
Abstract
Peripheral nerve blocks can provide surgical anaesthesia as well as excellent postoperative analgesia. When questioned postoperatively, however, some patients report low levels of satisfaction with their nerve block experience. At our hospital, patients undergoing regional anaesthesia have their patient characteristics, block characteristics and postoperative feedback routinely recorded in a block registry. We analysed data from 979 consecutive patients undergoing peripheral nerve block for orthopaedic surgery to identify factors associated with low levels of patient satisfaction. The primary outcome was patient satisfaction with their peripheral nerve block (scale 1–5: 4–5 is ‘satisfied’, 1–3 is ‘not satisfied’). Eighty-nine percent (871/979) of patients reported being ‘satisfied’ with their block. Factors negatively associated with patient satisfaction were rebound pain (adjusted odds ratio (aOR) 0.19, 95% confidence interval (CI) 0.04 to 0.85 for moderate rebound pain; aOR 0.11, 95% CI 0.03 to 0.48 for severe rebound pain), discomfort during the block (aOR 0.37, 95% CI 0.16 to 0.82 for moderate discomfort; aOR 0.19, 95% CI 0.05 to 0.76 for severe discomfort) and pain in the post-anaesthesia care unit (aOR 0.30, 95% CI 0.17 to 0.55 for pain ≥8/10). Only 24% (26/108) of patients who reported being ‘not satisfied’ stated that they would be unwilling to undergo a hypothetical future nerve block. Rebound pain of at least moderate intensity, procedural discomfort of at least moderate intensity and severe pain in the post-anaesthesia care unit are all negatively associated with patient satisfaction. Of these factors, rebound pain occurs most frequently, being present in 52% (403/777) of our respondents.
Introduction
Peripheral nerve blocks (PNBs) can be used to provide regional anaesthesia for operations involving the upper or lower extremities. The benefits of PNBs include excellent postoperative pain relief, reduced opioid requirements, reduced postoperative nausea and vomiting, faster discharge from the post-anaesthesia care unit (PACU) and shorter length of stay in hospital. 1 Despite these short-term advantages, there is little evidence that PNBs provide any improvements in longer-term functional outcomes. 2 PNBs may therefore be thought of as a type of ‘business class pain management’ 3 (i.e. superior to the ‘economy class’ of systemic analgesia) that can be offered to patients who desire the benefits of regional anaesthesia and who also accept its risks and limitations.
In this context, it is hard to justify PNBs if patients report low levels of satisfaction. The vast majority of patients (94%) indicate that they are either satisfied or very satisfied with their PNB. 4 A similarly high proportion of patients (94.6%) indicate that they would be willing to undergo a repeat PNB in a hypothetical case of future surgery. 5 There are methodological limitations with assessing patient satisfaction using a unidimensional global rating scale. 6 Nevertheless, its simplicity and patient-centredness make it a useful metric for describing a patient’s perception of the value of regional anaesthesia in the research or quality assurance setting. 7
The correlation between patient satisfaction and willingness to undergo a repeat PNB is not self-evident. Most patients who are satisfied with their PNB will also report their willingness to undergo a repeat PNB. Surprisingly, however, the majority of patients who report dissatisfaction with their PNB will also report a willingness to undergo a repeat PNB.4,5 This suggests that willingness to undergo a repeat PNB, while illuminating in some respects, is an imperfect metric. Despite this, prior research has focused on identifying factors that are negatively associated with a patient’s willingness to undergo a repeat PNB. 5 This requires a patient to speculate about something that may happen to them in the future rather than make a subjective judgement about something that they have actually experienced. We opine that a greater focus on patient satisfaction following PNB may improve our collective understanding on this issue and lead to more patient-centred targets for quality improvement and research projects.
In this study, we seek to identify factors that are associated with patient satisfaction following PNB during orthopaedic surgery — in particular, those factors associated with low levels of patient satisfaction. We also seek to better examine the relationship between patient satisfaction and a patient’s stated willingness to undergo a hypothetical future PNB.
Materials and methods
The Royal Brisbane and Women’s Hospital (RBWH) has maintained a point-of-care registry from February 2015, containing the details of all PNBs performed by a dedicated regional anaesthesia service. This service utilises a block room/block team model of care, which has been described previously. 8 Data were entered contemporaneously at the time of the block and used primarily for quality assurance purposes, but also for long-term clinical follow-up of abnormal neurological findings. Ethics approval was sought prior to data analysis, and an ethics exemption was granted by the RBWH human research and ethics committee (LNR/2018/QRNBW/47772).
We conducted a retrospective analysis of all PNBs performed in association with upper limb or lower limb orthopaedic surgical operations between February 2015 and December 2018. We excluded central neuraxial blocks, blocks for non-orthopaedic surgical operations and analgesic blocks that were not performed in conjunction with a surgical operation. Data were collected for 15 pre-defined variables that spanned three domains — patient characteristics, block characteristics and postoperative feedback. All data were prospectively collected and entered into the registry, and the study was designed before any statistical analysis had occurred.
Patient characteristics were sex (male, female), age (<60 years, ≥60 years), body mass index (<40 kg/m2, ≥40 kg/m2) and American Society of Anesthesiologists physical status (ASA PS) (I–II, III–V). Block characteristics were operative region (upper limb, lower limb), purpose of block (postoperative analgesia, surgical anaesthesia), sedation (no sedation, sedation, general anaesthesia), principal proceduralist (anaesthetist, anaesthetic trainee), perineural catheter (yes, no) and immediate complication (yes, no).
Postoperative feedback characteristics were obtained in two ways. Firstly, the medical record was reviewed to ascertain the maximum numerical rating scale (NRS) for pain in the PACU (0, 1–4, 5–7, 8–10), opioid use in the PACU (yes, no) and anti-emetic use in the PACU (yes, no). Secondly, a follow-up phone call was made by a member of the anaesthetic department at least five days postoperatively to enquire about the ‘level of discomfort during the nerve block procedure’, which we termed procedural discomfort (none, mild, moderate, severe) and the ‘level of pain after the block wore off’, which we termed rebound pain (none, mild, moderate, severe). This phone call was also when feedback was given regarding how satisfied the patient was with their PNB experience (scale 1–5: 5 is ‘completely satisfied’) and willingness to undergo a hypothetical future PNB (yes, no).
The primary outcome was patient satisfaction with their PNB. Patients were defined as ‘satisfied’ if they reported a satisfaction score of 4–5; and ‘not satisfied’ if they reported a satisfaction score of 1–3. Data were summarised with count (n) and percentage (%) as they were all categorical measures. Associations between follow-up status and the 15 variables were examined using chi-square tests. Associations between patient satisfaction and the 15 variables were examined using binary logistic regression and effect estimates were reported as odds ratios (ORs) for patients being ‘satisfied’, with 95% confidence intervals (CIs).
For multivariable binary logistic regression modelling, variables that had a P-value of less than 0.2 were included in an initial multivariable model, and a backward elimination approach was employed to remove variables sequentially on the basis of Wald’s statistic P-value until all remaining variables had a P≤0.05. Effect estimates were reported as adjusted OR with 95% CI. The two-sided level of statistical significance was set as P≤0.05. All analyses were performed using Stata 15 (StataCorp., 2017., Stata Statistical Software: Release 15; College Station, TX, USA: Statacorp LLC).
Results
A total of 1435 consecutive patients with PNBs that met inclusion criteria were identified. A patient satisfaction score was present for 979 of these patients, yielding a follow-up rate of 68%. The median (interquartile range) time period between PNB and follow-up phone call was 21 (10–47) days. ASA PS I–II and patients receiving sedation were over-represented in the group of patients that were successfully followed up (Table 1). Patients identified as ASA PS I–II represented 67% (963/1435) of total patients, yet made up 70% (685/979) of the followed up patients (P<0.001). Similarly, patients who received sedation during their block represented 65% (932/1423) of total patients yet were over-represented at 70% (686/974) of the followed up patients (P<0.001). All other demographic and clinical characteristics were similar in terms of follow-up status.
Characteristics of patients receiving peripheral nerve block, stratified by follow-up.
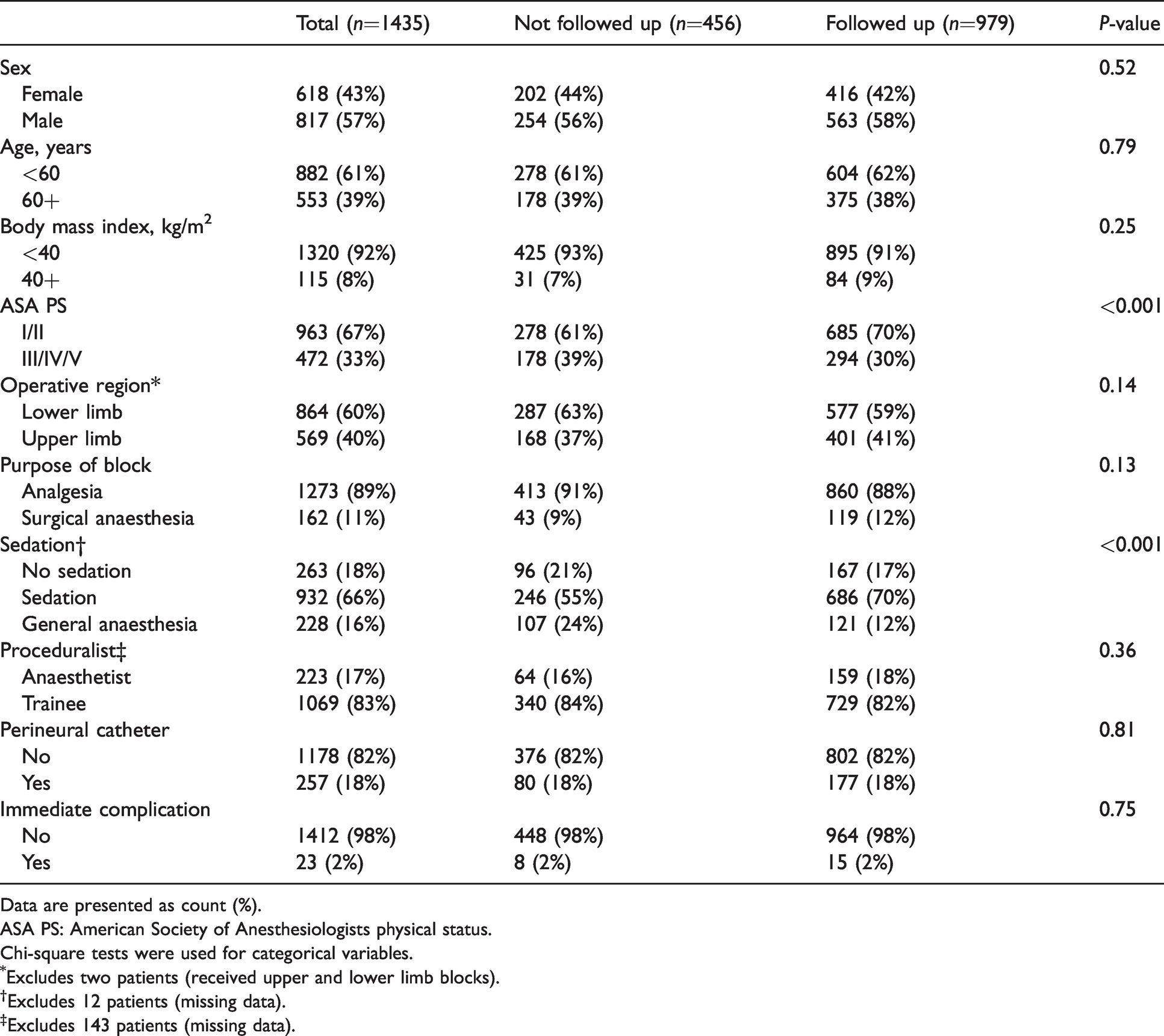
Data are presented as count (%).
ASA PS: American Society of Anesthesiologists physical status.
Chi-square tests were used for categorical variables.
Excludes two patients (received upper and lower limb blocks).
Excludes 12 patients (missing data).
Excludes 143 patients (missing data).
There were 871 patients with a satisfaction score of 4–5 (i.e. ‘satisfied’) from a total of 979 patients. Thus 89% (871/979) of respondents were considered ‘satisfied’ and 108 patients were identified as ‘not satisfied’. In univariable analyses, patient satisfaction was not associated with any patient or block characteristics (Table 2). In contrast, four of the five variables that describe postoperative feedback (pain in the PACU, opioid use in the PACU, procedural discomfort and rebound pain) were negatively associated with patient satisfaction.
Satisfied patients stratified by patient and block characteristics.
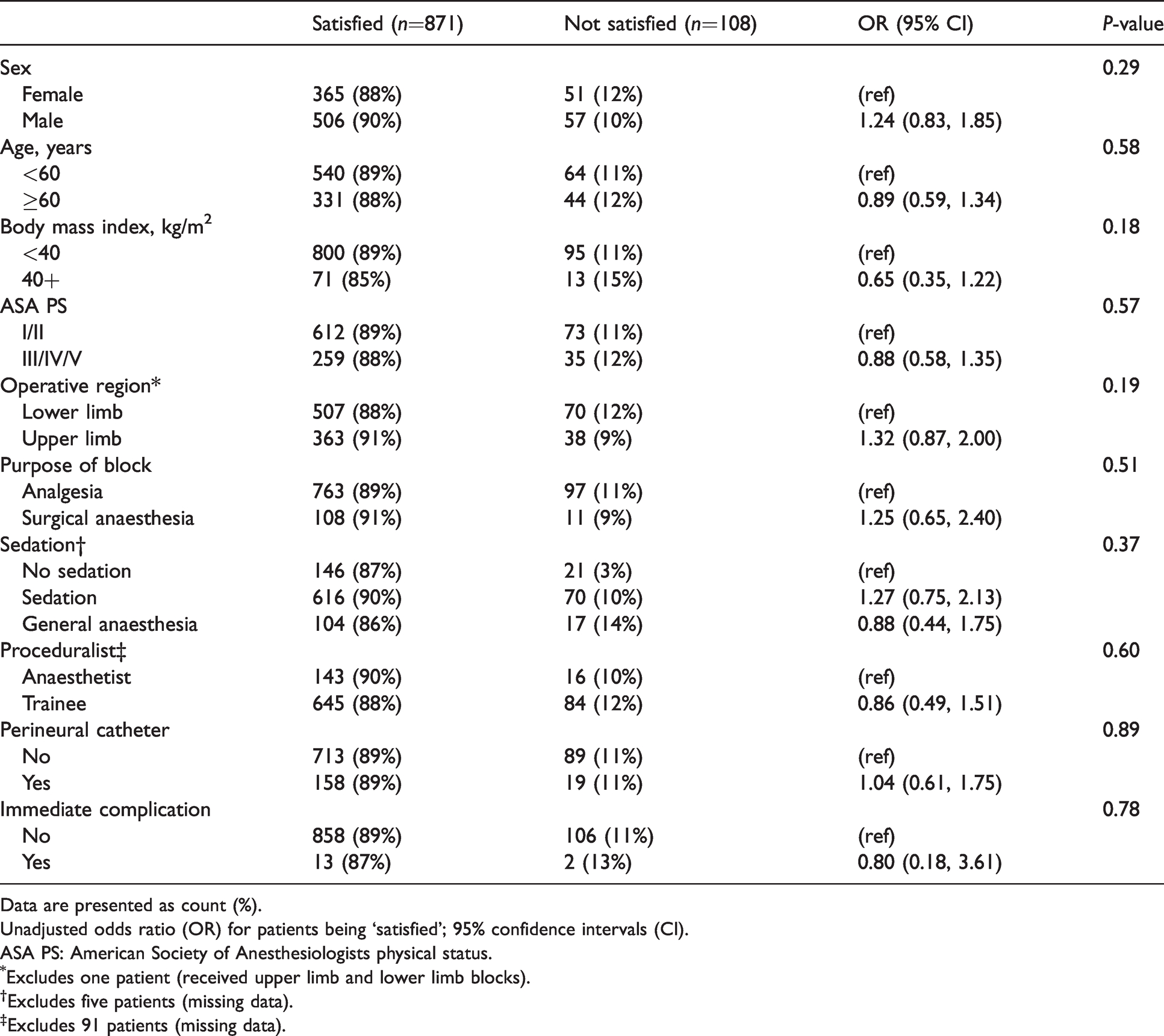
Data are presented as count (%).
Unadjusted odds ratio (OR) for patients being ‘satisfied’; 95% confidence intervals (CI).
ASA PS: American Society of Anesthesiologists physical status.
Excludes one patient (received upper limb and lower limb blocks).
Excludes five patients (missing data).
Excludes 91 patients (missing data).
Multivariable modelling initially included these four statistically significant postoperative feedback variables, as well as body mass index (P=0.18) and operative region (P=0.197). Despite the strong association observed in the univariable model, opioid use was not included in the final multivariable model because it was considered as a mediator (on the causal pathway between pain in the PACU and patient satisfaction), further supported by their being strongly associated. The multivariable modelling therefore identified three variables as being negatively associated with patient satisfaction — rebound pain, procedural discomfort and pain in the PACU (Table 3).
Satisfied patients, stratified according to postoperative feedback.
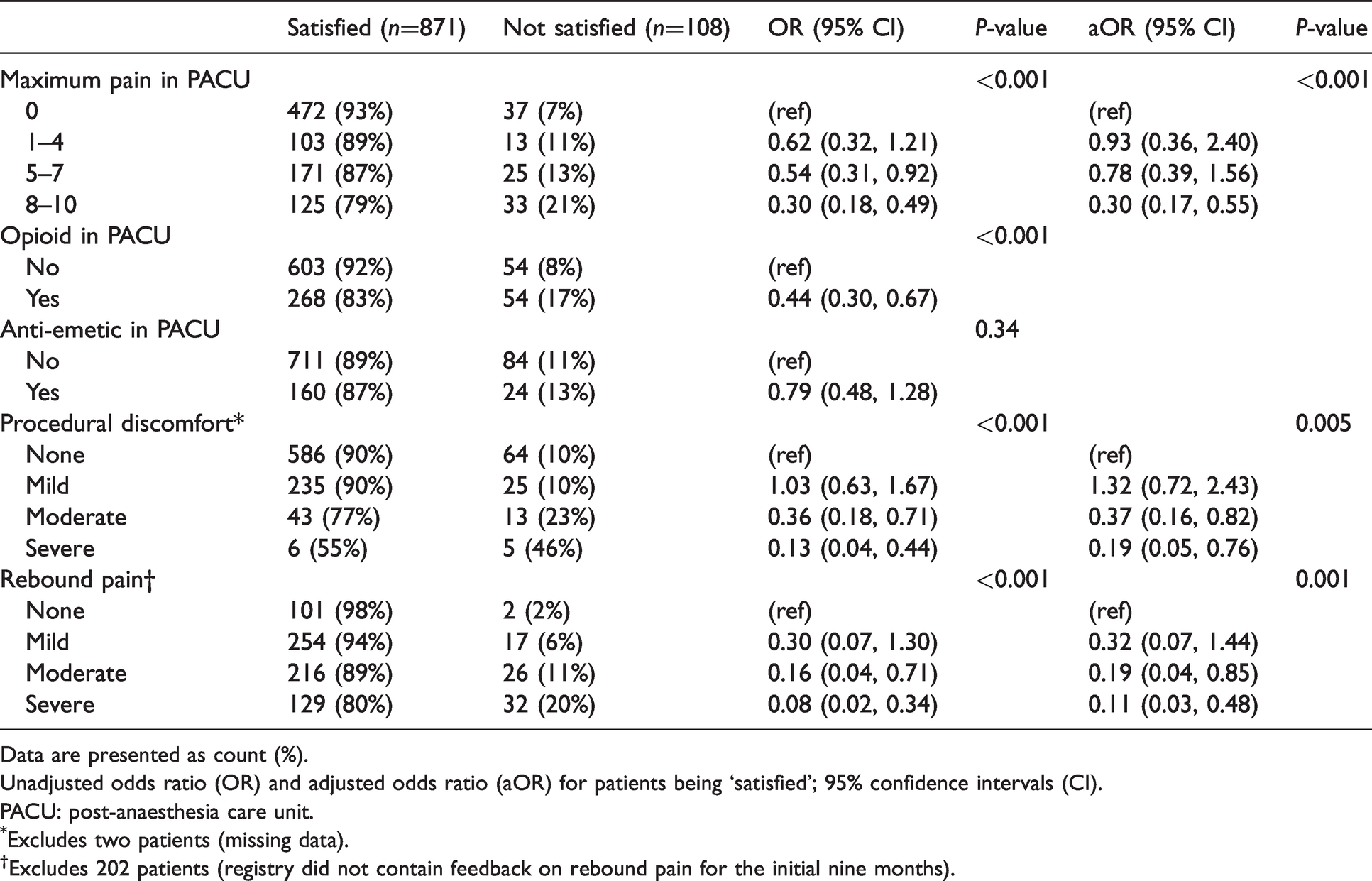
Data are presented as count (%).
Unadjusted odds ratio (OR) and adjusted odds ratio (aOR) for patients being ‘satisfied’; 95% confidence intervals (CI).
PACU: post-anaesthesia care unit.
Excludes two patients (missing data).
Excludes 202 patients (registry did not contain feedback on rebound pain for the initial nine months).
Rebound pain had a strong negative association with patient satisfaction, which was further dependent on intensity. Compared to no rebound pain, patients were less likely to be ‘satisfied’ when they had moderate rebound pain (OR 0.16, 95% CI 0.04 to 0.71 and adjusted OR 0.19, 95% CI 0.04 to 0.85) or severe rebound pain (OR 0.08, 95% CI 0.02 to 0.34 and adjusted OR 0.11, 95% CI 0.03 to 0.48). Discomfort during the PNB procedure also had a strong negative association with patient satisfaction, which was also dependent on intensity. Compared to no procedural discomfort, patients were less likely to be ‘satisfied’ when they had moderate procedural discomfort (OR 0.36, 95% CI 0.18 to 0.71 and adjusted OR 0.37, 95% CI 0.16 to 0.82) or severe procedural discomfort (OR 0.13, 95% CI 0.04 to 0.44 and adjusted OR 0.19, 95% CI 0.05 to 0.76). Patients were also less likely to be ‘satisfied’ if they had an NRS for pain in the PACU of 8/10 or greater (OR 0.30, 95% CI 0.18 to 0.49 and adjusted OR 0.30, 95% CI 0.17 to 0.55) compared to no pain.
Of the factors that were negatively associated with patient satisfaction (Figure 1), rebound pain occurred most frequently, with 21% (161/777) of patients reporting rebound pain as severe and 31% (242/777) reporting rebound pain as moderate. Severe pain in the PACU occurred less frequently, with 16% (158/979) of patients reporting an NRS for pain in the PACU of 8/10 or greater. Discomfort during the PNB procedure was uncommon, with only 1% (11/977) of patients reporting severe procedural discomfort and 6% (56/977) of patients reporting moderate procedural discomfort.
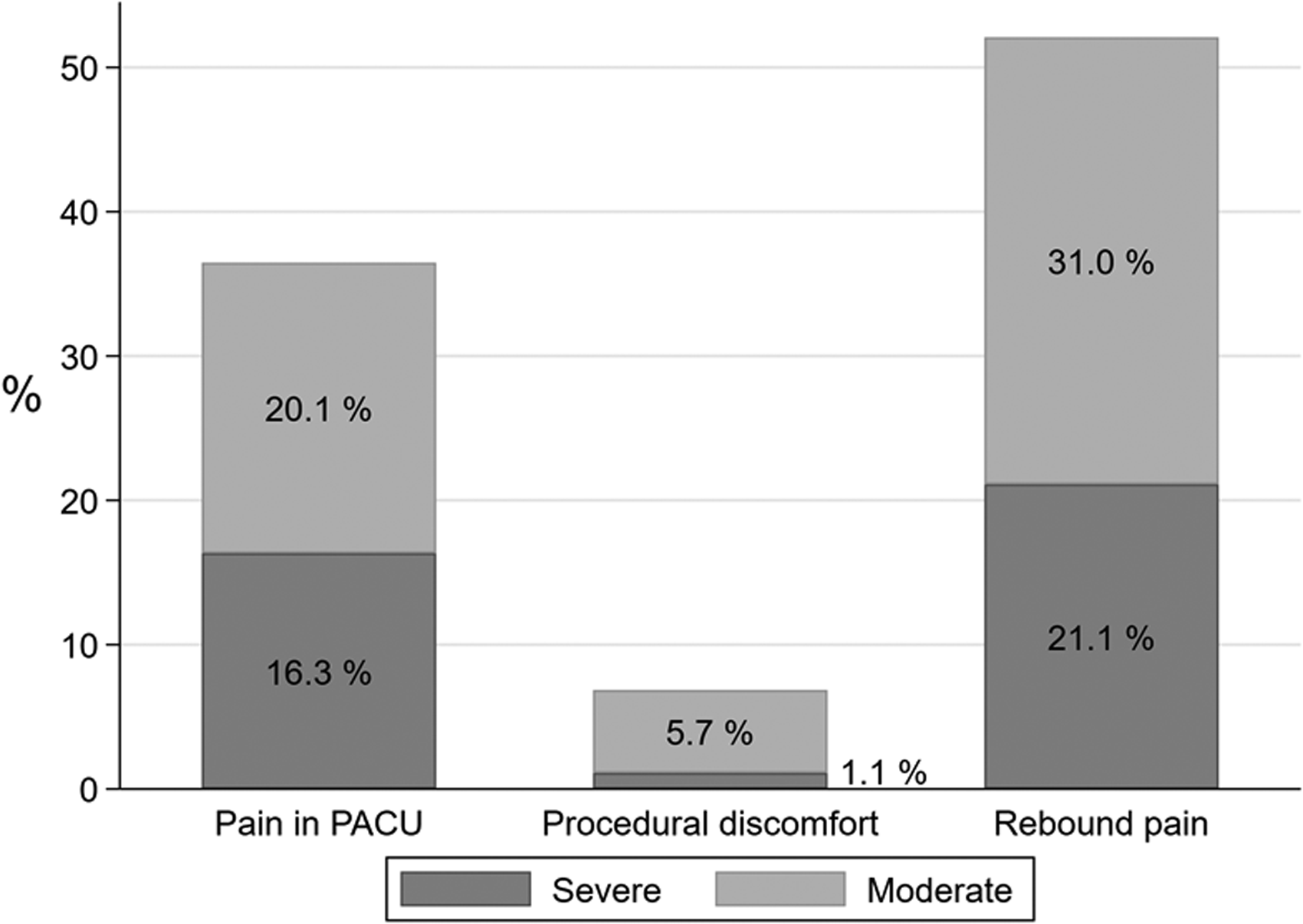
Percentage of patients who experienced pain in the post-anaesthesia care unit (PACU), procedural discomfort, and rebound pain — stratified according to the intensity of pain.
There was a relationship between patient satisfaction and willingness to undergo a repeat PNB for a hypothetical future surgery (Table 4). Unsurprisingly, 98% of ‘satisfied’ patients (850/871) indicated that they would be willing to undergo a hypothetical future PNB. Of the 108 patients who were ‘not satisfied’, 56% (60/108) nevertheless reported a willingness to undergo a hypothetical future PNB; 24% (26/108) said that they would be unwilling and 20% (22/108) did not provide an answer.
Cross-table of patient satisfaction and willingness to undergo a hypothetical future nerve block.
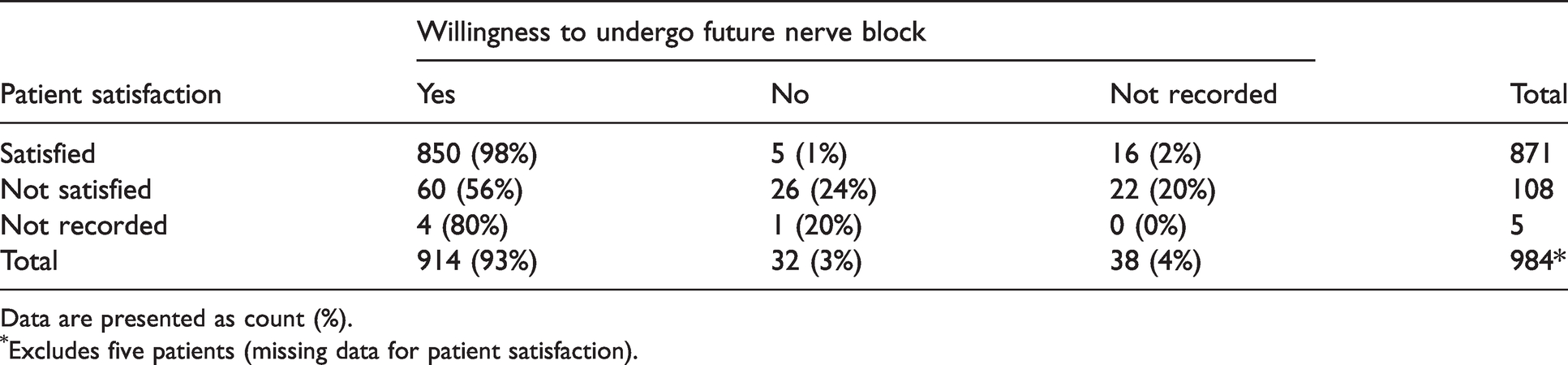
Data are presented as count (%).
Excludes five patients (missing data for patient satisfaction).
Discussion
Our analysis has identified rebound pain, procedural discomfort and severe pain in the PACU as factors that are negatively associated with patient satisfaction following PNB for orthopaedic surgery on the upper or lower extremity. Of the factors identified, severe and moderate rebound pain were the complaints that occurred most frequently.
Rebound pain of at least moderate intensity occurred in just over half of our patients — 403/777 (52%). This phenomenon has been described before. In a multicentre study on patient satisfaction with regional anaesthesia, Ironfield et al. identified that just over half of their 9969 respondents reported moderate or severe rebound pain. 5 This implies that an effective way to improve patient satisfaction with regional anaesthesia might be to enact strategies that reduce the incidence, severity or duration of rebound pain. This differentiates PNBs from central neuraxial blocks, in which the most common reasons for patient dissatisfaction relate to discomfort during needle placement, the high number of needle passes, or specific side-effects such as urinary retention.9,10
The finding that severe pain in the PACU was negatively associated with patient satisfaction was unsurprising. It is known, for example, that labouring women who report high post-epidural pain scores also report lower patient satisfaction. 11 Given that the main benefit of PNBs is to provide superior pain relief in the immediate postoperative period, we expected that the apparent failure to do so would be judged harshly by patients. We did not differentiate between pain due to a failed block versus pain from surgery outside a successfully blocked region of the body because we did not consider this distinction relevant from the point of view of the patient.
Rebound pain has been defined as ‘the quantifiable difference in pain scores when the block is working versus the increase in acute pain that is encountered during the first hours after the effects of PNB resolve’. 12 It occurs ubiquitously across a range of upper limb and lower limb orthopaedic operations whenever PNBs are used. 13 Some patients describe the pain as very intense and lasting for several hours, whereas others describe it as a mildly unpleasant dull ache. 14 There is some evidence to suggest that rebound pain may be less intense in patients over 60 years of age. 15
Perineural catheters have been shown to reduce rebound pain after anterior cruciate ligament reconstruction, 16 ankle fracture surgery 17 and arthroscopic rotator cuff repair. 18 Compared to patients who received a single-shot PNB, our data revealed that patients who received a perineural catheter were no more (or less) likely to be ‘satisfied’. To explore this further, we conducted a post hoc analysis and found no statistically significant difference in the severity of rebound pain between patients with perineural catheters versus patients with single-shot blocks (P=0.46). This is not surprising considering that our patients were not randomly allocated. Patients receiving perineural catheters would likely have unmeasured confounding variables (e.g. more extensive surgery, chronic pain, opioid tolerance) that systematically bias their reporting of pain scores. We therefore caution against drawing any conclusions from our dataset about the relative utility of using perineural catheters to reduce rebound pain.
To the best of our knowledge, this is the first study to demonstrate and quantify the degree to which rebound pain is negatively associated with patient satisfaction following PNB. Ironfield et al. previously demonstrated that rebound pain was negatively associated with a patient’s willingness to undergo repeat PNB only when their pain was severe (OR 0.58, 95% CI 0.40 to 0.85) and not when it was moderate (OR 1.03, 95%CI 0.72 to 1.42). 5 This is interesting, because it implies that patient satisfaction and willingness to undergo repeat PNBs are metrics that are related yet subtly different.
Our finding that over half of the patients who reported being ‘not satisfied’ stated that they would nevertheless be willing to undergo a hypothetical future PNB has been described before. Montenegro et al. surveyed 314 patients following regional anaesthesia for limb surgery; 15 patients reported being only partially satisfied or not satisfied, yet nine out of 15 (60%) nevertheless stated a willingness to undergo a hypothetical future PNB. 4
Our high rate of non-responders (20%) for the question on willingness to undergo repeat PNB is notable, considering that the question on patient satisfaction was only left unanswered by five out of 984 (0.5%) respondents. We speculate that the 5-point scale of patient satisfaction may have led to a higher response rate because it allowed for patients to remain neutral by giving a satisfaction score of 3 out of 5. Alternatively, patients may have wanted to answer ‘no’ to their willingness to undergo repeat PNB but felt uncomfortable giving this negative feedback (social desirability bias). When incomplete responses were excluded, our rate of willingness to undergo a hypothetical future PNB was 914/946 (97%), which was comparable to the rate (94.6%) found by Ironfield et al. 5
Another problem with measuring willingness to repeat PNB is that patients may state one preference when it is a hypothetical situation only to change their mind when the hypothetical becomes a reality. This phenomenon is known to economists as ‘revealed preference’ as opposed to ‘stated preference’. 19 Because of the low response rate, and the potential for stated preference to differ from revealed preference, we suggest that patient satisfaction is a better metric than willingness to undergo a hypothetical future PNB if one wishes to assess patient-centred subjective interpretation of the quality of regional anaesthesia.
In a study of 21,338 patients receiving PNBs, Kubulus et al. reported higher levels of patient satisfaction when the blocks were performed under sedation (compared to no sedation). 20 We were unable to replicate this finding, which may be a function of our smaller sample size. Alternatively, it may be that sedation is a surrogate marker for something else — an anaesthetist who prioritises patient comfort during block placement (which our analysis revealed as a factor associated with patient satisfaction).
Ironfield et al. reported a number of factors such as increasing age (OR 1.14 per 10-year increase), male sex (OR 1.60) and immediate complication (OR 0.37 for ‘arterial puncture’, OR 0.35 for ‘other complication’) that were associated with a willingness to undergo a hypothetical future PNB. 5 We did not find statistically significant associations of these factors with patient satisfaction in our patient sample. It is unclear whether these different findings are due to our smaller sample size, or due to our study using patient satisfaction rather than willingness to repeat PNB as the primary outcome.
Our study is limited by the exclusion of long-term complications such as block-related nerve injury, which clearly has the potential to impact patient satisfaction negatively. Large observational studies have estimated the prevalence of block-related nerve injury to be between 0.2 and 0.9 per 1000 blocks,21–23 so a larger study would be required to examine any association. Our slightly higher follow-up rate for ASA PS I–II patients and patients receiving sedation is also a potential source for bias.
Collecting feedback by phone interview may have resulted in less reporting of negative feedback as patients may have feared negative repercussions, or simply wished to avoid a potentially awkward conversation. Another source of bias is that our follow-up ascertained the patient’s memory of pain several weeks after the PNB, and indeed there was wide variability in the time to follow-up. It is possible that asking patients about their procedural discomfort and/or rebound pain while they were experiencing the pain or at a standardised point in time soon after their procedure would yield more accurate results. On the other hand, the fact that so many patients remembered rebound pain as being moderately or severely painful so long after their surgery is further evidence that rebound pain creates a significant and lasting negative impression.
In theory, retrospective observational research (such as ours) has a greater potential for bias compared to if the same research had been conducted prospectively. However, given that all data were collected prospectively and contemporaneously, and given that the study was designed before any statistical analysis, we do not consider the retrospective nature of our research to be a major limitation. Finally, our findings also cannot determine the direction of causality; it may be that pain/discomfort causes patients not to be satisfied, or it may be that patients who are not satisfied report higher levels of pain/discomfort when given the opportunity to provide feedback.
Conclusion
Rebound pain of at least moderate intensity, procedural discomfort of at least moderate intensity and severe pain in the PACU are all factors associated with low levels of patient satisfaction following PNB. Of these three factors, rebound pain occurs most frequently. These data suggest that if one wishes to increase patient satisfaction with PNB, a reasonable strategy might be to focus primarily on interventions that limit either the incidence, the severity or the duration of rebound pain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.