
Abstract
Alcohol misuse is a disproportionately large contributor to morbidity and mortality in the Northern Territory. A number of alcohol harm minimisation policies have been implemented in recent years. The effect of these on intensive care unit (ICU) admissions has not been fully explored. A retrospective before–after cross-sectional study was conducted at the Alice Springs Hospital ICU between 1 October 2017 and 30 September 2019. The primary outcome was the proportion of admissions in which alcohol misuse was a contributing factor in the 12 months before (pre-reforms phase) versus the 12 months following (post-reforms phase) implementation of alcohol legislation reforms. Secondary outcomes were measures of critical care resource use (length of stay, need for and duration of mechanical ventilation). After exclusions, 1323 ICU admissions were analysed. There was a reduction in the proportion of admissions associated with alcohol misuse between the pre-reforms and post-reforms phases (18.8% versus 11.7%, P < 0.01). This was true for both acute (10.6% versus 3.6%, P < 0.01) and chronic misuse (13.3% versus 9.6%, P = 0.03). Rates of mechanical ventilation were unchanged during the post-reforms phase (18.3% versus 14.7%). Admissions with a primary diagnosis of trauma were lower (10.5% versus 4.7%, P < 0.01). This study demonstrated a reduction in ICU admissions associated with alcohol misuse following the implementation of new alcohol harm minimisation policies. This apparent reduction in alcohol-related harm is suggestive of the effectiveness of the Northern Territory’s integrated alcohol harm reduction framework.
Introduction
Alcohol misuse is a disproportionately large contributor to morbidity and mortality in the Northern Territory (NT) compared with other jurisdictions.1,2 This is reflected in the high proportion of intensive care unit (ICU) admissions associated with alcohol misuse. 3 There have been a number of changes in government policy over the last three decades in attempts to reduce these harms.4,5
In 2018 a raft of alcohol legislation reforms came into effect in the NT as part of the government’s Alcohol Harm Minimisation Action Plan. 6 These reforms were based on recommendations from the Riley Review, which was set up to make recommendations to guide the development of an integrated alcohol harm reduction framework, reporting in October 2017. 4 The subsequent policy changes included the introduction of a floor price or minimum unit price (MUP) for alcohol at A$1.30 per standard drink in October 20187 and the introduction of Police Auxiliary Liquor Inspectors (PALIs) in August 20188. The PALIs, stationed at takeaway liquor outlets, were tasked to screen for consumers taking alcohol to restricted areas, and to enforce alcohol harm minimisation legislation already in place such as restrictions on the volume of certain types of alcohol sold and use of the Banned Drinkers Register (BDR). 9 PALIs evolved from a previous policy (temporary beat locations (TBLs)) in which uniformed police officers performed a similar role. TBLs were criticised for being resource intensive and inconsistent, while leaving other policing areas under-resourced. 5 The BDR, initially trialled from 2011 to 2012, was revised and reintroduced in the NT in September 2017.9,10 It is an alcohol supply reduction measure that involves placing people who consume alcohol at harmful levels onto a register that prohibits the purchase, consumption or possession of alcohol for three to 12 months. These legislative changes have since been incorporated in the Liquor Act 2019, which replaced the Liquor Act 1978.
A previous observational study by Secombe 11 examining the impact of alcohol misuse on ICU admissions and resource burden at Alice Springs Hospital (ASH) from April 2018 to March 2019 found a 54% reduction in admissions associated with acute alcohol misuse in the six months following the implementation of the new laws.
To understand the longer-term impact of these alcohol reforms and to account for seasonal fluctuations, we conducted a retrospective before–after cross-sectional study comparing ICU admissions associated with alcohol misuse 12 months before and after implementation of the MUP of alcohol. Although a number of policies have been introduced, the MUP represents the final piece of policy and a pragmatic breakpoint at which to evaluate the effect of these reforms. It was hypothesised that there would be lower rates of ICU admission associated with alcohol misuse in the 12 months following implementation of the new alcohol policies.
Methods
The study was undertaken at ASH ICU, a ten-bed unit in Central Australia with approximately 600 admissions per year. It is the only critical care facility for 1500 km in any direction, serving a population of approximately 50,000 dispersed over one million square kilometres. 12 Approximately two-thirds of the patients identify as Indigenous.3
Data relating to all admissions to the ASH ICU are routinely entered into the Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcome and Resource Evaluation’s Outcome Measurement and Evaluation Tool (COMET). These local data are subsequently uploaded to the ANZICS Adult Patient Database (APD)—one of four clinical quality registries maintained by ANZICS. COMET was used to identify all patients admitted to the ICU between 1 October 2017 and 30 September 2019 (52 fortnights).
Admissions with no outcome data were excluded as were re-admissions to ICU that occurred during the same hospital episode. Multiple ICU admissions were included if they occurred during a separate hospital episode.
Data regarding patient demographics (age, gender, Indigenous status), the presence of comorbidities (diabetes, chronic liver, respiratory, cardiovascular and renal disease), disease severity, reason for admission, measures of resource use including level of care required (high dependency unit versus ICU), ICU and hospital length of stay (LOS), need for mechanical ventilation, duration of mechanical ventilation, and survival (ICU and hospital mortality) were extracted. 13
Illness severity was described using the Acute Physiology and Chronic Health Evaluation (APACHE) III scoring system and the Australian and New Zealand Intensive Care Risk of Death (ANZROD) model.14–16 ANZROD is derived from locally collected variables and components of the APACHE scoring system. It provides accurate mortality prediction for admissions to Australian and New Zealand ICUs. 16 The reason for ICU admission was taken from the ANZICS modification of the APACHE III diagnostic coding system. 13 Individual admission diagnoses were grouped into seven major system-based categories.
Definitions of alcohol misuse.
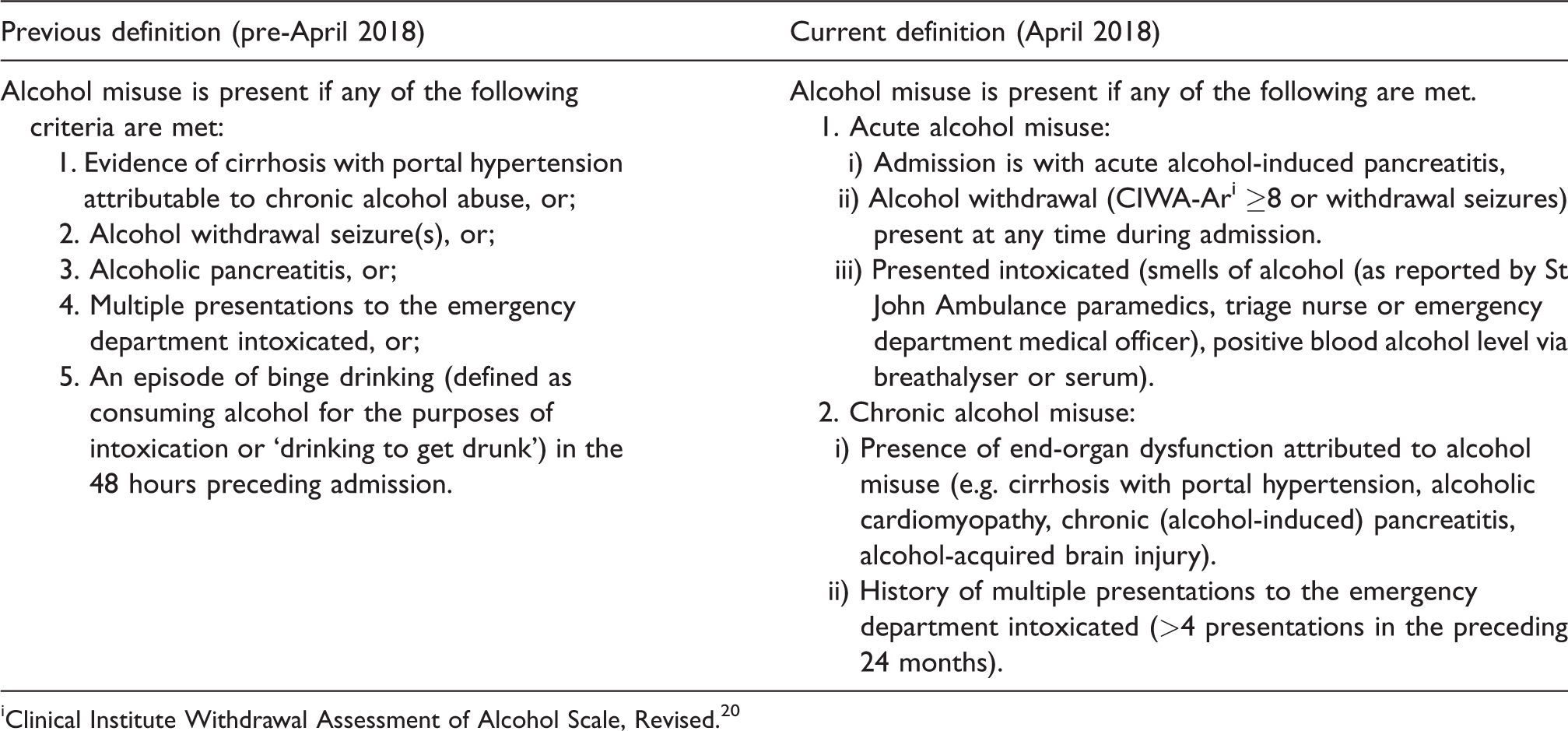
iClinical Institute Withdrawal Assessment of Alcohol Scale, Revised. 20
The primary outcome was the proportion of ICU admissions associated with alcohol misuse in the 12 months before the implementation of the MUP on 1 October 2018 (pre-reforms phase) compared with the 12 months following (post-reforms phase). Secondary outcomes included the proportion of admissions associated with acute or chronic alcohol misuse, measures of resource use (ICU and hospital LOS), need for mechanical ventilation, and mortality (both ICU and hospital) during these two periods. All endpoints were defined a priori.
Ethics approval was granted by the Central Australian Human Research Ethics Committee (CA-18-3110) and the study was conducted following the Strengthening the Reporting of Observational Studies in Epidemiology standards (see supplementary data). 17
Statistical analysis
Data were analysed with STATA™ version 15.1 (Statacorp, College Station, TX, USA). All data were initially assessed for normality. Group comparisons were performed using chi-square tests, the Student’s t-test for normally distributed data and the Kruskall–Wallis test for non-normally distributed data. Results are reported as n (%), mean (standard deviation) or median (interquartile range) respectively. A two-sided P-value of 0.05 was used to indicate statistical significance, and no adjustment was made for multiple comparisons. Sensitivity analyses using multivariable regression were undertaken to account for baseline imbalances where there was a difference (<0.2) between the pre- and post-reforms periods.
To assess temporal trends across the sampling period, segmented linear regression analysis with data aggregated at a fortnightly level was undertaken. Segmented regression is a well-established statistical technique that is used when multiple timepoints exist before and after an intervention and is used in order to determine whether or not an intervention had a significantly greater effect than any underlying secular trend. The breakpoint for analysis was arbitrarily defined by the introduction of the MUP, the last of the policy framework implementations, that is to say 1 October 2018 (Fortnight 27). Segmented regression was used to evaluate whether there had been a stepwise change (change in the intercept) in the proportion of admissions admitted to ICU with alcohol misuse and whether there was difference in the rate of change (change in slope) after the breakpoint. 18 A further sensitivity analysis using the segmented regression technique substituting absolute numbers for proportion was also undertaken. The methodology suggested by the University of California, LA, USA, was followed. 19
Results
Between October 2017 and September 2019 there were 1353 patients admitted to the ASH ICU. After exclusions, the study dataset comprised 1323 episodes of care available for analysis: 622 during the pre-reforms phase and 701 during the post-reforms phase (Figure 1). Patients admitted during the post-reforms phase were slightly older (48 versus 51 years, P < 0.01), and less likely to have chronic cardiovascular disease (7.4% versus 4.4%, P = 0.02), but were otherwise similar in baseline characteristics (Table 1).
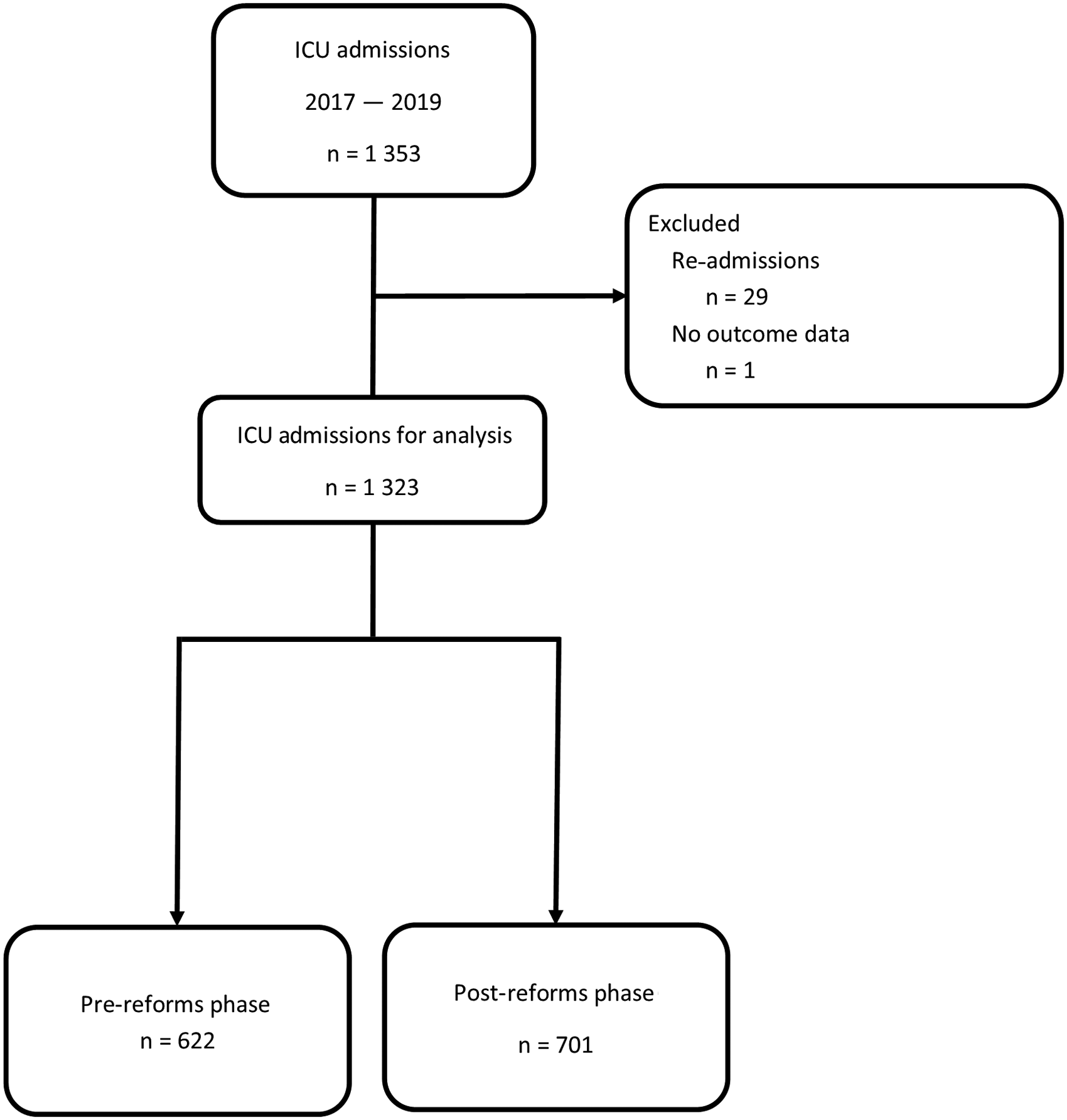
The study dataset after exclusions.
Characteristics of patients admitted to Alice Springs Hospital intensive care unit.
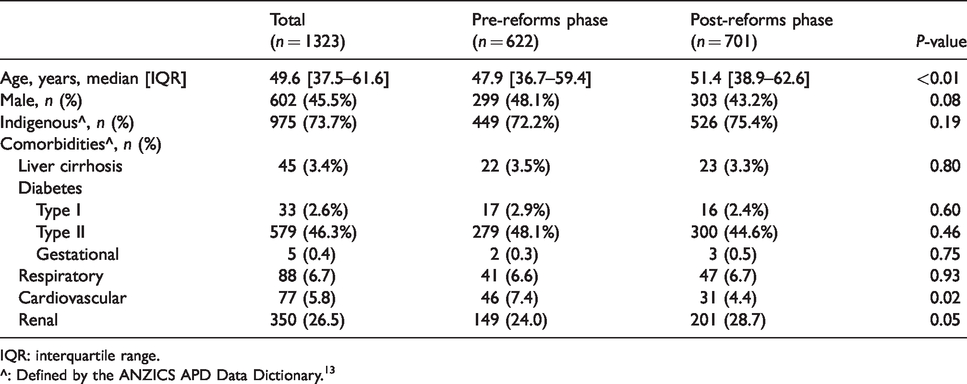
IQR: interquartile range.
^: Defined by the ANZICS APD Data Dictionary.13
Sensitivity analysis (Supplementary Table 1) using multivariable regression to account for baseline differences between the pre- and post-reforms phases confirmed that the breakpoint chosen (introduction of the MUP) remained significant.
There was a 38% relative reduction in ICU admissions associated with alcohol misuse in the post-reforms phase (18.8% versus 11.7%, P < 0.01; Table 2). The bulk of this was due to a reduction in admissions associated with acute alcohol misuse (10.6% versus 3.6%, P < 0.01), although there was also a smaller reduction in admissions associated with chronic alcohol misuse (13.3% versus 9.6%, P = 0.03) and admissions associated with both acute and chronic misuse (5.1% versus 1.4%, P < 0.01; Figure 2).
Outcomes.
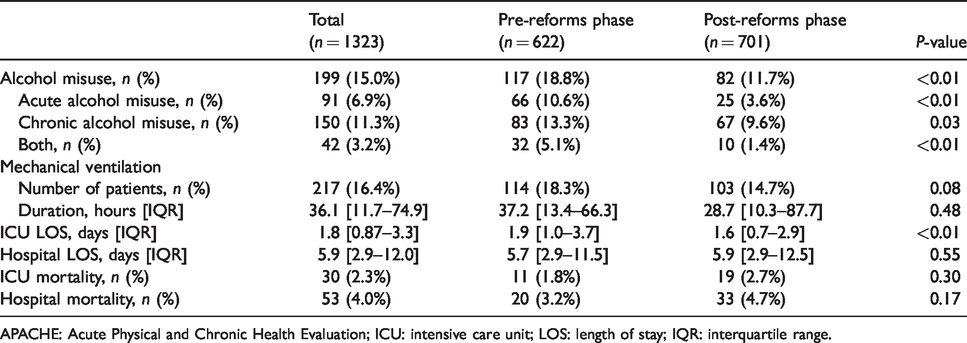
APACHE: Acute Physical and Chronic Health Evaluation; ICU: intensive care unit; LOS: length of stay; IQR: interquartile range.
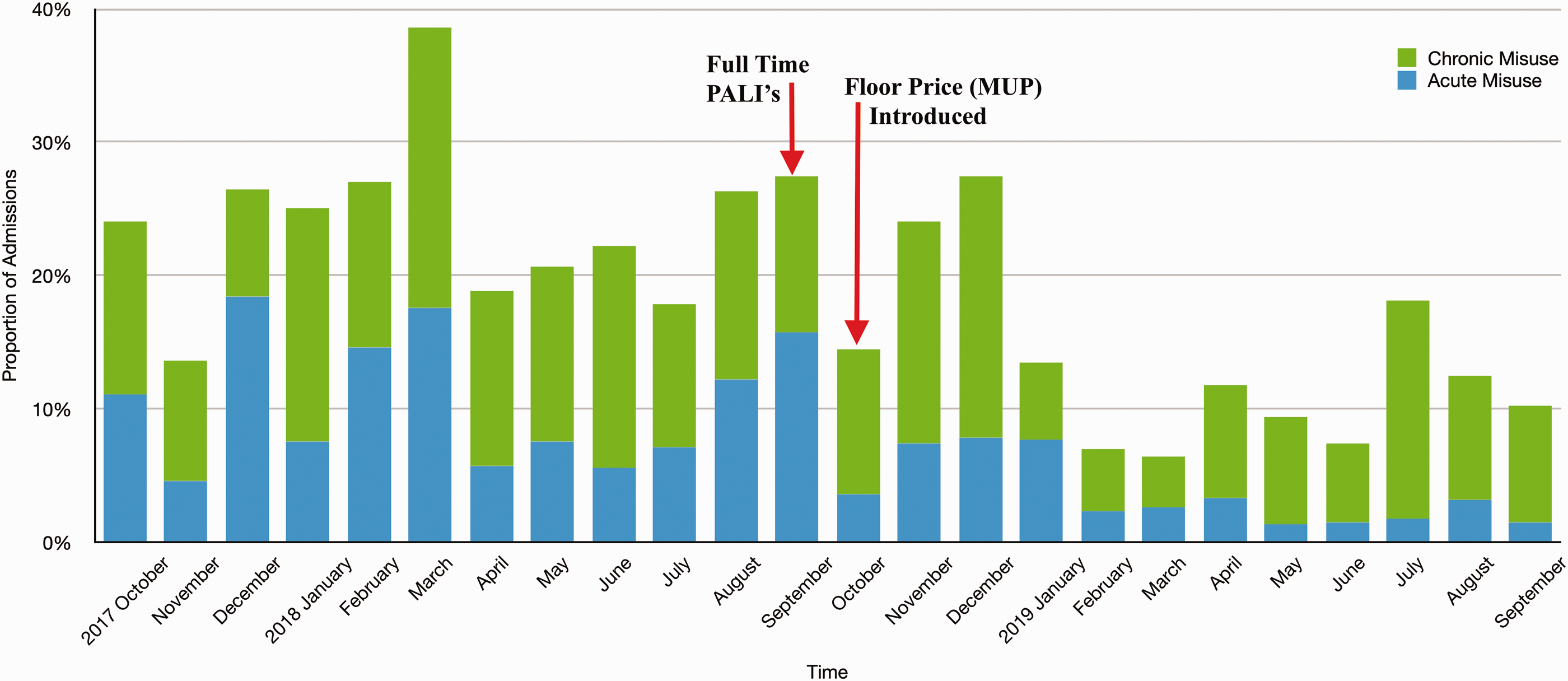
Proportion of Alice Springs Hospital intensive care unit admissions associated with alcohol misuse.
Segmented regression analysis confirmed that the slope of the fitted lines for each of the three endpoints (misuse, acute misuse and chronic misuse) changed in the post-reforms phase (Figure 3(a) to (c)), although these changes did not reach statistical significance. The full model for each, including the coding, can be found in the supplementary data file (Supplementary Tables 2–4). Sensitivity analysis applying segmented regression (Supplementary Figures 3(a) to (c)) using absolute numbers rather than proportion of admissions did not alter the overall results substantially.
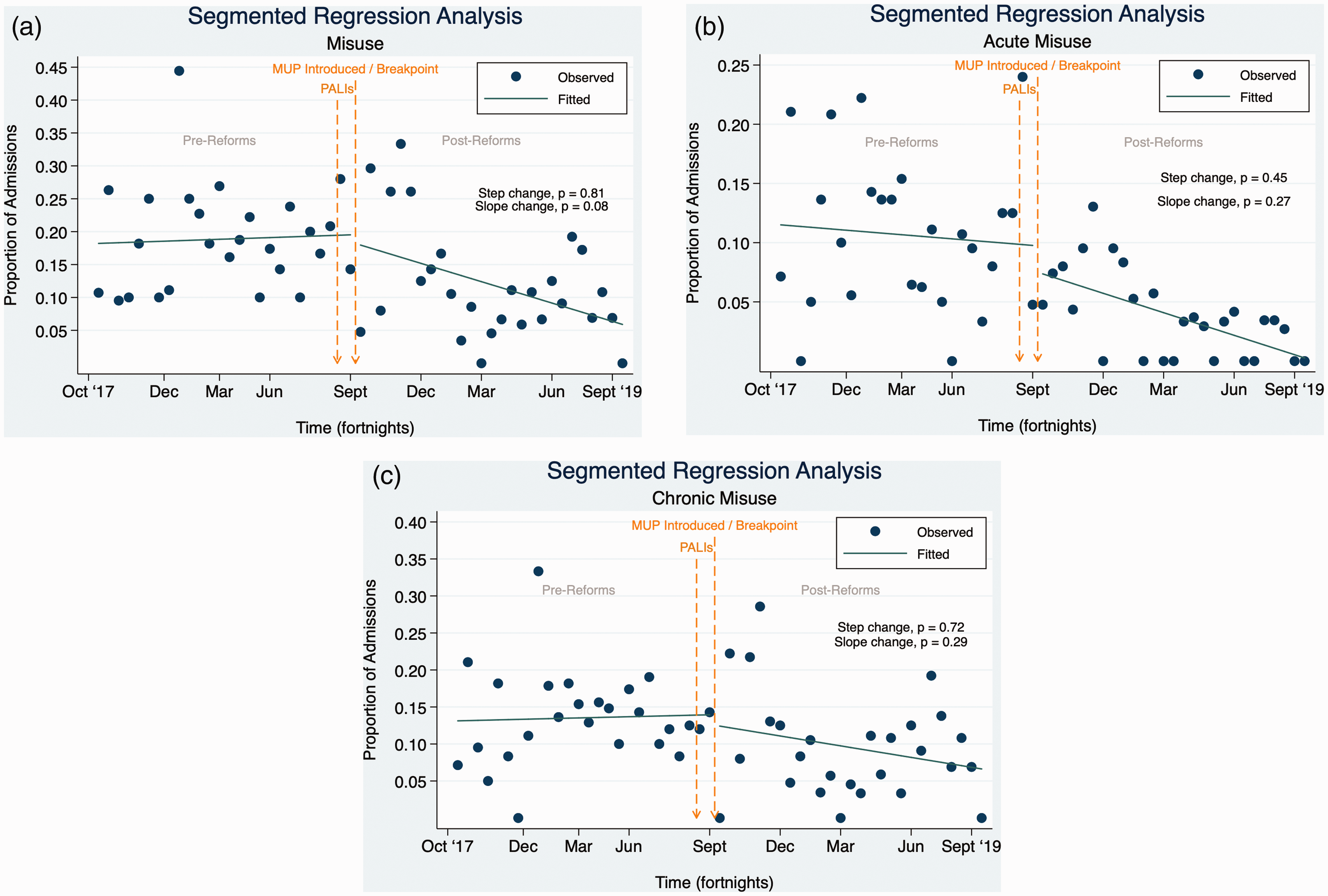
Segmented regression analysis of Alice Springs Hospital intensive care unit admissions associated with (a) overall misuse, (b) acute misuse, and (c) chronic misuse.
There was no difference in the proportion of patients requiring mechanical ventilation between the two periods (18.3% versus 14.7%, P = 0.08, for the pre- and post-reforms phases respectively), although the duration of mechanical ventilation was shorter in the post-reforms phase. ICU LOS was shorter in the post-reforms phase (1.9 versus 1.6 days, P < 0.01). There were no other significant differences for the remaining secondary outcomes (Table 2).
During the post-reforms phase there were fewer patients admitted with a primary diagnosis of trauma (10.5% versus 4.7%, P < 0.01) and slightly more patients admitted with a cardiovascular diagnosis (13.0% versus 17.0%, P = 0.05) compared with the pre-reforms phase (Table 3). Despite similar illness severity between the two groups, patients were less likely to require an ICU level of care (27.2% versus 18.5%, P < 0.01) during the post-reforms phase (Table 3).
Illness acuity.
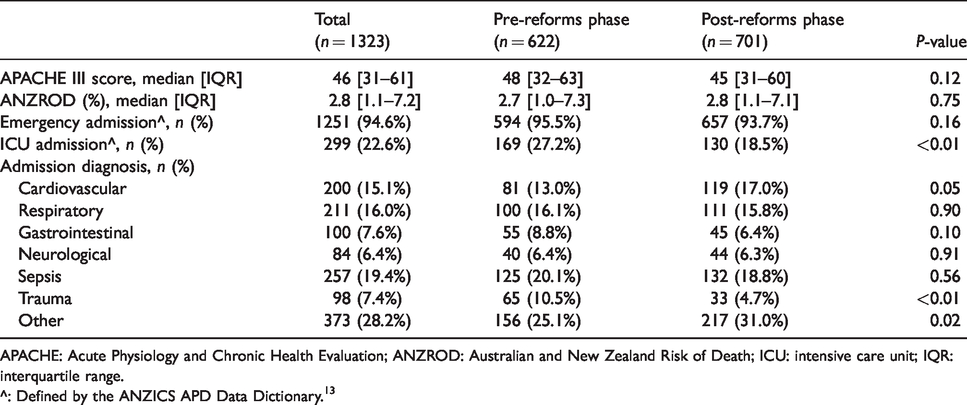
APACHE: Acute Physiology and Chronic Health Evaluation; ANZROD: Australian and New Zealand Risk of Death; ICU: intensive care unit; IQR: interquartile range.
^: Defined by the ANZICS APD Data Dictionary.13
Discussion
The proportion of ICU admissions associated with alcohol misuse reduced after the implementation of the alcohol reform policies in September/October 2018. The decline in admissions associated with acute alcohol misuse was more marked than that with chronic alcohol misuse. This is to be expected given the sudden implementation of restrictions and the relatively short time frame analysed. Based on this initial trend, we anticipate that the rate of admissions associated with chronic alcohol misuse may decrease further if alcohol reforms remain in place.
The difference in age at admission between the pre-reforms and post-reforms phases was consistent with a reduction in ICU admissions associated with acute alcohol misuse. This is in keeping with findings that those who engage in risky drinking on a single occasion tend to be young adults 21 and with an earlier study from our unit that showed that patients who had an admission associated with alcohol misuse were younger.3
Given the well-established causal link between alcohol misuse and trauma22,23 it was unsurprising that the rate of ICU admissions with a diagnosis of trauma reduced following the introduction of stricter alcohol regulations. This finding is also in keeping with data from Central Australia that showed higher rates of trauma to be a primary ICU admission reason in patients who misused alcohol.3 Given that the NT has the highest rates of alcohol-related road accidents 1 and the highest rate of death and hospital presentations secondary to injuries from alcohol in Australia, 24 our finding that the implementation of alcohol harm minimisation policies was associated with a reduction in ICU trauma admissions is an important one.
Despite the evidence regarding alcohol-induced immunosuppression25–27 and a previous human study that has shown that chronic alcohol use is an independent risk factor for the development of sepsis, 28 there was no change in the rate of sepsis amongst ICU admissions after the implementation of new alcohol restrictions.
Admissions associated with alcohol misuse consume ICU resources. In particular, alcohol misuse has been shown to be associated with an increased need for mechanical ventilation,3,29 a longer duration of mechanical ventilation 30 and increased ICU LOS.3,31,32 In keeping with this, it was expected that ICU resource use would decrease in the post-reforms phase, mirroring the decrease in ICU admissions associated with alcohol misuse during this period. While there was a significant reduction in the duration of mechanical ventilation, the proportion of patients requiring mechanical ventilation was only slightly reduced and not statistically significant. There was a decrease in ICU LOS, which represents a reduction of a cumulative 234 patient-days. It is likely that this represents a considerable cost saving.
The argument that our findings are directly attributable to the implementation of stricter alcohol regulations is supported by similar findings elsewhere. Observational studies following the introduction of minimum unit pricing for alcohol overseas have shown a substantial reduction in alcohol consumption 33 and that the greatest reduction in alcohol use (as inferred by quantity of alcohol purchased) is amongst those who drink the most alcohol. 34 While there has been little research into the effectiveness of point-of-sale interventions such as the PALIs or a BDR, data relating to alcohol-related harm following the implementation and withdrawal of old incarnations of these laws in Alice Springs are highly suggestive of their effectiveness in reducing alcohol-related harm. Following the dismantling of the BDR in 2012, alcohol-related presentations to the ASH emergency department increased by 80% over the next 14 months 35 and there were increases in alcohol-related offences, domestic assaults and admissions to the sobering-up shelter. 9 There was a subsequent decrease in these same measures when TBLs, a precursor to the role of PALIs, were introduced to Alice Springs in 2014. 9
Our study has limitations. First, it was not possible with this data to determine the impact of each individual alcohol reform given the close temporal frame in which they were implemented, nor did our data encompass the period in which the BDR was reintroduced. In addition to the introduction of an MUP, PALIs and the BDR, there were also new alcohol restrictions relating to takeaway alcohol sale hours and quantities introduced in the Tennant Creek/Barkly Region in February 2018 in response to the rising rates of alcohol-related harm in the area. 36 The Barkly Region is part of the catchment area for ASH ICU and these regional legislation changes may have had an impact on rates of ASH ICU admissions associated with alcohol misuse. Given that these changes were implemented during the pre-reforms phase of our study, one could speculate that this may have reduced the magnitude of the reduction in alcohol misuse seen in the post-reforms phase. Second, the definition for misuse may not have captured all admissions in which alcohol was a contributing factor. It was anecdotally noted during data collection that there were many patients who did not meet criteria for misuse due to their presenting in the days that followed injury sustained while intoxicated. Further, our definition of acute alcohol abuse also did not capture admissions in which the alcohol misuse of another person was a contributing factor (e.g. the passenger in a motor vehicle accident where the driver was intoxicated). It is therefore likely that our data underestimated the proportion of patients who have an ICU admission associated with alcohol misuse. Third, although an interrupted time series design is amongst the strongest of the quasi-experimental approaches for the longitudinal evaluation of an intervention (or interventions), most observational designs overestimate effect size, even when the direction of effect is correct, plausible and consistent with the findings of other researchers.
Further research, in particular analysis of admissions associated with alcohol misuse at Royal Darwin Hospital ICU, may help in elucidating the impact of individual alcohol reforms given that an MUP and BDR, but not PALIs were introduced in the Darwin region.
Conclusions
Following the introduction of alcohol legislation reforms in Central Australia, in particular an MUP, PALIs and the BDR, there was a 38% relative reduction in ICU admissions associated with alcohol misuse as well as a marked reduction in trauma admissions.
ICU outcomes are only one measure of alcohol-related harm, and, when considering the effectiveness of new policies, other measures should be scrutinised such as emergency department presentations, crime statistics and road accident data. It will be important to continue to analyse ICU admission patterns and resource use over time to better understand the long-term impacts of these reforms.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20977503 - Supplemental material for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20977503 for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study by Carly Wright, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing original draft, Writing review editing, Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Validation, Writing review editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review editing in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-2-aic-10.1177_0310057X20977503 - Supplemental material for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study
Supplemental material, sj-pdf-2-aic-10.1177_0310057X20977503 for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study by Carly Wright, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing original draft, Writing review editing, Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Validation, Writing review editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review editing in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-3-aic-10.1177_0310057X20977503 - Supplemental material for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study
Supplemental material, sj-pdf-3-aic-10.1177_0310057X20977503 for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study by Carly Wright, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing original draft, Writing review editing, Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Validation, Writing review editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review editing in Anaesthesia and Intensive Care
Supplemental Material
sj-pdf-4-aic-10.1177_0310057X20977503 - Supplemental material for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study
Supplemental material, sj-pdf-4-aic-10.1177_0310057X20977503 for The effect of alcohol policy on intensive care unit admission patterns in Central Australia: A before–after cross-sectional study by Carly Wright, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing original draft, Writing review editing, Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Validation, Writing review editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing review editing in Anaesthesia and Intensive Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.