
Abstract
Avoiding hypoxaemia is considered crucial in cardiac surgery patients admitted to the intensive care unit (ICU). However, avoiding hyperoxaemia may also be important. A conservative approach to oxygen therapy may reduce exposure to hyperoxaemia without increasing the risk of hypoxaemia. Using a before-and-after design, we evaluated the introduction of conservative oxygen therapy (target SpO2 88%–92% using the lowest FiO2) for cardiac surgical patients admitted to the ICU. We studied 9041 arterial blood gas (ABG) datasets: 4298 ABGs from 245 ‘conventional’ and 4743 ABGs from 298 ‘conservative’ oxygen therapy patients. During mechanical ventilation (MV) and while in the ICU, compared to the conventional group, conservative group patients had significantly lower FiO2 exposure and PaO2 values (P < 0.001 for each). Accordingly, using the mean PaO2 during MV, more conservative group patients were classified as normoxaemic (226 versus 62 patients, P < 0.01), fewer as hyperoxaemic (66 versus 178 patients, P < 0.01) and no patient in either group as hypoxaemic or severely hypoxaemic. Moreover, more ABG samples were hyperoxaemic or severely hyperoxaemic during conventional treatment (P < 0.001). Finally, there was no difference in ICU or hospital length of stay, ICU or hospital mortality or 30-day mortality between the groups. Our findings support the feasibility and physiological safety of conservative oxygen therapy in patients admitted to ICU after cardiac surgery.
With more than a million cases annually worldwide, cardiac surgery is a leading reason for admission to an intensive care unit (ICU).1–3 Oxygen therapy for these patients begins in the operating room and continues until ICU discharge. In the ICU, the conventional approach to oxygen therapy is to target oxygen saturation (SpO2) levels of >96%.4,5 However, while throughout the perioperative period avoiding hypoxaemia is considered fundamental, there are growing concerns over hyperoxaemia, with particular regard to oxidative stress, cardiopulmonary bypass (CPB)–related myocardial ischaemia/reperfusion injury and pulmonary inflammation.4–7 Such concerns suggest the need for a conservative approach to oxygen therapy.
Conservative oxygen therapy is defined as the targeting of an SpO2 between 88% and 92% using the lowest possible fraction of inspired oxygen (FiO2) for mechanically ventilated patients. In undifferentiated ICU patients, this approach has been shown to markedly decrease exposure to hyperoxaemia, while being free of adverse physiological and clinical outcomes. 8 However, whether a conservative approach to oxygen therapy would be feasible and safely reduce exposure to hyperoxaemia in cardiac surgery patients following admission to the ICU, is unknown.
Accordingly, we sought to evaluate the impact of implementing a conservative oxygen therapy approach on physiological as well as patient-centred outcomes in patients admitted to the ICU after cardiac surgery. We hypothesised that, in cardiac surgery patients, conservative oxygen therapy would be feasible and safe and would reduce the exposure of such patients to hyperoxaemia.
Materials and methods
Design
We performed an uncontrolled before-and-after study in the 22-bed multidisciplinary ICU of a tertiary care hospital located in Melbourne, Victoria. We included all consecutive cardiac surgical patients admitted from 1 January, 2013 to 31 October, 2013 (the conventional oxygen therapy period) and 1 January, 2014 to 31 October, 2014 (the conservative period), with a dedicated educational period from 1 November, 2013 to 31 December, 2014. Prospective ethical approval was obtained with a waiver of informed consent as this study was evaluating a unit-approved practice change to the oxygen saturation targets that applied to all admissions who required mechanical ventilation (MV) (approval number HREC/13/Austin/100). This study was also prospectively registered with the Australian New Zealand Clinical Trials Registry (ACTRN12613001322729). Based on historic admission rates for cardiac surgical patients in our ICU we estimated that approximately 250 patients would be evaluated for each period.
Intervention
Cardiac surgical patients admitted to the ICU during the study periods were included. During both periods patients were mechanically ventilated with an AVEA ventilator (CareFusion, Yorba Linda, CA, USA) or an Evita ventilator 4, Evita XL (Drägerwerk AG, Lübeck, Germany).
During the conventional period, oxygenation goals for each patient were prescribed by their bedside clinicians, and data were recorded by a research staff member who reviewed each cardiac surgical patient. A run-in period was then undertaken that provided education on conservative oxygen therapy to all ICU staff. During the intervention period, ICU clinicians targeted an SpO2 level between 88% and 92% using the lowest possible FiO2 during the period of MV for all cardiac surgical patients. The intervention period applied only to the period of MV, as the FiO2 is known and can be titrated. There was no change to the oxygen therapy practice for patients before or during their operation.
Data extraction
For each patient, using their primary admission to ICU following cardiac surgery, we collected information on baseline demographics (age, sex, body weight, preoperative creatinine, EuroScore) and surgical characteristics (type of surgery, duration of bypass). Simultaneously, we collected arterial blood gas (ABG) data from samples obtained over the patient’s entire ICU admission. Blood gas analysis was performed with ABL800 FLEX (Radiometer, Copenhagen, Denmark). In addition, we obtained data on duration of MV while in the ICU; need for continuous renal replacement therapy (CRRT); ICU and hospital length of stay; ICU and hospital mortality; and 30-day mortality.
Outcomes
The primary outcomes were change in PaO2 and FiO2 during MV.
Secondary outcomes included: (a) PaO2 and FiO2 during changes throughout the ICU admission; (b) the proportion of ABGs and patients classified as having severe hypoxaemia (<55 mmHg), hypoxaemia (55–60 mmHg), normoxaemia (60–120 mmHg), hyperoxaemia (120–300 mmHg) and severe hyperoxaemia (>300 mmHg); (c) duration of MV; (d) ICU and hospital length of stay; (e) hospital discharge status (alive versus dead); and (f) 30-day mortality.
Statistical analysis
Continuous variables were summarised using median and interquartile range (IQR) as appropriate, and categorical variables using number (percentage). The Mann–Whitney U-test was used for comparison between continuous variables and the chi-squared test or Fisher’s exact test for comparisons between categorical variables. Changes over time of PaO2 and FiO2 for each study period were tested by repeated measures analysis of variance (RM-ANOVA) using time as the repeated measures variable. Associations of baseline characteristics and conservative oxygen therapy with 30-day mortality were evaluated by univariable and multivariable logistic regression analysis. As the dependent variables of ICU and hospital length of stay were non-parametric, multivariable linear regression analyses using log-transformation were used. Covariates with P < 0.10 in the univariate analysis were included in the multivariable model. In the final analyses, a two-sided P-value <0.01 was considered statistically significant. All statistical analyses were performed with SPSS version 19.0 (SPSS Inc., Chicago, IL, USA).
Results
Demographic characteristics
We included 543 patients: 245 patients from the before period and 298 patients from the after period. Overall, 388 (71.5%) patients were male, their median age was 66 years (IQR 57–74 years), 320 (58.9%) patients had coronary artery bypass grafting (CABG), 140 (25.8%) valve surgery only, 53 (9.8%) combined valve and CABG, and 30 (5.5%) underwent a different type of cardiac surgical procedure. The two groups had similar baseline and surgical characteristics (Table 1).
Baseline characteristics of study patients and processes of care during mechanical ventilation.
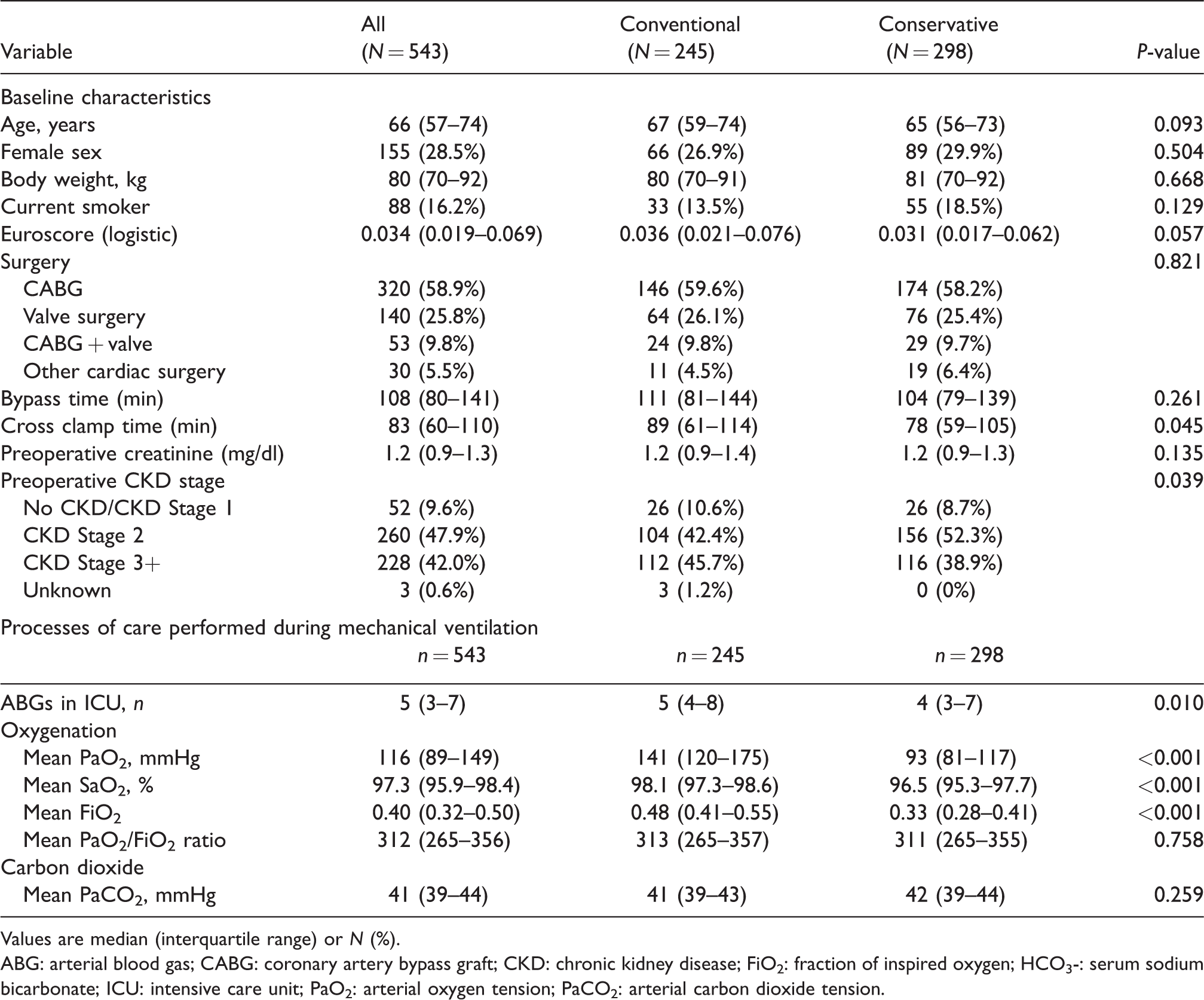
Values are median (interquartile range) or N (%).
ABG: arterial blood gas; CABG: coronary artery bypass graft; CKD: chronic kidney disease; FiO2: fraction of inspired oxygen; HCO3-: serum sodium bicarbonate; ICU: intensive care unit; PaO2: arterial oxygen tension; PaCO2: arterial carbon dioxide tension.
Process of care characteristics and oxygenation changes for patients during MV are shown in Table 1 and for the overall ICU admission in Appendix Table 1.
During MV, we assessed 5015 ABGs: 2397 from patients in the conventional therapy group and 2628 from patients in the conservative therapy group. We assessed 5025 ABGs: 2397 from patients in the conventional therapy group and 2628 from patients in the conservative therapy group. The median number of ABGs during ICU admission was 10 (IQR 7–17). During MV, there was a decrease in number of ABGs between the groups with 4 (3–7) in the conservative therapy group versus 5 (3–7) in the conventional therapy group (P=0.01) (Table 1), with a similar pattern in the number and distribution of ABGs over the ICU admission (Appendix Table 1).
Comparison of patient oxygenation management in the ICU
There were differences between the groups in relation to FiO2 values and PaO2 exposure during MV (P < 0.01) (Table 1) and throughout the entire ICU admission (P < 0.01) (Appendix Table 1). Compared to the conventional period, FiO2 and PaO2 values were significantly lower in the conservative group over the first 10 hours in ICU (P < 0.001, respectively) (Figures 1 and 2). The mean PaO2/FiO2 ratio was similar for both groups during the period of MV (P = 0.75).
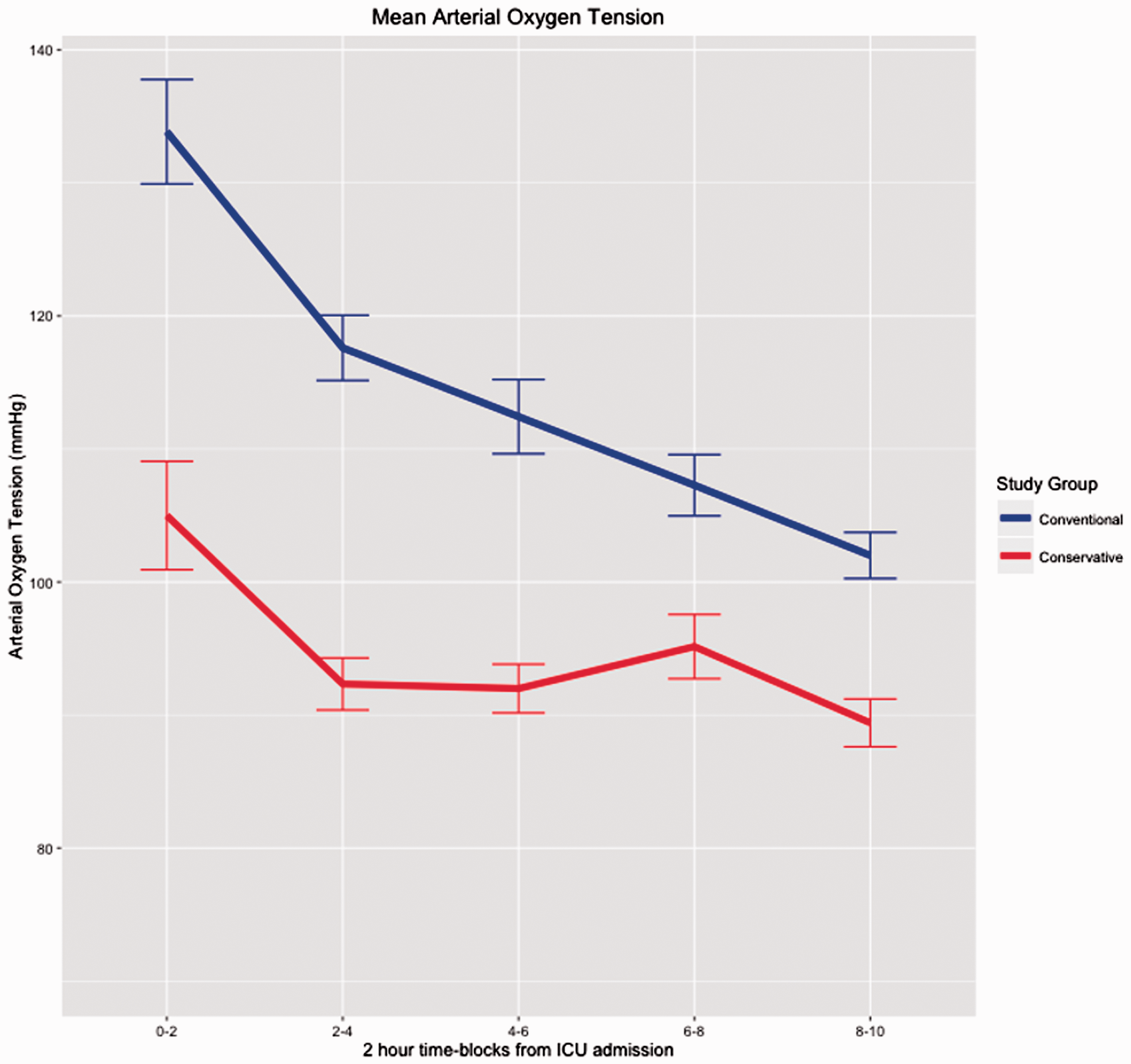
Change in PaO2 over time in the first 12 hours for the conventional and conservative oxygen therapy group patients, expressed as median values for every 2-hour period. Blue line indicates the conventional therapy group, and red line indicates the conservative therapy group. Values are mean and error bars indicate the standard error. Repeated measures analysis of variance: P < 0.001.
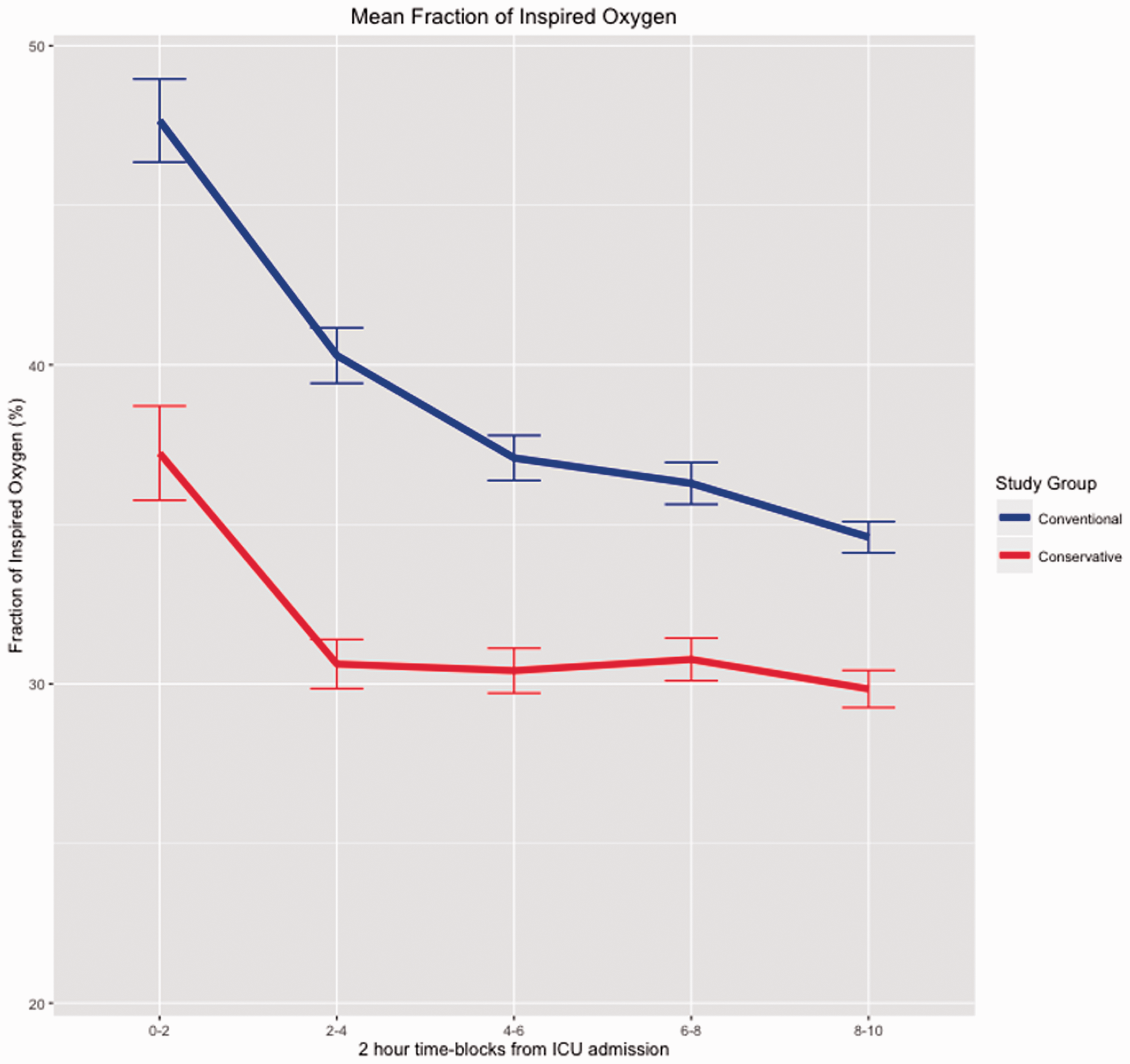
Change in FiO2 over time in the first 12 hours for the conventional and conservative oxygen therapy group patients, expressed as median values for every 2-hour period. Blue line indicates the conventional therapy group, and red line indicates the conservative therapy group. Values are mean and error bars indicate the standard error. Repeated measures analysis of variance: P < 0.001.
ABG classification into O2 groups
During MV, 3717 (74%) of ABGs were classified as normoxaemic and 863 (17.2%) as hyperoxaemic. Moreover, the conservative group had more ABGs classified as normoxaemic (79.2% versus 68.2%, P < 0.001) and fewer as hyperoxaemic (13.4% versus 21.3%, P < 0.001) compared to the conventional group (Table 2). Fewer ABGs in the conservative group were in the severe hyperoxaemia range (Table 2).
Classification into O2 groups based on arterial blood gas data together with mean and time range of PaO2 values during mechanical ventilation.
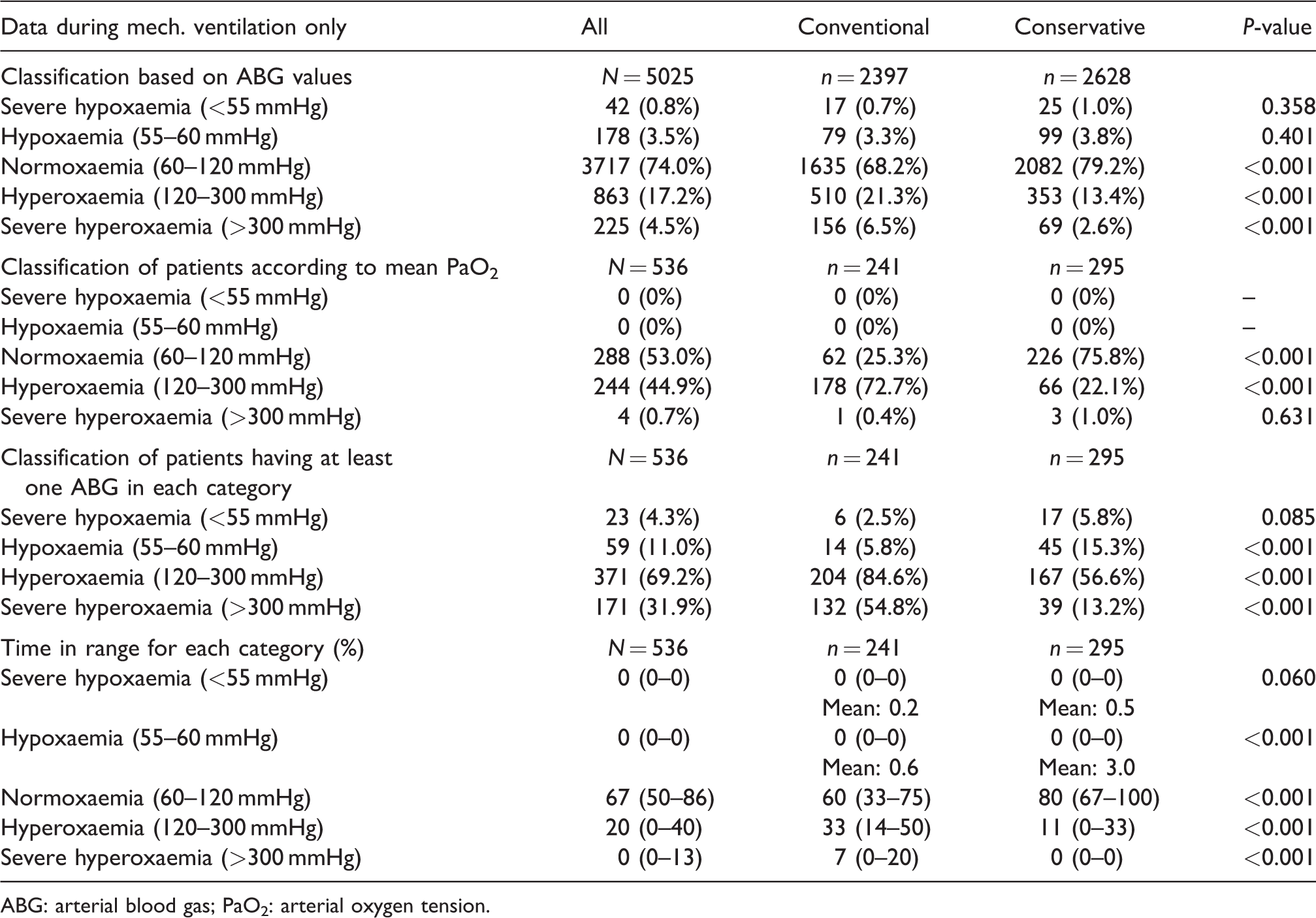
ABG: arterial blood gas; PaO2: arterial oxygen tension.
Of all ICU ABGs taken, 7083 (78.3%) of ABGs were classified as normoxaemic and 1275 (14.1%) as hyperoxaemic. Significantly, more ABGs in the conservative therapy group were classified as normoxaemic (81.5% versus 74.8%, P < 0.001) and fewer as hyperoxaemic (11% versus 17.5%, P < 0.001) compared to the conventional group (Table 2). Moreover, more ABGs were in the mild hypoxaemic range in keeping with the targeting of an SpO2 of 88% to 92% (Appendix Table 2).
Patient classification into O2 groups
During MV, using the mean PaO2 of all ABGs, 288 (53%) patients were classified as normoxaemic and 244 (44.9%) as hyperoxaemic. More conservative therapy group patients were classified as normoxaemic (226 versus 62 patients, P < 0.001) and fewer as hyperoxaemic (66 versus 178 patients, P < 0.001) than those in the conventional group (Table 2). No patient in either group was classified as having hypoxaemia or severe hyperoxaemia (Table 2).
According to the mean PaO2 of all ICU ABGs, 400 (73.3%) patients were classified as normoxaemic and 143 (26.3%) as hyperoxaemic. More conservative therapy group patients were classified as normoxaemic (264 versus 136 patients, P < 0.001) and fewer as hyperoxaemic (34 versus 109 patients, P < 0.001) than those in the conventional group (Appendix Table 2). No patient in either group was classified as having hypoxaemia or severe hyperoxaemia (Appendix Table 2).
Clinical outcomes
While non-significant, there was a pattern toward a shorter duration of MV in the conservative group patients (P=0.06). There was no significant difference in the need for CRRT, ICU or hospital length of stay, ICU or hospital mortality and 30-day mortality between the groups (Table 3).
Patient outcomes.
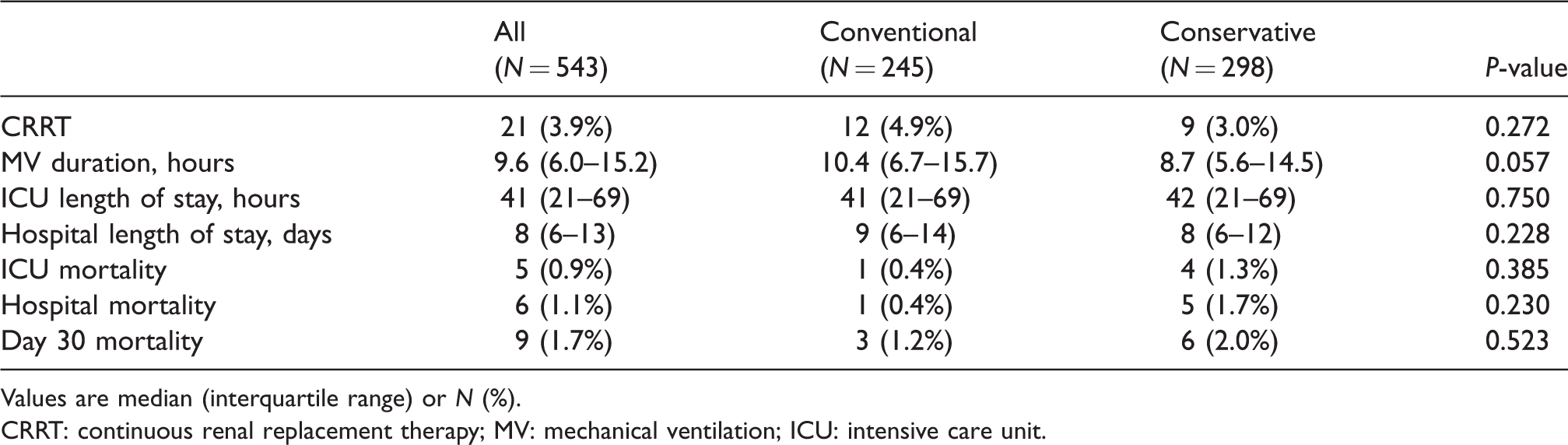
Values are median (interquartile range) or N (%).
CRRT: continuous renal replacement therapy; MV: mechanical ventilation; ICU: intensive care unit.
On univariate or multivariable linear regression analysis, conservative oxygen therapy was not associated with MV duration, ICU length of stay or hospital length of stay (Appendix Table 3).
Discussion
Key findings
Using a before-and-after design, we studied the impact of introducing a conservative oxygen therapy strategy in cardiac surgery patients admitted to the ICU. As expected, there were clear differences in PaO2 and FiO2 during MV and over the course of the ICU admission with a significant decrease in the occurrence of hyperoxaemic states, both when ABGs and patients were classified. However, during conservative oxygen therapy, we also found that fewer ABG values were in the severely hyperoxaemic range than in the conventional therapy period. In addition, in the conservative therapy period, lactate levels were lower with a pattern toward a shorter duration of MV. Finally, as a measure of safety, there were no differences in ICU, hospital or 30-day mortality outcomes for patients in either group.
Relationship with previous studies
To our knowledge, this is the first study using historical controls to investigate the biochemical, physiological and clinical impact of aiming for lower SpO2 targets during MV in cardiac surgery patients admitted to the intensive care unit. Our findings, however, are aligned with other studies evaluating the introduction of conservative oxygen therapy in other ICU patients.8,9 For example, in a multicentre randomised controlled trial where 103 patients from four different institutions were evaluated, the median time-weighted, PaO2 and FiO2 were significantly lower during the conservative oxygen therapy. In another study, there was a reduction in PaO2 and FiO2 over the course of MV, which was sustained over the ICU admission. 9
Systemic concerns over perioperative hyperoxaemia for cardiac surgical patients particularly relate to excessive free radical production, 10 exacerbation of ischaemic-reperfusion injury, 11 haemodynamic instability 12 and the development of cardiac surgery-associated multiorgan dysfunction.13,14 Evaluating the impact of avoiding hyperoxaemia during CPB on acute kidney injury (AKI), investigators in Australia and New Zealand randomised 298 patients to either usual care or a targeted PaO2 of 75–90 mmHg providing an SpO2 ≥97%. 14 This study revealed a sustained and significant reduction in mean PaO2, with a mean SpO2 of 97.2% in the intervention arm throughout CPB but no difference in the development of AKI or ICU and hospital length of stay. More recently, investigators in the Netherlands performed a single-centre randomised controlled trial evaluating targeted moderate hyperoxic versus near-physiological oxygen levels during and after cardiac surgery in 50 patients. Patients in the control group had a PaO2 target of 200–220 mmHg during CPB and 130–150 mmHg during ICU admission compared with the conservative group, which had a PaO2 target of 130–150 mmHg during CPB and 80–100 mmHg in the ICU. While exposure to hypo- and hyperoxaemic states was not reported, the time-weighted PaO2 during CPB was 220 mmHg versus 157 mmHg, and during ICU 107 mmHg versus 90 mmHg, respectively. Clearly, such studies do not explore true conservative oxygen therapy as the treated population was either in the conventional range or even in the hyperoxaemic range. Our study, instead, takes the degree of conservative oxygen therapy much further and for a longer period and shows no evidence of harm.
High FiO2 concentrations have been associated with absorption atelectasis. This phenomenon appears to develop within minutes of breathing 100% oxygen. 15 Moreover, evidence from animal and human studies has shown spontaneous breathing during MV reduces intrapulmonary shunting and decreases atelectasis formation.16–18 We found a trend toward a shorter duration of MV during the conservative period, suggestive of a shorter period of mandatory ventilation. This finding is consistent with previous evidence in non-cardiac surgery patients reporting a decreased incidence and severity of atelectasis. As such it supports the notion that a more conservative approach to oxygen therapy may have some clinical advantages.9,15
Clinical implications
Our findings imply that in cardiac surgery patients admitted to ICU, it is feasible to introduce conservative oxygen therapy as a means of avoiding supranormal oxygen levels. They further imply that such a treatment strategy does not simply decrease the number of episodes of hyperoxaemia but can also decrease the number of episodes of severe hyperoxaemia. Moreover, our findings support the view that targeted oxygen delivery during admission to ICU, and particularly so during MV, is probably safe. Finally, they justify further investigation of conservative oxygen therapy in these patients.
Strengths and limitations
Our study has several strengths. To our knowledge, this is the first study to evaluate the impact of a truly conservative approach to oxygen therapy in MV cardiac surgical patients in ICUs. Clinicians were unaware of the study in the pre-intervention phase allowing standard care to remain unchanged, providing a control group that represented standard care in our institution. We studied a moderately large population and thousands of ABG samples lending a degree of robustness to our findings. We used all ABGs obtained during both periods without exclusion, thus attenuating both ascertainment and surveillance bias. Our ABG values and oxygen management during MV and ICU stay in the conventional treatment period are similar to those reported in the literature for such patients, implying a high degree of external validity. Finally, the characteristics of our patients are identical to those of similar patients having cardiac surgery in developed countries, providing a further degree of external validity.
Our study also carries some limitations. In a before-and-after study, only limited causal inferences can be drawn because the intervention period cannot be blinded. However, blinded studies of oxygen therapy are exceedingly difficult to conduct in intensive care, and all studies so far have been ‘open label’. In addition, our assessment of oxygen therapy was restricted to the period of MV in the ICU admission and did not include such factors as intraoperative oxygen administration or the delivery of supplemental oxygen to patients in the ward setting. Additionally, ABGs do not provide continuous data on the arterial saturation of oxygen, and thus, patients may have been exposed to ‘worse’ abnormal oxygen states prior to, during MV in the ICU or after ICU discharge, which were not identified in our study. Furthermore, the period of MV in our cohort may not have been long enough to detect any substantial effect. However, our findings still suggest that targeting such lower levels during MV and in the ICU does decrease the risk of exposure to hyperoxaemia and that such avoidance, possibly through increased surveillance, also leads to increased prevalence of normoxaemia. Whether the potential benefits of a decrease in hyperoxaemia and an increase in normoxaemia offset the potential harm of hypoxaemia remains uncertain. We further acknowledge that our target of an SpO2 of 88% to 92% was lower than in previous studies. The decision to extend the lower limit of SpO2 represented a consensus view of clinicians that it would provide a broader target range and would still be safe. Our findings support this view and have led to the design of a randomised controlled trial. 19 Future adequately powered randomised controlled trials, however, are required to test the robustness of these findings over longer durations of MV, in other institutions and health system settings and to ascertain whether such physiological gains translate into clinical benefits.
Conclusions
In our exploratory before-and-after study of cardiac surgical patients admitted to the ICU, we found that conservative oxygen therapy was feasible, did not result in an increased incidence of severe hypoxaemia and led to a significant decrease in exposure to hyperoxaemia. Further investigations of conservative oxygen therapy and its impact on patient-centred outcomes in this group are warranted.
Supplemental Material
Supplemental material for Conservative versus conventional oxygen therapy for cardiac surgical patients: A before-and-after study
Supplemental Material for Conservative versus conventional oxygen therapy for cardiac surgical patients: A before-and-after study by Glenn M Eastwood, Matthew J Chan, Leah Peck, Helen Young, Johan Mårtensson, Neil J Glassford, Hidetoshi Kagaya, Satoshi Suzuki, Sean Galvin, George Matalanis and Rinaldo Bellomo in Anaesthesia and Intensive Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Anaesthesia Intensive Care Trust Fund, Austin Hospital, Melbourne, Victoria.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.