
Abstract
The COVID-19 pandemic has required intensive care units to rapidly adjust and adapt their existing practices. Although there has a focus on expanding critical care infrastructure, equipment and workforce, plans have not emphasised the need to increase digital capabilities. The objective of this report was to recognise key areas of digital health related to the COVID-19 response. We identified and explored six focus areas relevant to intensive care, including using digital solutions to increase critical care capacity, developing surge capacity within an electronic health record, maintenance and downtime planning, training considerations and the role of data analytics. This article forms the basis of a framework for the intensive care digital health response to COVID-19 and other emerging infectious disease outbreaks.
Keywords
Introduction
Digital health combines technology and digital information to support the delivery of healthcare. Many intensive care units (ICUs) have introduced electronic health records (EHRs) to collate clinical documentation, test results and biomedical data into a single digital platform. These platforms are now a repository for rich and detailed clinical information, which can be aggregated and analysed to improve care, detect adverse safety signals and rapidly facilitate clinical research. 1 , 2 Although the cost-effectiveness remains a much debated issue, ICUs have increasingly embraced these digital platforms, using real-time data and the clinical decision support tools as part of daily operations. 3
As health services expand their critical care capacity in response to the coronavirus disease (COVID-19) pandemic, it is therefore essential to consider the expansion and readiness of these digital platforms alongside the traditional focus on staff, beds and equipment.
We identify and discuss six focus areas within digital readiness relevant to critical care: (a) increasing critical care capacity; (b) increasing EHR surge capacity; (c) EHR maintenance; (d) downtime planning; (e) digital training; and (f) data analytics (Figure 1).
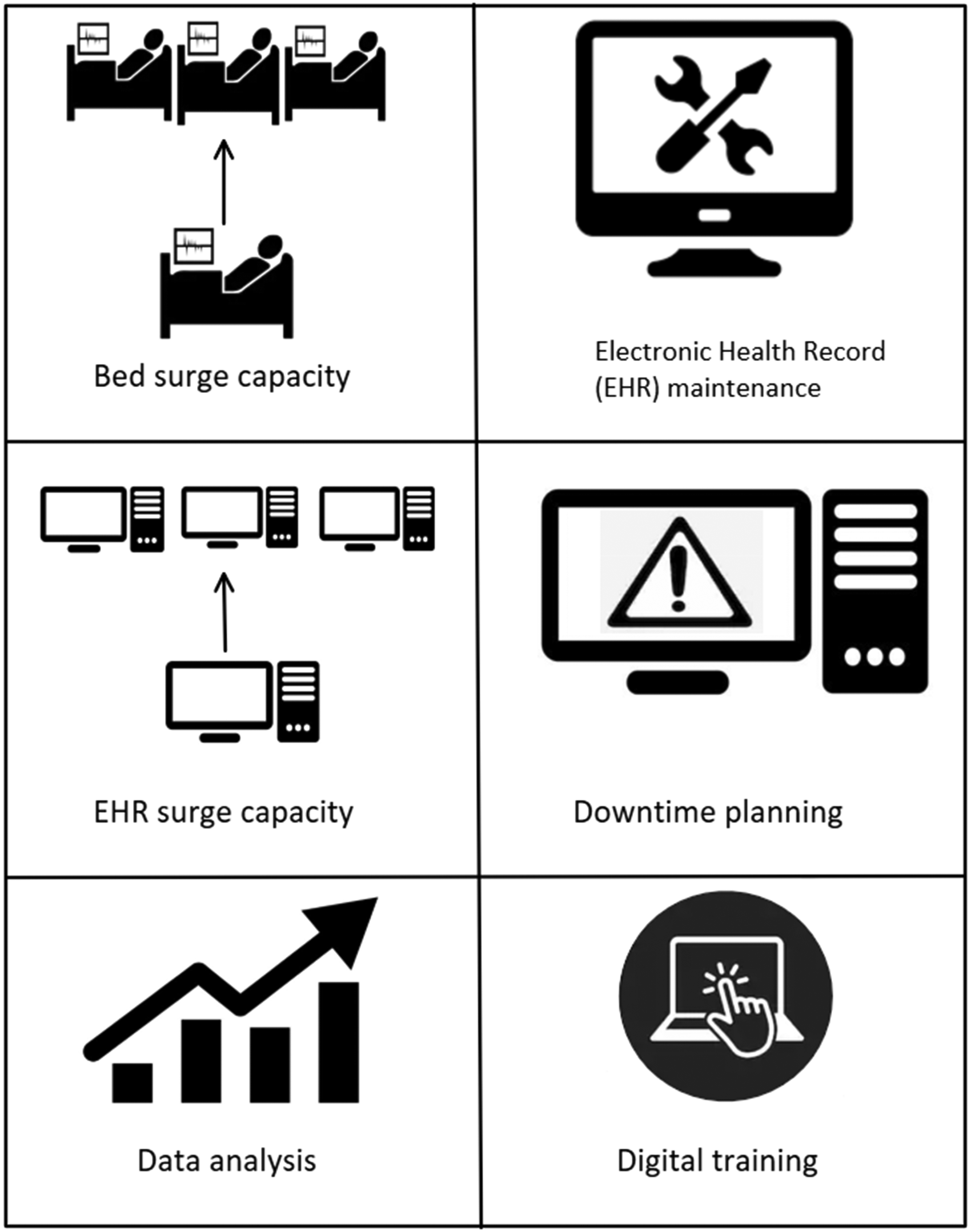
Six focus areas within digital readiness.
Increasing critical care capacity
Globally, intensive care societies, such as the Australian and New Zealand Intensive Care Society (ANZICS), have issued recommendations to help health services increase critical care capacity. 4 Critical care capacity includes bed spaces and staff. A rapid increase in capacity in both of these areas has significant digital implications.
Bed spaces
There is a range of digital readiness solutions required for ICU bed spaces. Bed spaces may be classified into three digital tiers (Figure 2). Tier 1 beds are fully integrated beds and already exist within the EHR database but may not be in current use. Tier 2 beds are additional beds implemented within the ICU complex that require deployment of additional biomedical devices (e.g. physiological monitors, ventilators). These additional devices may not be connected to central patient monitoring or to the network, so all biomedical information will be entered manually. Tier 3 beds are added outside the ICU complex in areas such as operating theatres and recovery facilities that can be readily transformed into facilities appropriate for critical care. 4
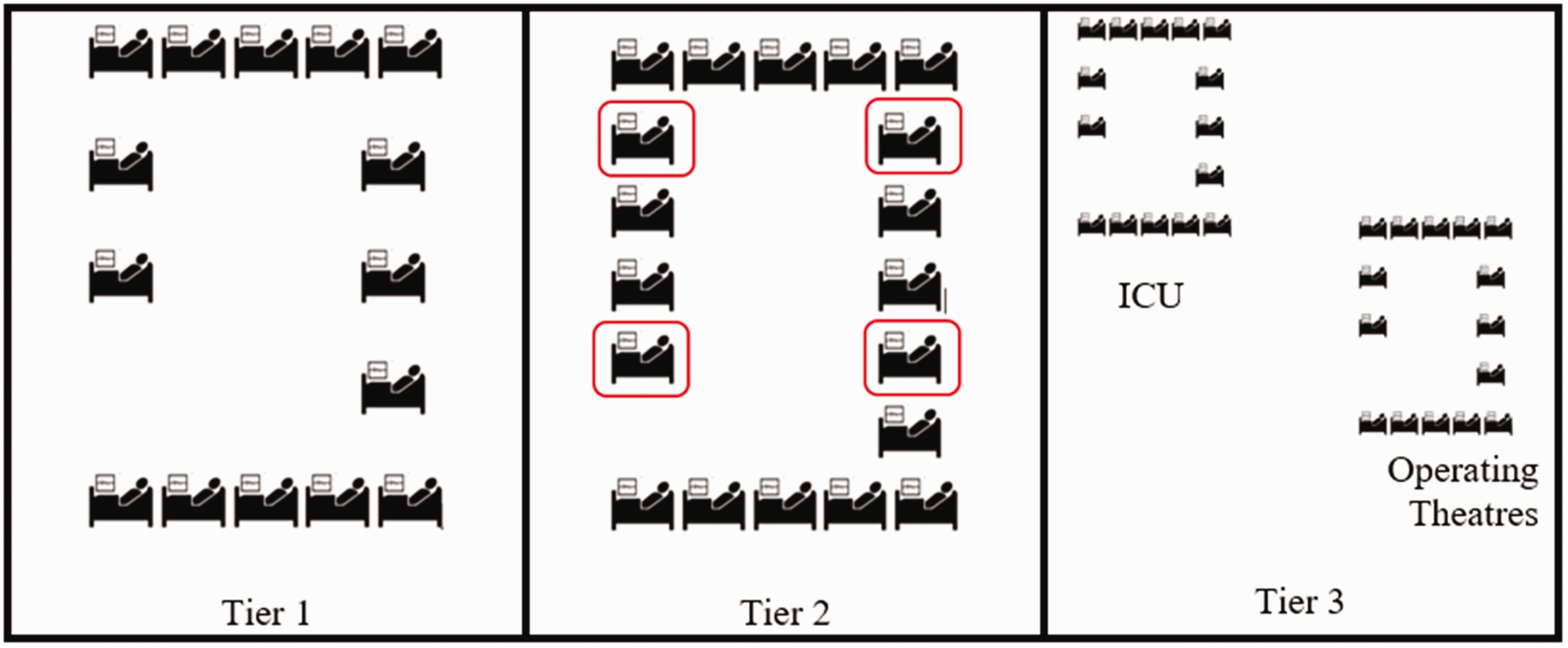
Surge capacity for intensive care units.
Staff
The ANZICS guidelines include strategies to increase the ICU workforce rapidly, acknowledging that this is a significant challenge for Australian remote, rural and regional health services. 4 Many such hospitals rely on a small cohort of intensive care specialists, usually supported by anaesthetic specialists, to provide medical oversight of the ICU. Jurisdictional pandemic preparation must include plans for the absence of key staff, including maintaining intensive care specialist support.
As all healthcare services seek to balance this surge in critical care activity and the ongoing management of patients with chronic diseases, with a need to reduce the risk of the nosocomial spread of COVID-19, virtual models of care have gained prominence.
Traditional telehealth models use two high-quality videoconferencing systems, one at each site, with licensed software providing secure communications. 5 A virtual consultation service can be staffed remotely, allowing staff quarantining at home after exposure to COVID-19 6 to contribute.
The College of Intensive Care Medicine (CICM) has guidelines to support virtual consultations. They specify three key categories:
The provision of intensive care specialist support to an ICU staffed by non–CICM Fellows. The provision of intensive care specialist support to remote centres for the management of patients awaiting retrieval to an ICU or a higher level ICU. The provision of intensive care specialist support out of hours when 24-hour a day critical care specialist cover cannot be provided on site.
7
As the demand on telehealth systems increases across all areas of healthcare, and provisioning additional systems with licences is time consuming, alternative models must be explored. Possibilities include utilising computers with built-in webcams and off-the-shelf videoconferencing systems such as Microsoft’s Skype for Business and Teams. Consumer-grade applications, such as Google Duo and FaceTime, do not currently fulfil the rigorous information security requirements for healthcare applications; 5 , 8 however, these restrictions should be weighed against the immediate risks to patients and a temporary waiver for the pandemic period considered.
Ideally the remote site, defined as the entity providing the virtual consultation, 8 will provide contemporaneous documentation—this may be achieved by remote access to an EHR; however, alternative methods of sharing information, such as emailing scanned notes, should be in place.
Information security is an important consideration: access should be secured, with a minimum of two-factor authentication, and when possible through a virtual private network (VPN). Prompt approvals and set-up for staff is essential.
Increasing EHR surge capacity
In order to maintain current levels of care, ICUs should use their EHR throughout the expanded ICU. This preserves standards for documentation of observations and notes, maintains prescribing safety and the ability for staff to work remotely.
As Tier 1 beds are fully integrated existing bed spaces, these beds are easily activated. Tier 2 and 3 bed spaces do not exist virtually, so they must be added to the EHR configuration. As ICUs aim to triple critical care bed capacity, 9 site configurations will alter substantially as the additional beds will remain permanently configured. Sites should use a standard naming convention to identify surge beds clearly and consider building separate virtual units for Tier 3 beds. All additional beds must also be added to the hospital patient administration system.
The additional device requirements will vary by site and include biomedical devices, handheld devices and bedside computers or ‘workstation on wheels’ with spare batteries and chargers. 10 Sourcing additional devices quickly is a major logistical challenge. These devices must undergo cleaning before and after redeployment to minimise fomite spread. Ideally, all devices are tracked through the wireless network using a real-time location system, preferably linked to a comprehensive tracking and tracing decontamination log.
The computers will also require network access, either through wired data points or utilising wireless networks. While the latter is the preferred option for safety reasons, this may require an increased wireless network density. Accordingly, site surveys should be commissioned to confirm sufficient location-grade wireless network coverage is present.
EHR maintenance
ICUs rely heavily on the expertise of their EHR teams, which include clinical informaticians and technical staff. These key staff must be supported to work remotely—this requires secure VPN access with reliable internet connection for all EHR team members.
In addition, infrastructure requirements must be considered. This includes ensuring enough servers to support a surge in EHR traffic, with the increased burden estimated at 15 simultaneous users per ten additional beds. This mandates an early technical assessment of the network capacity and the EHR server and fail-over capacity to mitigate against catastrophic network and server failures.
The burden of real-time reporting on servers is significant and sites should consider a mirror database to allow real-time reporting without further adding to server traffic. A mirror database also provides additional redundancy in the form of a fail-over database.
Downtime planning
All sites require procedures in place for the failure of their EHR, or downtimes. These are best supported by downtime viewers: computers wired directly to a printer with standardised note sets, including a medication record, which can be printed during a downtime. Downtime plans will need to be reviewed to incorporate changes to physical locations of bed spaces and staffing.
In the context of the anticipated prolonged response to the COVID-19 pandemic, the likelihood of a downtime must be considered. Given that non-ICU staff may be deployed to ICUs to assist, the consequence of a downtime requiring reversion to paper is considered major. Additional downtime viewers should be proactively deployed to ensure all new surge bed spaces have adequate downtime equipment.
Digital training
Staff who do not usually work in ICUs will be deployed to staff the additional critical care capacity. Many jurisdictions have a goal of one-to-one nursing of ventilated patients 11 , 12 so this deployment is predominantly nursing staff. New staff commonly receive on-site small-group EHR training delivered by the EHR team or designated educators. As staff are deployed at short notice, including out of hours, this approach is not sufficient. It is prudent to develop short, generic training videos demonstrating the key areas of documentation of notes, clinical observations and the prescription and administration of medications.
These training videos should be stored in a central and easily accessible repository. 10 More complex EHR interactions, if deemed necessary, can be supported by an ICU-trained nursing coordinator deployed within each area. 4
Training videos should include information on reactivating staff accounts and resetting forgotten passwords. As social distancing constraints prevent face-to-face meetings, staff will also benefit from training videos about videoconferencing applications.
Data analytics
Digital health makes it possible to collect and analyse data rapidly and easily. Data analytics ranges from simple reporting, such as aggregate and descriptive statistics, to more complex predictive modelling. Data analytics can be used to: (a) coordinate the critical care response at the institutional and multi-institutional levels; (b) monitor quality assurance indicators; and (c) facilitate research initiatives (Figure 3).
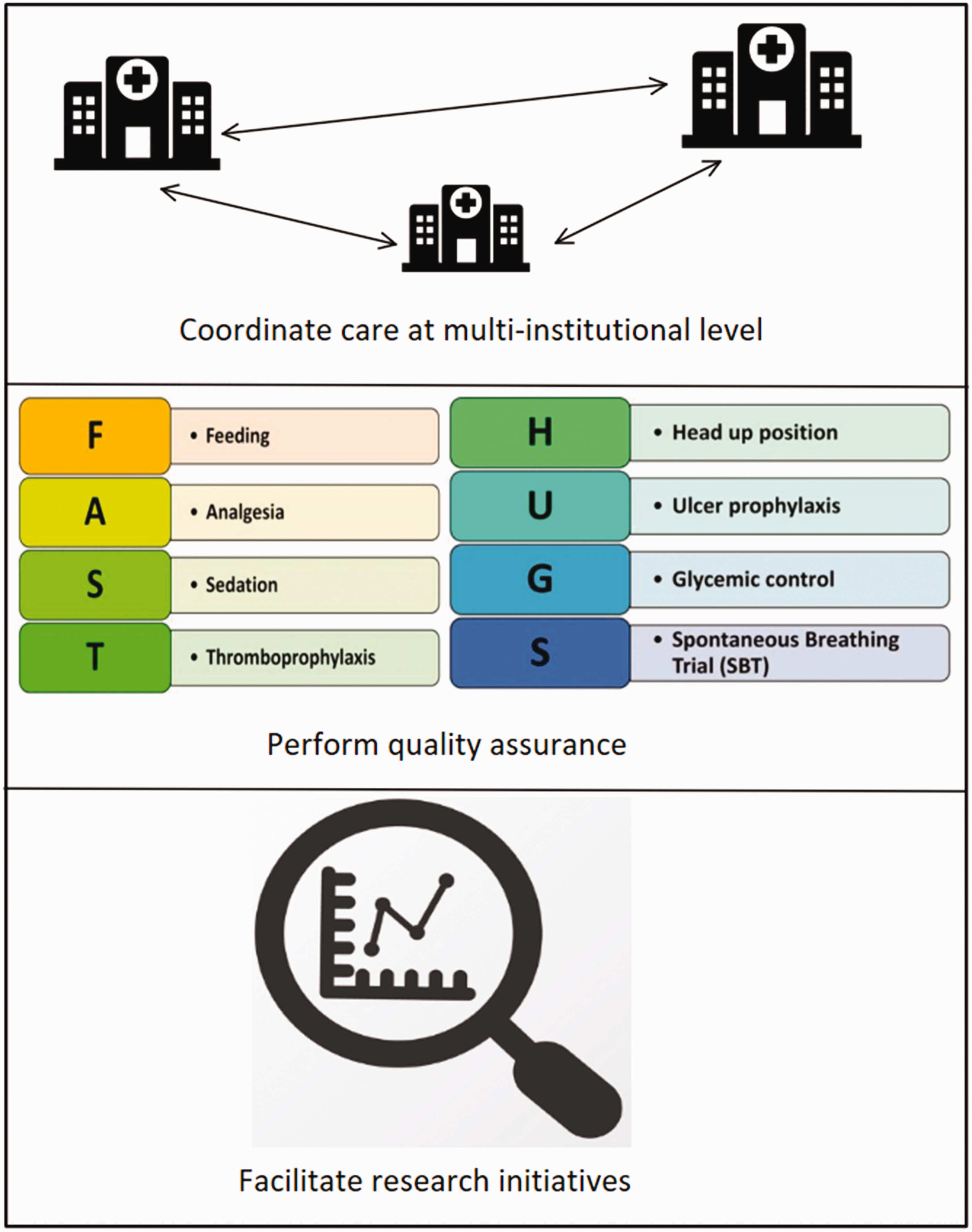
The role of data analytics in pandemics.
Data analytics to coordinate the critical care response
The surge in demand for critical care beds during the COVID-19 pandemic has shown significant geographical variation. 13 To achieve the best outcomes at a population level, critical care capacity must be considered at a multi-institutional level, also referred to as critical care networks, 14 and patients must be transferred from overwhelmed centres to those that have more capacity. 13
Current practice, which requires clinicians to make multiple phone calls in search of available ICU beds, is inefficient and distracts from patient care. The best use of critical care capacity will occur when clinicians have access to real-time ICU bed availability. Well-designed dashboards also include the number of infectious patients and the acuity or activity load of each ICU, as this allows better distribution of patients to maximise care delivery. 15
As workforce management is key during pandemics, real-time tracking of staff availability and staff absences is crucial. This information, when linked to real-time monitoring of emergency department presentations, ICU referral burden and the activity load of key areas, allows for considered redeployment of staff. Predictive analytics may provide opportunities for a seasonal-style staffing approach. 16
Data analytics to monitor quality assurance
Reports of healthcare staff working extra shifts during the COVID-19 pandemic are rife, with resulting physical and mental fatigue. 17 Fatigue and stress are well documented contributing factors to medical errors. 18 Real-time data analytics, combined with a highly customisable reporting structure, can support the delivery of high-quality care and reduce the cognitive load on staff, for example, using a ‘FASTHUG’ 19 report to confirm the presence of EHR orders for feeds, analgesia, sedative infusions, thromboembolism prophylaxis, stress ulcer prophylaxis and glucose control for each patient.
Data analytics and facilitating research initiatives
In the setting of a novel disease outbreak, rapid research is required to develop an evidence base for clinical care. This includes observational studies to identify high-risk patients and assess their recovery journey, as well as clinical trials of potential therapies. Conventional paper-based data collection is challenging, so EHRs can play a major role in facilitating rapid data collection.
A digital-ready ICU can pivot existing data collection tools rapidly to contribute to electronic surveillance and registry-embedded clinical trials. 20 , 21 Integration with existing registries and multi-jurisdictional data harmonisation, 22 as demonstrated by the SPRINT-SARI international hospital-based surveillance database project, 23 are key to success.
The digital-ready health service will bolster its data analytics and research teams to enable the swift introduction of approved complex observational studies and clinical trials. This requires streamlined data management processes and the ability to prioritise ethical and governance approvals.
During previous pandemics, complex predictive modelling could not be delivered to the clinician fast enough to impact care meaningfully. However, the increasing maturity of artificial intelligence techniques means that predictive modelling can now be rapidly developed, frequently updated and presented in easily understood graphical formats. 24 The ability to pinpoint which clinical variables contribute most to an artificial intelligence decision, known as feature importance, can result in the identification of a relatively small number of prognostic variables. This approach often outperforms traditional predictive tools.25–27 The COVID-19 Critical Care Consortium will use feature importance to collate the global data held within ECMOCard, a multicentre observational study of intensive care unit patients with COVID-19, 28 into a risk prediction tool to aid ICU clinicians during triage.
Conclusion
We highlight six key areas of importance for digital health within the critical care response to a pandemic such as COVID-19. We further discuss the role of data analytics related to crisis response coordination, quality assurance and research.
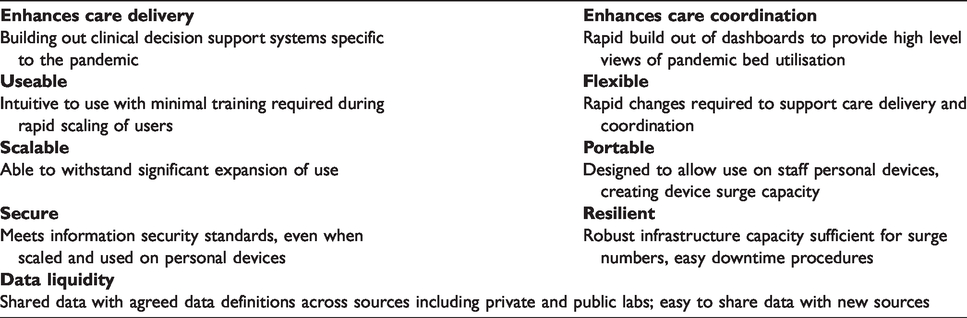
However, currently digital health systems are not mature enough to fulfil the wide range of expectations and a ‘disaster-ready’ digital health system (see Table 1) may not be achievable unless there is active engagement of all stakeholders to address the current issues.
Key attributes for disaster-ready electronic health records.
Footnotes
Acknowledgements
The authors acknowledge the contributions of Patrick Young, Nermin Karamujic, George Cornmell, Shane Townsend, Hamish Pollock, Jayshree Lavana and Jayesh Dhanani. Kiran Shekar acknowledges research fellowship support from Metro North Hospital and Health Service.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.