognitive domain recovery between younger aged and older aged patients at three days after BCP shoulder surgery was analysed using Fisher’s exact test. The secondary outcome of other postoperative quality of recovery domains at all timepoints between groups was analysed using the Cochrane–Mantel–Haenszel test with continuity correction for repeated tests of independence of proportions.
Intraoperative rSO2 electronic records were analysed offline using the Sensmart data management software supplied with the cerebral oximeter. The reference level was manually set at –10% from each individual patient’s baseline rSO2. Potential cerebral ischaemia is calculated as area under the curve of total time that intraoperative rSO2 fell below this reference level; this is recorded as cumulative desaturation in minutes-%. Demographic and perioperative differences between age groups were analysed with t-tests, Mann–Whitney, or chi-square tests for parametric, non-parametric and categorical data, respectively.
PostopQRS cognitive domain recovery data are available from a randomised controlled trial comparing younger patients (18–40 years) and older patients (≥65 years) undergoing orthopaedic knee surgery. 15 On postoperative day three, 83% of younger patients had recovered compared to 50% in older patients. In order to detect a difference in cognitive recovery between age groups, with two-sided significance less than 0.05 and power of 0.80, a sample size of 29 patients is required, calculated using Wang and Chow’s formula for comparing proportions. 22 To compensate for withdrawals and for the possibility of 15% of patients being excluded due to low baseline preoperative cognitive function, the sample size was increased to 40 patients. Analysis was performed using SPSS version 25 (IBM Corp, Armonk, NY, USA). Statistical significance was determined by two-tailed analysis, P <0.05.
Results
A total of 178 adult patients were recruited for the larger chronic post-surgical pain study between February 2017 and October 2019. A total of 112 patients satisfied the age inclusion criteria for this substudy, composed of 41 younger aged patients (18–40 years inclusive), and 71 older aged patients (≥60 years). Twenty patients were excluded from analysis of the primary outcome of cognitive recovery at postoperative day three; seven patients (6%) were due to low baseline preoperative cognitive scores (Figure 1).
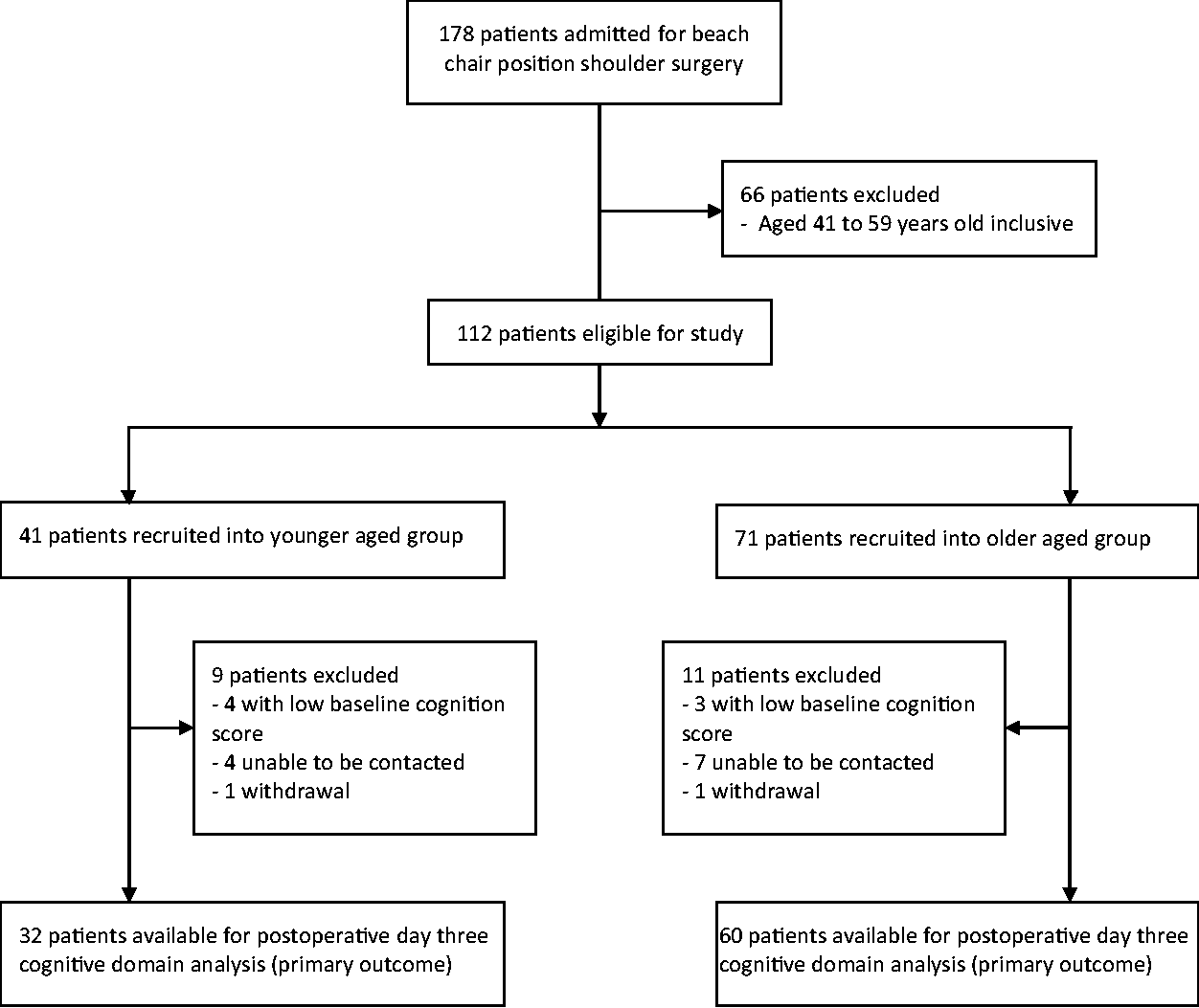
Study flow diagram.
Sociodemographic characteristics and intraoperative data comparing the younger aged and the older aged groups are shown in Tables 1 and 2, respectively. More younger aged men underwent surgery than women, although this proportion is less distinct in older aged patients. Not unexpectedly, older aged patients had significantly worse American Society of Anesthesiologists physical status classification levels, and 30 (42%) patients were diagnosed with hypertensive disease requiring medication (P <0.001). Proportionately higher numbers of older aged patients underwent total shoulder arthroplasty (37%), and less reconstructive surgery such as labral repair or Latarjet procedures (25%), than younger patients (10% and 49%, respectively, P <0.001). More extensive surgery for older patients is reflected in statistically significant differences in surgery duration and ropivacaine doses for interscalene blocks, median (interquartile range (IQR)) 150 mg (98–150 mg) versus 90 mg (90–150 mg), P=0.01. Vasoactive medications were required in only three (7%) younger patients, compared to 32 (45%) older patients (P <0.001). Baseline, preoperative, at rest, room air, rSO2 was statistically lower in older versus younger patients, 72% (69%–74%) versus 76% (72%–80%), P=0.02. However, intraoperative rSO2 was maintained comparably between groups, and the cumulative desaturation below reference was zero minutes-% in both groups (P=0.79).
Sociodemographic characteristics of recruited patients.
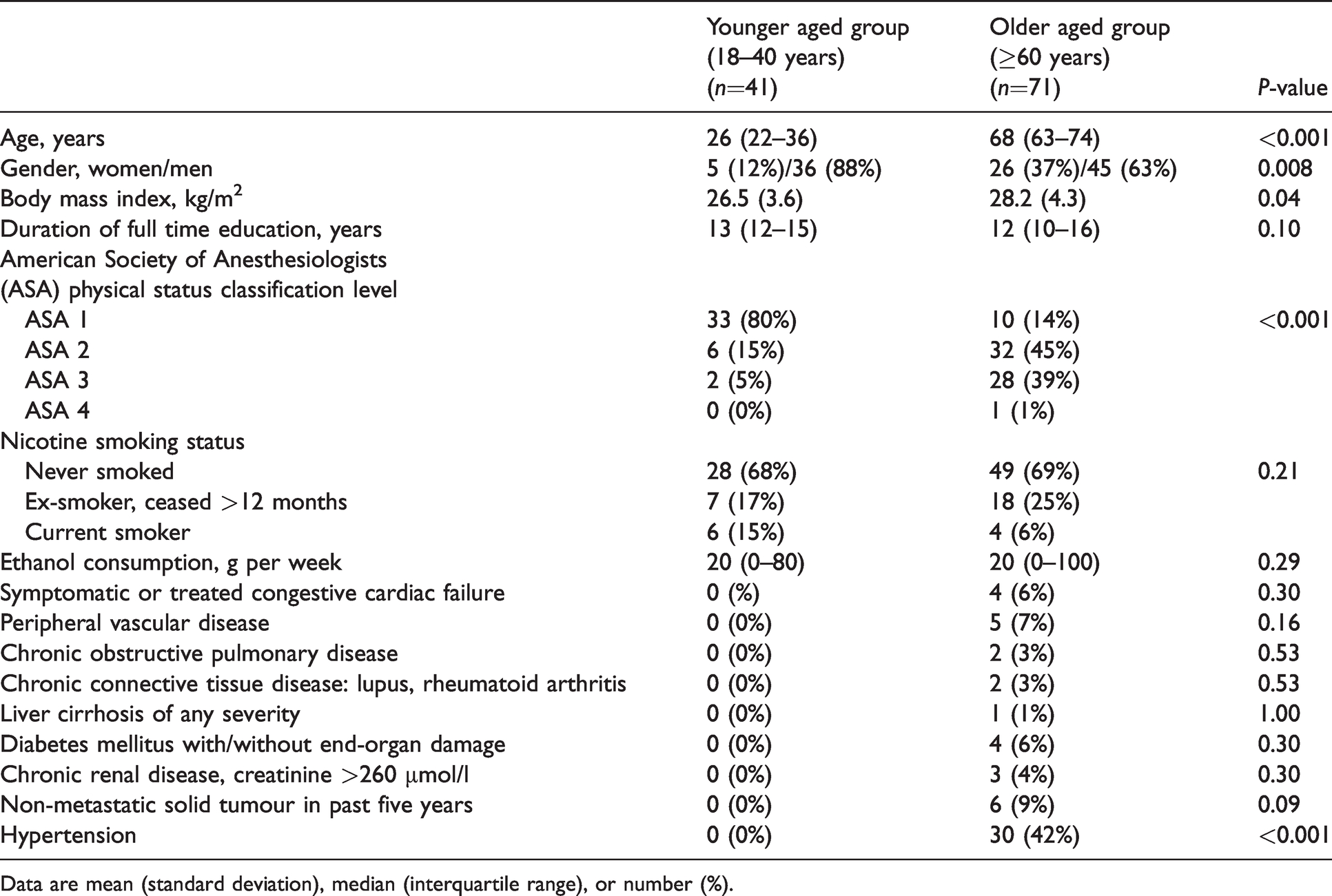
Data are mean (standard deviation), median (interquartile range), or number (%).
Intraoperative characteristics of recruited patients.
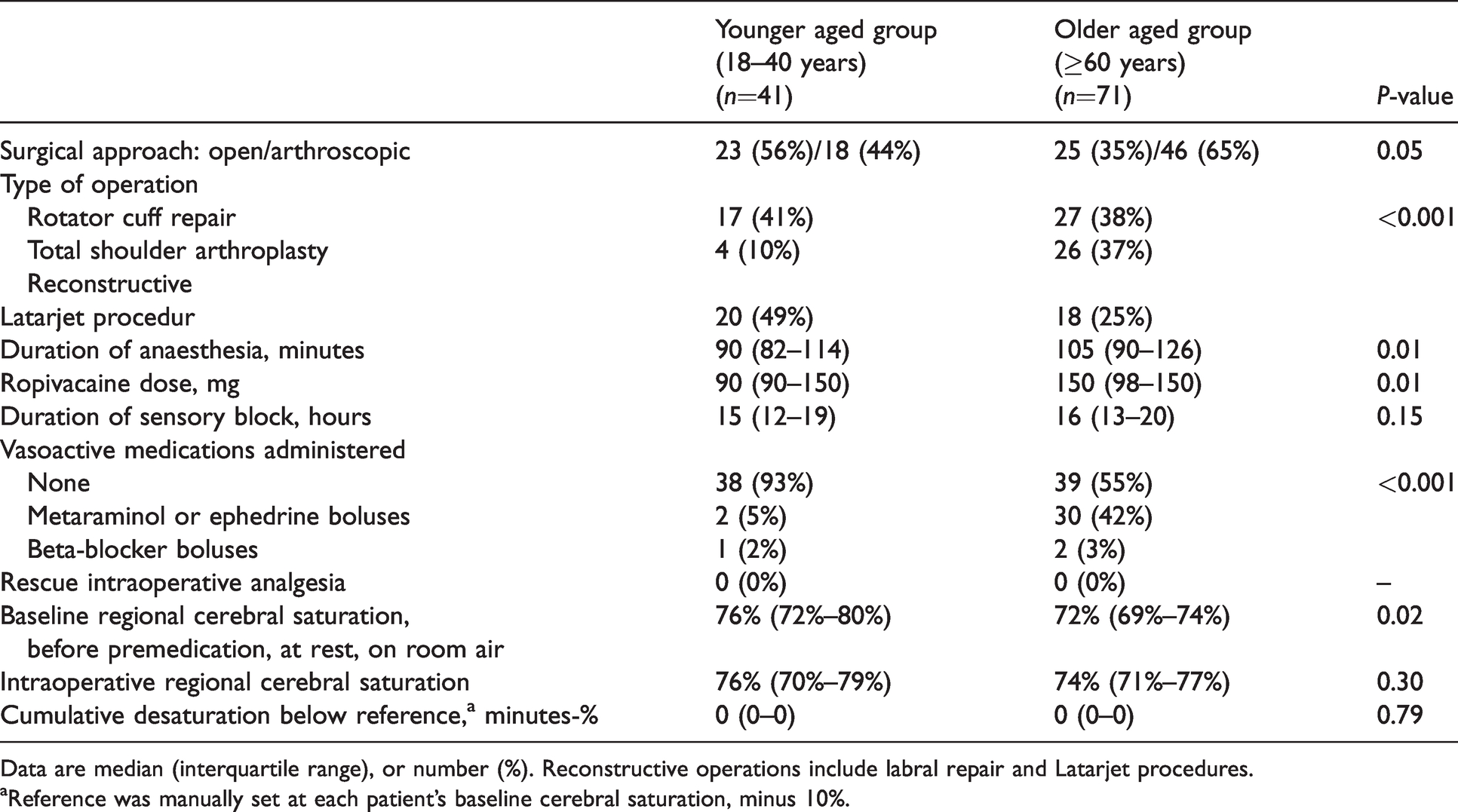
Data are median (interquartile range), or number (%). Reconstructive operations include labral repair and Latarjet procedures.
aReference was manually set at each patient’s baseline cerebral saturation, minus 10%.
For the primary outcome, there was no statistically significant difference between the cognitive domain recovery on postoperative day three in younger patients, 26 recovered out of 32 (81%), versus older patients, 43 recovered out of 60 (72%), P=0.45 (Figure 2). In the secondary outcome of cognitive recovery up to postoperative day one, there was a statistically significant difference with younger patients recovering proportionally more than older patients–34%, 76% and 91% recovered versus 18%, 40% and 73% at 15 minutes, 40 minutes and one day, respectively, P <0.001. Other secondary outcomes of quality of recovery in the nociception, physiological, emotional and functional activities domains at all timepoints are illustrated in Figure 3. The recovery trajectory of physiological and functional activities of daily living was similar in younger and older patients alike (both domains P >0.40). In the immediate postoperative phase (up to three days), older patients experienced better recovery in pain and nausea than younger patients, but were conversely more anxious and depressed (both domains P=0.02); however, by the later postoperative phase (three months) this difference was not observed. There was no statistically significant difference between groups in the self-reported overall patient perspectives domain, P >0.35 (Figure 4).
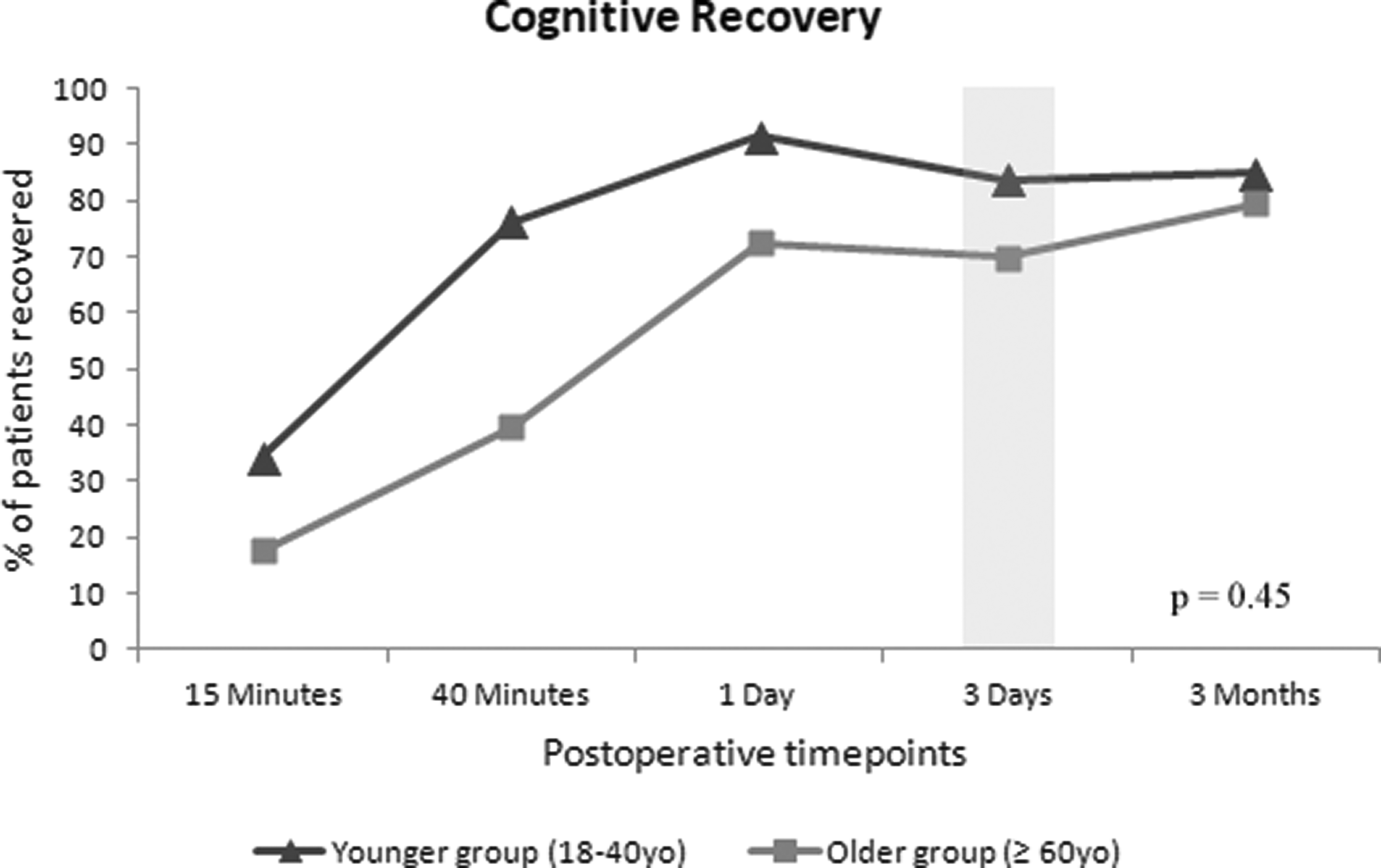
Proportion of younger aged patients (triangles) compared to older aged patients (squares) who recovered in the cognitive domain of the postoperative quality of recovery at scheduled postoperative timepoints. Shaded bar denotes time frame for comparison between groups.
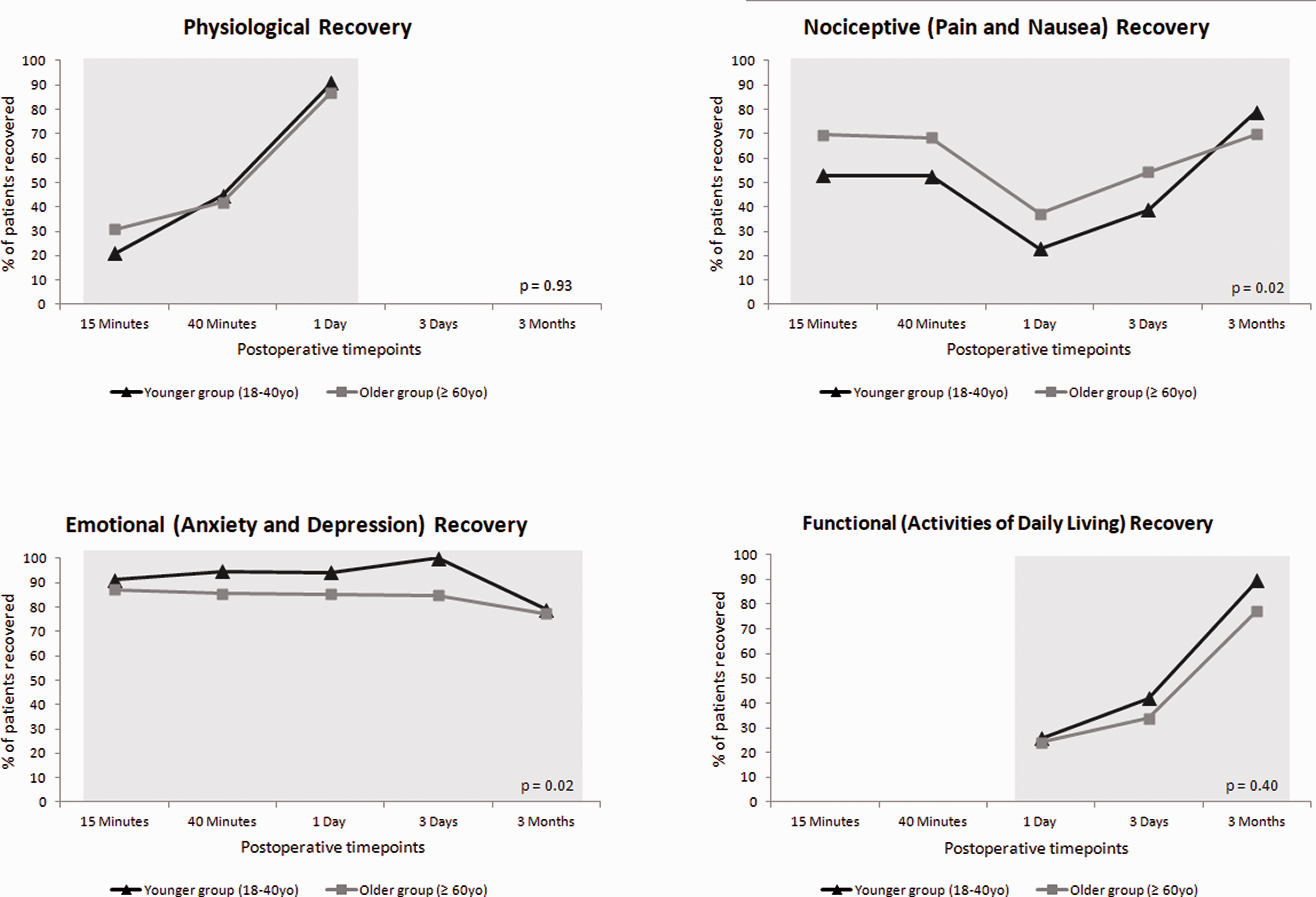
Proportion of younger aged patients (triangles) compared to older aged patients (squares) who recovered in the physiological, nociceptive, emotional and functional domains of the postoperative quality of recovery at scheduled postoperative timepoints. Shaded bar denotes time frame for comparison between groups.
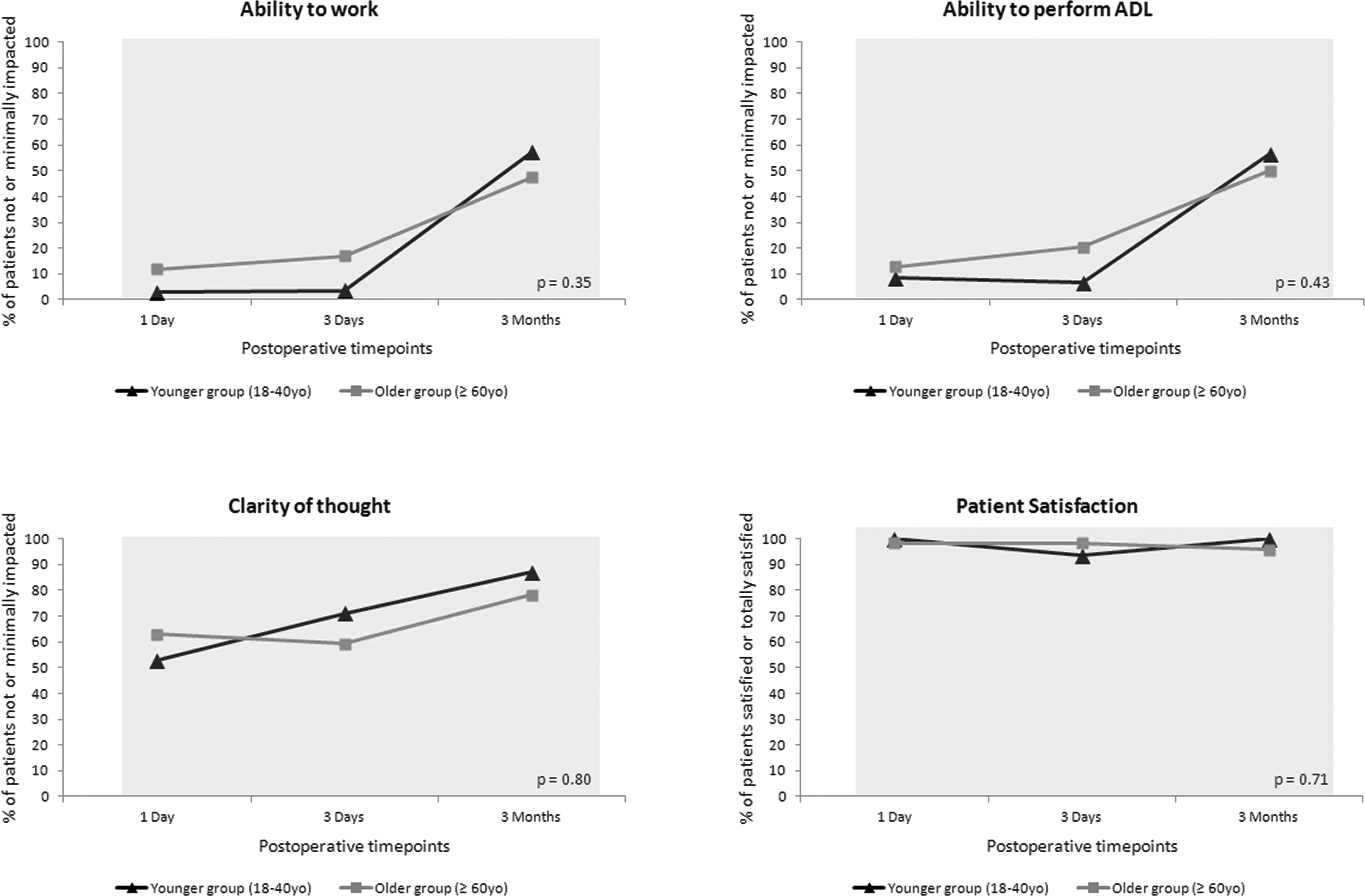
Proportion of younger aged patients (triangles) compared to older aged patients (squares) who recovered in the overall patient perspectives domain of the postoperative quality of recovery at scheduled postoperative timepoints. Shaded bar denotes time frame for comparison between groups.
Discussion
This study of postoperative quality of recovery after BCP shoulder surgery found that younger patients recovered more quickly to their preoperative cognitive baseline function than older patients up to a day after surgery, but this disparity was not statistically significant by day three. For the secondary outcomes in the nociceptive and emotional domains, statistically significant age-related differences occurred in the immediate to intermediate postoperative period but this disappeared by the late postoperative period. In the physiological and functional domains, there was no statistically significant difference in recovery between the age groups. Similarly, no significant differences were found in the self-reported patient perspectives of ability to work, ability to perform activities of daily living, clarity of thinking, or satisfaction with anaesthesia care. At least 70% of patients, irrespective of age, recovered to their preoperative baseline in all domains within three months of surgery. This study thus revealed there are age-related differences in postoperative quality of recovery that are domain specific and dependent on time frame.
Two previous studies examined the quality of recovery after shoulder surgery. Boissard et al. 23 investigated whether inpatient or outpatient shoulder surgery influenced recovery, and found no difference up to seven days postoperatively. Elkassabany et al. 24 compared patients before and after commencement of a standardised multimodal analgesia protocol; patients on the new protocol had improved quality of recovery up to seven days postoperatively. Both studies used the quality of recovery QoR-15 and QoR-9 scales, which are composite scores without discrete domains. The strengths of our study include: we investigated the influence of age on recovery; it was specific for BCP shoulder surgery; it used a recovery scale that collects granular information on trajectory of recovery in multiple domains; it was powered for a cognitive outcome and performed late follow-up to three months.
The effect of anaesthesia in older patients is an active area of research. Most shoulder surgery studies have focused on the devastating but rare complication of cerebrovascular stroke and death after BCP shoulder surgery. However, after adjusting for age, these studies have not shown differences in neurocognitive outcomes, serum brain injury biomarkers, or regional cerebral oxygenation using either near-infrared spectroscopy or cerebrovascular autoregulation indices.25,26 In our study, a delay in dichotomous return of cognitive function was found to occur in older patients, but the contribution of surgical, anaesthetic, or patient factors remains unclear.
One surgical contribution could be that older aged patients have more invasive and longer duration surgery. It is unlikely that cerebral ischaemia was a contributor in our study. Our protocol stipulated a more stringent threshold of 10% decrease from rSO2 preoperative baseline rather than a more lenient 20%. 27 We recorded zero minutes-% of cumulative desaturation, although 45% of older patients did require vasoactive drug administration to maintain this target band.
Pain was also unlikely to be a contributor, as older patients recovered faster in the nociceptive domain. This finding is not unexpected as age-related changes result in increased pain perception thresholds and lower pain scores, compared to younger patients.28,29 Our perioperative analgesia management is identical to best-practice procedure-specific postoperative pain management (PROSPECT) recommendations for rotator cuff surgery, 30 but nonetheless there was a worsening of pain in both age groups during the first postoperative day as the interscalene brachial plexus block presumably wore off.
An interesting finding is the lower proportion of older patients with emotional domain recovery. Our results are similar to those reported by Weekes et al., 31 who found increased rates of postoperative depression after shoulder stabilisation surgery, with older age as a risk factor. It is known that the incidence of depression is higher in shoulder surgery patients than in the general population; the presence of depression and other psychological problems increases the risk of morbidity and negatively impacts on rates of surgical success after shoulder operations. 32
There are several limitations to our study. Assessment of cognition in perioperative patients is difficult and complicated by residual effects of anaesthesia, opioid analgesics, pain and emotional state. We chose postoperative day three as our cognition primary endpoint to reduce the confounding effects of anaesthesia and surgery in the immediate postoperative period. The PostopQRS cognitive outcome is dichotomous, using each patient’s baseline function as the comparator; it is, however, insensitive to subtle changes in neurocognition. Our study was also powered using an absolute 33% difference in cognitive outcome; to detect more subtle but still potentially clinically important change in cognitive recovery would require a larger sample size. Our study is also a pragmatic design, standardising anaesthesia care, but we did not investigate causal associations between patient characteristics and cognitive outcome. We did not employ depth of anaesthesia monitoring; deeper versus lighter anaesthesia has not been shown to affect delayed neurocognitive recovery 26 or major end-organ outcomes, 33 but this controversy is unresolved and control of blood pressure may be of greater importance. 9 Finally, we performed multiple statistical comparisons between groups (Tables 1 and 2), which increases the possibility of a type I error. Our results are thus hypothesis-generating; future studies should consider complementing our patient-reported outcome results with dedicated neurocognitive screening tools and control factors influencing anaesthesia depth. We powered our study to detect a large difference between younger versus older patients, and a larger trial would be required to detect smaller differences in dichotomous cognitive recovery. Finally, we used chronological age to differentiate our groups; however, frailty may be a better concept as this categorises patients by a multisystem approach that is a stronger predictor of postoperative outcomes than chronological age alone. 34
In conclusion, we found that older patients did not recover as quickly as younger aged patients in the cognitive domain immediately postoperatively, but this difference was not significant by day three. Older patients also had significantly lower recovery in the emotional domain, but conversely had better nociceptive recovery. Older patients did require more frequent interventions to maintain haemodynamic parameters and cerebral oxygenation. When managed with our perioperative anaesthesia and analgesia protocol for elective BCP shoulder surgery, 70% of patients both younger and older aged recovered in all PostopQRS domains by three months after surgery.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X211020319 - Supplemental material for Age-related differences in cognition and postoperative quality of recovery after beach chair position shoulder surgery
Supplemental material, sj-pdf-1-aic-10.1177_0310057X211020319 for Age-related differences in cognition and postoperative quality of recovery after beach chair position shoulder surgery by Alwin Chuan in Anaesthesia and Intensive Care
Footnotes
Data sharing statement
The dataset for this study is available from the corresponding author on reasonable request.
Author contributions
Declaration of conflicting interests
The authors declare no potential conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.