
Abstract
There is no consensus on which weight clinicians should use for weight-based dosing of neuromuscular blocking agents (NMBAs), as exemplified by differing or absent recommendations in clinical practice guidelines. The purpose of this paper is to review studies that evaluated various size descriptors for weight-based dosing of succinylcholine and non-depolarising NMBAs, and to provide recommendations for the descriptors of choice for the weight-based dosing of these agents in patients with obesity. All of the studies conducted to date involving depolarising and non-depolarising NMBAs in patients with obesity have assessed single doses or short-term infusions conducted in perioperative settings. Recognising that any final dosing regimen must take into account patient-specific considerations, the available evidence suggests that actual body weight is the size descriptor of choice for weight-based dosing of succinylcholine and that ideal body weight, or an adjusted (or lean) body weight, is the size descriptor of choice for weight-based dosing of non-depolarising NMBAs.
Keywords
Introduction
There is no consensus on which weight clinicians should use for weight-based dosing of neuromuscular blocking agents (NMBAs), as exemplified by differing or absent recommendations in clinical practice guidelines. Current guidelines by the Society of Critical Care Medicine suggest (i.e. weak recommendation) that clinicians use a consistent weight (ideal body weight (IBW) or adjusted body weight), not actual body weight, when calculating doses of non-depolarising NMBAs for obese patients. 1 For perioperative management of obese surgical patients, guidelines of the Association of Anaesthetists of Great Britain and Ireland and the Society for Obesity and Bariatric Anaesthesia suggest the use of lean body weight for dosing non-depolarising NMBAs. 2 Guidelines by the Enhanced Recovery After Surgery (ERAS) Society for the perioperative care of patients undergoing bariatric surgery provide no specific recommendations for dosing NMBAs. 3 None of these clinical practice guidelines provide dosing recommendations for succinylcholine. In the critical care and anaesthesia settings, the choice of weight for weight-based dosing of NMBAs is of most importance during intubating procedures and with short-term infusions when concerns related to under- or overdosing are most likely to be an issue. When used as sustained infusions in the critical care setting, use of a consistent weight descriptor is likely more important than the choice of weight descriptor, assuming dosing adjustments are performed using appropriate clinical assessment and neuromuscular transmission monitoring. The purpose of this paper is to review studies that evaluated various size descriptors for weight-based dosing of succinylcholine and non-depolarising NMBAs, and to provide recommendations for the descriptors of choice for the weight-based dosing of these agents in patients with obesity. Particular emphasis will be placed on studies evaluating these agents in patients with more extreme obesity (body mass index (BMI) ≥40 kg/m2 as defined by the Centers for Disease Control and Prevention), since these patients are most likely to have adverse consequences associated with suboptimal dosing regimens. For example, when using a 1 mg/kg intravenous dose of rocuronium for rapid sequence induction, an extremely obese patient with an IBW of 70 kg and an actual body weight of 160 kg could receive a dose ranging from 70 mg with potential inadequate paralysis and suboptimal intubating conditions if using IBW to 160 mg with potential prolonged paralysis if using actual body weight. In conjunction with patient-specific considerations, the recommendations in this paper provide initial guidance for designing NMBA dosing regimens. As there is no standardisation of size descriptor terminology, Table 1 provides a list of the definitions of the size descriptors used in this paper. Since the equations or nomograms used to estimate IBW, lean body weight, lean body mass and adjusted body weight vary from study to study, the specific method of estimation is described when discussing specific studies or making weight-based dosing recommendations.
Definitions of size descriptors.
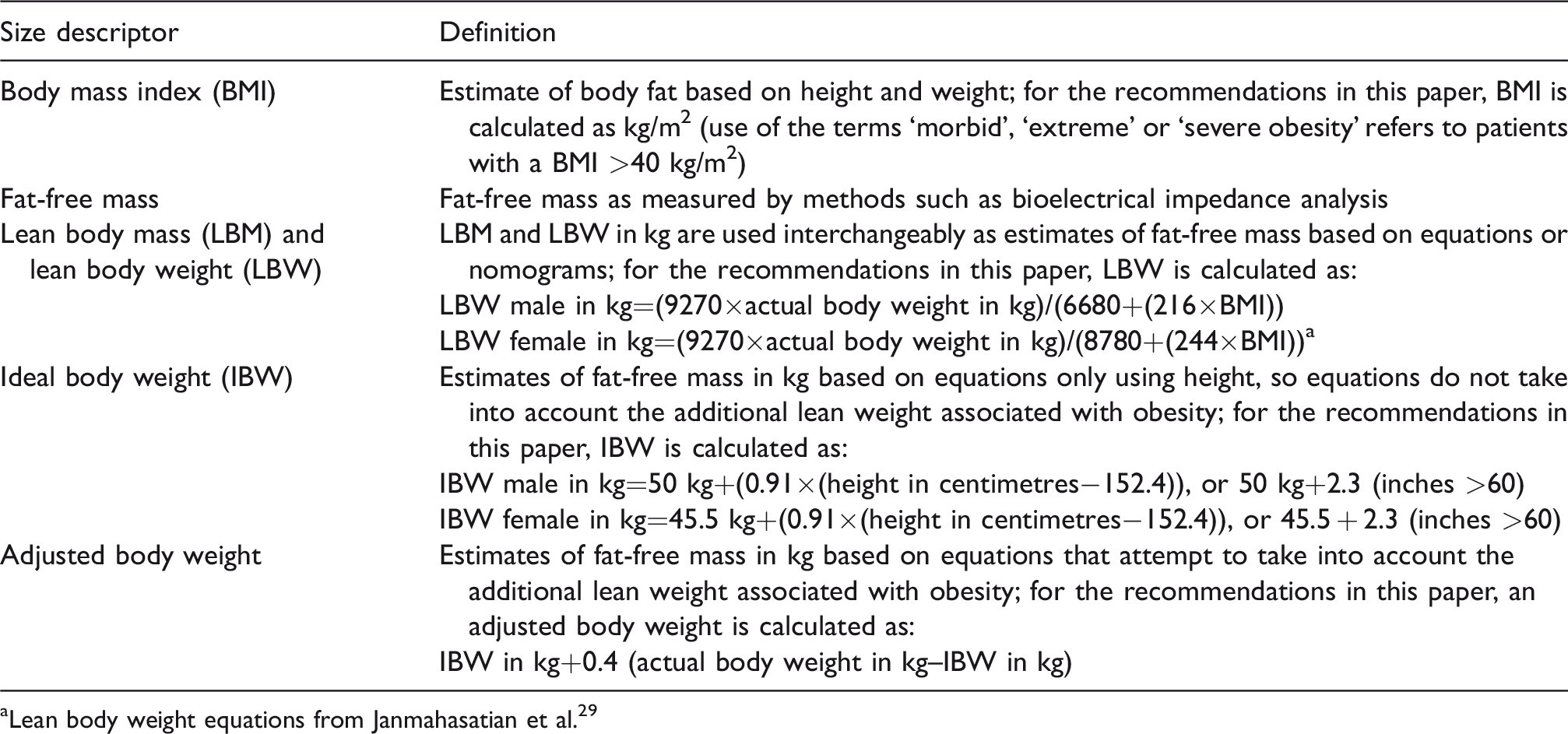
aLean body weight equations from Janmahasatian et al. 29
Data sources
The search strategy was developed using the MeSH database of PubMed. The initial search was for ‘neuromuscular blocking agents’. The search was limited to ‘humans’, ‘English’ and ‘adults’ from July 1976 to present. This provided 5172 results, 1735 results when limited by article type to clinical trial and 31 results when limited to obesity. Eleven of the trials included in this review were identified from this initial search, with the remaining trials identified through the following searches. The heading ‘neuromuscular blocking agents’ was added to the PubMed search builder, with subsequent searches for ‘succinylcholine’, ‘pancuronium’, ‘vecuronium’, ‘atracurium’, ‘cisatracurium’ and ‘rocuronium’ using the ‘OR’ function. From the latter search, the following numbers of abstracts were reviewed for each NMBA: succinylcholine 541, pancuronium 338, vecuronium 813, atracurium 531, cisatracurium 193 and rocuronium 686. One additional study was identified from these abstracts. Bibliographies of papers were reviewed for articles that may have been missed through the PubMed search, and ten additional studies were identified.
Historical perspective
In an investigation published in 1972, Wulfsohn evaluated lean body mass as a preferred alternative to actual weight for dosing succinylcholine based on the premise that initial drug distribution into highly perfused lean tissues (i.e. non-fat tissues) was the primary determinant of succinylcholine onset. 4 Percent fat was estimated (90 – 2(height in inches–girth in inches)), which was subsequently used to estimate lean body mass ((100–percent fat)×(weight in kg)). Succinylcholine doses of 0.6 mg/kg (seven patients), 0.8 mg/kg (21 patients) and 1 mg/kg (38 patients), all based on lean body mass, were administered, with muscle twitch response used to determine degree of blockade and recovery. The 0.8 mg/kg and 1 mg/kg doses resulted in complete block and adequate intubating conditions, whereas the 0.6 mg/kg dose yielded an average block of 96.7% and suboptimal intubating conditions (not performed or performed with difficulty in 43% of patients). Recovery time was longer with larger doses (8.9 minutes with 0.6 mg/kg, 9.2 minutes with 0.8 mg/kg and 9.6 minutes with 1 mg/kg), but the differences were small (statistical significance not stated). Heavier patients (76.9 kg versus 51 kg) had shorter recovery times (7.7 minutes versus 10.1 minutes, respectively). Wulfsohn recommended the use of lean body mass for dosing, stating that even reduced doses based on actual body weight could lead to prolonged apnoea, although data from the study found a poor correlation between apnoea and lean body mass or actual body weight. Conclusions from the Wulfsohn study about weight-based dosing of succinylcholine in obese patients are limited due to the low weight of the patients under investigation and other methodological limitations, but the study set the stage for future investigations of the preferred size descriptor to use for dosing various NMBAs.
All of the subsequent clinical trials investigating dosing of NMBAs in extremely obese patients have been intravenous bolus-dose or short-infusion studies conducted in association with surgical procedures (Supplemental Table S1).5–22 In these bolus-dose studies, the therapeutic concentration of the NMBAs is largely a function of volume of distribution, which is small for NMBAs, given their hydrophilic nature. Estimation of pharmacokinetic parameters necessitates assumptions about factors such as homogeneity in drug distribution and consistency in clearance when using compartmental modelling. While fraught with difficulty, dosing extrapolations from these bolus-dose studies to critically ill patients receiving sustained infusions of such agents is necessary for clinicians to formulate initial dosing regimens.
Succinylcholine (suxamethonium)
None of the clinical trials have evaluated succinylcholine for rapid sequence induction of obese or extremely obese patients in the emergency department or intensive care unit setting. Three trials evaluated succinylcholine in obese or extremely obese patients undergoing surgery, and the conclusions from all three were to dose succinylcholine using actual body weight.6,13,17 One open-label trial which evaluated succinylcholine in non-obese, overweight and obese adults found a linear correlation between serum pseudocholinesterase activity and three size descriptors (actual weight, body surface area and body mass index). 6 The investigators recommended the use of actual body weight for dosing, since recovery times using weight-based dosing were similar regardless of weight. 6 Another open-label trial in obese adolescents found dosing by either actual body weight or body surface area to yield similar results. 13 In addition, effective doses based on train-of-four monitoring were similar to those noted in a previous study involving lean adolescents. Therefore, the investigators recommended the use of actual body weight using a weight-based dosing regimen. The third trial involving succinylcholine was a double blind investigation that randomised extremely obese patients into three groups based on IBW (calculated as 22 x (height in metres, squared)), adjusted (referred to as lean body weight and calculated as ideal+30% of excess weight) weight or actual body weight. 17 Patients dosed using IBW had significantly less maximal block, and one-third of them had intubating conditions judged to be poor. Patients dosed using adjusted body weight had similar maximal block and significantly shorter recovery time compared with those dosed using actual body weight, but intubating conditions using adjusted weight were judged to be poor in 4/15 patients compared with 0/15 patients in the actual weight group (P<0.05). The investigators recommended the use of actual body weight for weight-based dosing of succinylcholine, recognising that neither adjusted nor actual weight yielded both excellent intubating conditions and short recovery.
Non-depolarising neuromuscular blocking agents
In a study involving pancuronium, extremely obese patients undergoing gastric bypass were administered a bolus dose followed by a continuous infusion to maintain 90% twitch depression. 5 In two uncontrolled studies involving rocuronium and atracurium, patients undergoing major surgery were administered bolus doses followed by continuous infusions during the surgical procedure.14,23 One of these studies was not focused on obesity per se, but rather atracurium clearance in patients with various body builds. 23 Compared to actual body weight, lean body weight (as estimated by James equations 24 ) was a significantly (P<0.001) better predictor of atracurium clearance in both underweight and obese patients. In all subsequent studies involving vecuronium, atracurium, cisatracurium or rocuronium, the obese or extremely obese patients under investigation were given intravenous weight-based bolus doses during neurosurgical, gynaecological or bariatric surgical procedures.7–12,15,16,18–22 In two small studies involving vecuronium for patients undergoing neurological procedures, recovery times were shorter in normal-weight controls compared with obese (few if any extremely obese) patients, with both groups dosed based on IBW.7,9 In two small studies involving atracurium, there were no significant differences in recovery times between the normal-weight controls and obese patients, with both groups dosed on IBW.7,8 In a study involving 127 female patients of varying weights receiving atracurium based on actual body weight, both actual body weight and actual weight divided by body surface area were significant predictors of the prolonged duration of action noted in the obese patients. 11 The investigators recommended a reduced dose of atracurium for patients with an actual body weight >70 kg. In a more recent randomised trial involving patients with a BMI >35 kg/m2 undergoing bariatric surgery, patients dosed by IBW had more rapid (P≤0.05) and less variable (significance not provided) recovery compared with patients dosed by actual body weight. 20 In addition, blockade reversal with neostigmine was necessary in 70% of patients dosed by actual weight compared with none dosed by IBW (P=0.003).
Of the trials involving bolus-dose rocuronium, one small study found no difference in recovery time between six patients who were overweight or mildly obese and six patients of normal weight, all of whom were dosed using actual body weight. 12 Another study evaluated a 1.2 mg/kg dose of rocuronium based on IBW (22 x (height in metres, squared)) in patients with a BMI >40 kg/m2 found good to excellent intubating conditions in a high percentage of patients. 21 Two studies found the duration of action of rocuronium was longer in patients with increasing BMIs and when dosed using actual body weight.10,15 There is one double blind investigation that evaluated patients with BMIs ranging from 34 to 72 kg/m2. 19 Patients were randomised to receive 0.6 mg/kg of rocuronium by IBW (height in cm minus 106 for women; height in cm minus 102 for men), IBW plus 20% of excess weight or IBW plus 40% of excess weight. While there were no significant differences in onset time, the duration of action increased with increased doses, with a statistically significant difference noted between the IBW and IBW plus 40% of excess weight. Intubating conditions were similar in all patients. So, the investigators recommended using IBW for dosing rocuronium. The most recent trial evaluating rocuronium in a double blind investigation involved 40 women undergoing laparoscopic surgery. 22 Patients were randomised to receive 1.2 mg/kg doses of rocuronium based on an adjusted or lean body weight. Although intubating conditions and onset of blockade were similar between groups, the duration of action in the adjusted body weight group was almost twice that of the lean body weight group (60 versus 35 minutes, respectively; P < 0.01).
Two small open-label trials, each with a control group of normal-weight patients, evaluated cisatracurium dosing in patients with morbid obesity. In the first trial, the duration of action of cisatracurium was significantly longer in obese patients who received 0.2 mg/kg based on actual body weight compared with obese patients who received 0.2 mg/kg based on IBW or normal-weight patients who received 0.2 mg/kg based on actual weight. 16 In the second trial, the duration of action of cisatracurium was significantly shorter in extremely obese patients who received 0.15 mg/kg based on an adjusted body weight compared with the same dose given based on IBW (height in cm–100 for men or height in cm–105 for women) in normal-weight patients. However, the clinical significance of the difference in duration is questionable (46 versus 56 minutes, respectively). Intubating conditions were significantly worse in the obese patients. 18
Limited evidence suggests that IBW, or possibly adjusted body weight, is preferred when using weight-based dosing of rocuronium for rapid sequence induction in extremely obese patients.10,12,14,15,19,21,22 However, the most appropriate dose is unknown, since no adequately powered clinical trial has compared commonly used doses (i.e. 0.6 mg/kg and 1.2 mg/kg) adjusted by the same dosing weight for onset of action, optimal intubating conditions and duration of action.
None of the clinical trials evaluated size descriptors and doses of non-depolarising NMBAs given as sustained infusions in obese compared with normal-weight patients. Extrapolations from single-dose studies in the surgery setting are fraught with difficulties, given the frequent changes in organ function over time in critically ill patients. Further complicating the issue of dosing patients receiving sustained infusions of non-depolarising NMBAs is the use of high-dose regimens in patients with acute respiratory distress syndrome (ARDS) which, if adopted, arguably would preclude the need for weight-based dosing regimens regardless of obesity. In three investigations involving patients with ARDS, patients in the treatment arms received 48-hour infusions of cisatracurium at doses of sufficient magnitude (i.e. 37.5 mg/h) to obviate the need for train-of-four guided dosing.25,26 Some investigators are now recommending this dosing approach when using cisatracurium as rescue therapy for ARDS. 27 However, we agree with other investigators who argue that the flat-dose regimen was designed to facilitate blinding but, if used clinically, could lead to adverse effects from needlessly excessive dosing and would be costly. 28 This flat-dose approach to dosing raises additional questions in subgroups of patients such as those of extreme body weight who were not well represented in the published studies. Concerns related to non-depolarising NMBAs accumulation in light of single-dose studies conducted to date suggest that an IBW or an adjusted body weight is preferred for weight-based dosing of obese patients in conjunction with clinical and train-of-four monitoring. As an alternative, lean body weight, as calculated by more validated lean body weight equations, could be used, with the recognition that such calculations might be prone to dosing errors if performed using handheld calculators instead of being built into software such as the electronic health record. 29
Discussion
While all of the studies evaluating succinylcholine in extremely obese patients were conducted in the surgery setting, there is little reason to predict that the results would not apply to other settings where intubations are performed. There is a linear correlation between pseudocholinesterase activity and actual body weight. So, underdosing of succinylcholine is the major concern, assuming no abnormal genetic variations in metabolism. An argument could be made to use a larger dose with IBW instead of using usual recommended doses with adjusted or actual body weights, but we do not recommend this approach, since it has not been studied and so there is no information as to how much larger the dose should be depending on the degree of obesity.
For succinylcholine, actual body weight with usual weight-based doses in milligrams per kilogram is suggested for weight-based dosing in obese or extremely obese patients. The use of an adjusted or lean body weight may be considered for patients in the upper end of the extremely obese category (e.g. BMI >60 kg/m2) and/or for situations in which the bedside supply of succinylcholine is limited (e.g. standard doses in rapid sequence induction kits), recognising that intubating conditions may be less than optimal.
There are few single-dose studies of non-depolarising NMBA agents in the surgical setting evaluating the most appropriate size descriptor for weight-based dosing in patients of extreme weight, but the studies that are available demonstrate less consistent and more prolonged recovery when using actual body weight for dosing, which in one study necessitated the use of pharmacological reversal in 70% of patients compared with none dosed by IBW. 20 A caveat to all of the studies is that sample sizes were small and lack of follow-up precluded the detection of possible clinically important adverse events such as pulmonary complications or need for reintubation due to prolonged duration of action of NMBAs resulting from excessive dosing. There are no studies evaluating the most appropriate size descriptor for dosing obese patients receiving sustained infusions of non-depolarising NMBAs. Nevertheless, there is substantial consensus from study investigators that when using weight-based dosing regimens, an IBW, adjusted body weight or lean body weight are the size descriptors of choice for obese patients, with the final dosing determination based on patient-specific considerations such as body composition (fat versus muscle weight), comorbidities, cost, the specific NMBA prescribed and concomitant medications (e.g. sedatives, analgesics, reversal agents).
Use of IBW might lead to suboptimal blockade with initial dosing, while use of actual body weight might lead to prolonged duration of action after single intubating doses or after discontinuation of short-term infusions. In addition to cost considerations, prolonged duration of action of NMBAs could lead to adverse sequelae such as pulmonary complications and the need for reintubation. NMBA reversal agents such as neostigmine and sugammadex (for rocuronium or vecuronium) are available for use in patients undergoing surgery, but each has associated costs and potential adverse effects to consider. In contrast to IBW equations based solely on height, adjusted and lean body weight equations take into account the increases in NMBA volume of distribution and clearance likely to occur in patients with obesity, but may avoid excessive dosing due to less than proportional increases in these pharmacokinetic parameters relative to the total increased body weight in obesity. For non-depolarising NMBAs, the available evidence and consensus of investigators is that IBW, adjusted body weight or lean body weight are the most appropriate size descriptors for use with weight-based dosing regimens in obese patients, and particularly in patients with more severe forms of obesity (e.g. BMI ≥40 kg/m2). In general, IBW is most useful when overdosing is more of a concern than underdosing, while use of adjusted or lean body weight is preferable when avoidance of underdosing is the priority.
Conclusion
All of the studies identified in this review involving depolarising and non-depolarising NMBAs in patients with obesity have assessed single-dose or short-term infusions conducted in perioperative settings. There is no choice but to extrapolate this information to dosing obese patients in other settings and with other regimens, in particular continuous infusions. Recognising that any final dosing regimen must take into account patient-specific considerations, the available evidence suggests that actual body weight appears to be the size descriptor of choice for weight-based dosing of succinylcholine in obese patients. For non-depolarising NMBAs, the available evidence suggests that IBW, adjusted body weight or lean body weight are the most appropriate size descriptors for use with weight-based dosing regimens in obese patients, and particularly in patients with more severe forms of obesity (e.g. BMI ≥40 kg/m2). In general, IBW appears to be most useful when overdosing is more of a concern than underdosing, while use of adjusted or lean body weight appears to be preferable when avoidance of underdosing is the priority.
Supplemental Material
sj-pdf-1-aic-10.1177_0310057X20968573 - Supplemental material for Dosing of neuromuscular blocking agents in patients with obesity: A narrative review
Supplemental material, sj-pdf-1-aic-10.1177_0310057X20968573 for Dosing of neuromuscular blocking agents in patients with obesity: A narrative review by Brian L Erstad Jeffrey F Barletta in Anaesthesia and Intensive Care
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.F.B. is a consultant for Wolters Kluwer. There are no other conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.