
Abstract
The primary aim of this study was to evaluate the perceptions of Australian anaesthetists in relation to smartphone use within anaesthetic practice. In particular, we aimed to assess the frequency of smartphone use, the types and number of smartphone applications used, how reliant anaesthetists perceive themselves to be on smartphones and whether they perceive them to be a factor that aids or distracts from their practice. Secondly, we assessed whether there is an association between the type, frequency, reliance and perceptions of smartphone use and the years of experience as an anaesthetist. A 24-item questionnaire addressing these questions was created and distributed to an email list of credentialled anaesthetists in Melbourne, Australia. A total of 113 consultant anaesthetists who practise at 55 hospitals in Melbourne completed the questionnaire. Our results suggest that the majority of anaesthetists are using smartphones regularly in their practice. About 74% of respondents agreed that they rely on their smartphone for their work. We found that respondents were more likely to rely on smartphones and consider them to aid patient safety than to consider them a distraction. This phenomenon was particularly apparent in those who had been a consultant anaesthetist for less than three years. Furthermore, those who had been a consultant anaesthetist for less than three years were more likely to have more smartphone apps relating to anaesthetics, use them more often and rely on them to a greater degree. Our results highlight the ubiquitous and perceived useful nature of smartphones in anaesthetic practice.
Introduction
Smartphones are integral to our personal and professional lives and their use has become ubiquitous in recent years. These devices are now owned by 91% of Australians and enable instantaneous information gathering. 1 Smartphone advancements have improved efficiency within the medical workplace through improved communication among colleagues, access to up-to-date literature and remote monitoring. 2 , 3
There are hundreds of available smartphone applications designed for different medical specialties, including anaesthetics. These applications aid decision-making, improve perioperative planning and provide access to anaesthetic guidelines and algorithms. 4 Smartphones have the clear potential significantly to benefit the work of anaesthetists. However, the potential for distraction caused by smartphones exists. This phenomenon termed ‘distracted doctoring’ is especially pertinent to anaesthetics, in which a lack of situational awareness has the potential to result in catastrophic outcomes for patients. 5
Variations in the level of potential distraction relating to years of experience have been proposed, with trainee anaesthetists being more at risk of distraction, as a result of less experience and a narrower margin for cognitive overload. 6 One might suggest that less experienced anaesthetists should avoid the use of smartphones in theatre to reduce their risk of distractions and errors. However, the release of the iPhone in 2007 accelerated the uptake of smartphones globally and now young professionals enter the workforce having grown up with these devices. To these individuals, smartphones appear as a quintessential component to their learning and development, which may mean they rely more strongly on these devices for their work.
Although some research has explored the pattern of utilisation of and dependence on smartphones by anaesthetists, there are currently limited data on the perceptions of anaesthetists themselves with regard to their smartphone use, and the relationship between their benefit and distractibility in a clinical context. Furthermore, research is limited on whether these perceptions are dependent on the years of experience of an anaesthetist, with differences in smartphone use associated with experience potentially impacting current and future training curricula.
We aimed to evaluate and characterise the use of smartphones in clinical situations by Australian anaesthetists. We also wished to explore their perception of whether their smartphone was a facilitator of, or barrier to, their clinical practice. We hope this information can potentially inform the development of future policies and guidelines surrounding smartphone use in anaesthesia practice.
Methods
In December 2019, a 24-item questionnaire was created on cloud-based software Qualtrics (Provo, UT, USA) and distributed to an email list of currently credentialled anaesthetists at a large tertiary private metropolitan hospital in Melbourne, Australia. This survey was approved in November 2019 by the Human Research Ethics Committee of Cabrini Hospital (CHREC 12-09-12-19), Melbourne, Australia. Only consultant anaesthetists were invited to participate. It was distributed to the email addresses of 317 consultant anaesthetists in Melbourne. Consent was implied by participation in the survey with no incentive offered for completion. Not all email addresses were thought to be actively used.
During questionnaire development, the researchers reviewed the available literature on smartphone use among medical professionals to aid the design of the study. The questionnaire was divided into three sections: responder demographics; smartphone uses; and perceptions of smartphone use within anaesthetic practice.
All the questions in the questionnaire were multiple choice except the final question, which enabled participants to submit a comment regarding the survey.
The study data were collected anonymously and were analysed utilising Qualtrics software. Additional analysis was performed using grouped analysis, whereby agree was grouped as either ‘somewhat agree’ or ‘strongly agree’, and disagree was grouped as either ‘somewhat disagree’ or ‘strongly disagree’.
Results
The questionnaire was completed by 113 participants (response rate 35.6%). Of the 113 anaesthetists who began completing the survey, 110 (97.3%) answered all the questions. Responder demographics are tabulated below in Table 1.
Demographics.
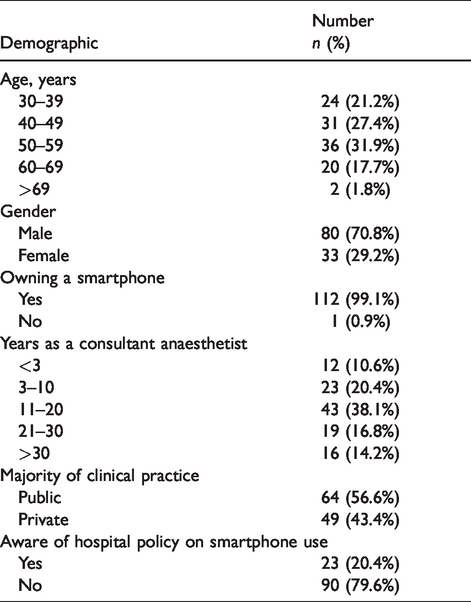
The responders reported regular practice at a total of 55 hospitals in Melbourne (21 public and 34 private). All but one of the respondents reported owning a smartphone, with 91.1% (n = 102) using an iPhone compared to 8.9% (n = 10) using an Android operated device.
Usage
All respondents (100%) reported using their smartphone for anaesthetic practice to varying degrees. Of these, 35.7% (n = 40) reported using their smartphone ‘sometimes’, 13.4% (n = 15) answered ‘about half the time’, 24.1% (n = 27) answered ‘most of the time’ and 26.8% (n = 30) answered ‘always’. Furthermore, 62.5% (n = 70) of survey respondents stated that they used their smartphone on more than six occasions during their last full day of practice.
Most participants (89.2%, n = 74) reported no difference in their smartphone use between public and private practice.
Type of use
The majority (97.3%; n = 109) of participants reported using smartphone applications relating to their practice, with 39.3% (n = 40) possessing more than six different work-related applications on their device.
The number of applications used in clinical practice was shown to vary across the length of anaesthetic practice. As demonstrated in Figure 1, 58% (n = 7) of those practising for less than three years owned at least six separate applications compared to 12.5% (n = 2) of those who had been fully qualified for more than 30 years.
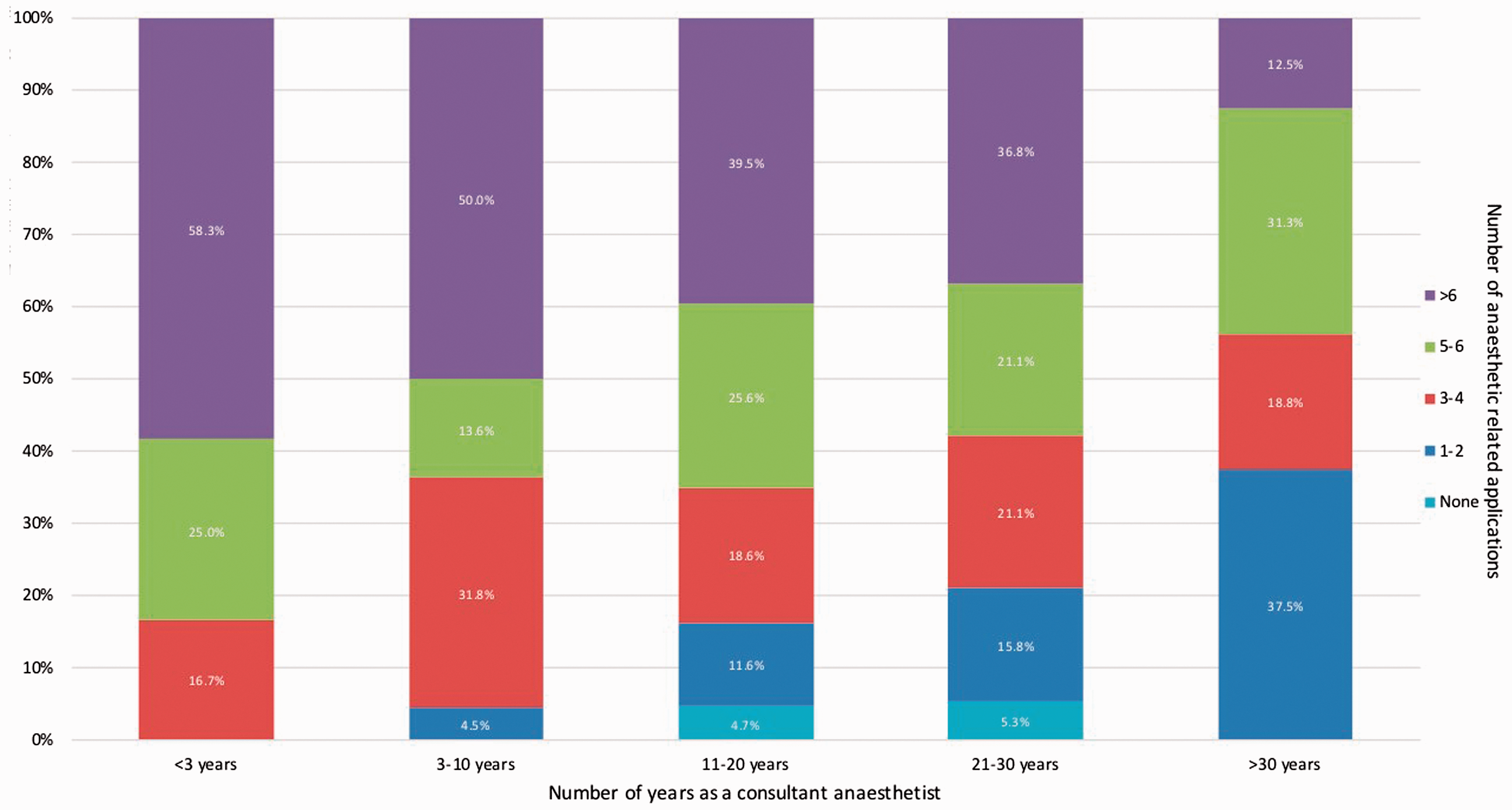
Relationship between number of applications relating to anaesthetic practice and number of years as a consultant anaesthetist.
The types of smartphone applications used by surveyed anaesthetists included applications for billing, clinical algorithms, clinical planning and assessment, drug referencing, prescription and dosing, academic journals, accessing patient results and communicating with colleagues.
Drug reference applications were the most frequently used applications, with 87.5% (n = 98) of surveyed anaesthetists stating their use. This was followed by prescription and dosing applications, which were used by 67.0% (n = 75) of responders. In addition to the listed applications, other applications that surveyed anaesthetists reported using included those that allow ‘access to hospital electronic medical record’, ‘Twitter for professional development’, ‘distraction of paediatric patients’ and ‘diary management’.
In addition to smartphone applications that required user-initiated downloading, surveyed anaesthetists reported using their smartphone for other built-in features such as a camera (n = 75), as a means to contact other clinicians for referrals or advice (n = 76), as a torch (n = 53) and as a stopwatch (n = 44).
Reliance on smartphones
Utilising grouped analysis, participants were 5.8 times more likely to agree (either ‘somewhat agree’ or ‘strongly agree’) (n = 81) than disagree (either ‘somewhat disagree’ or ‘strongly disagree’) (n = 14) that they rely on their smartphone to practise anaesthesia.
Smartphones and patient safety in theatre
As shown in Table 2 the majority (71.8%; n = 79) of surveyed anaesthetists agreed that the use of smartphones improves their patient safety in theatre. The likelihood of a respondent agreeing or disagreeing that smartphones improve patient safety in theatre was associated with the number of years’ experience as a consultant anaesthetist. Grouped analysis demonstrated that 90.9% of respondents with less than three years’ experience as a consultant agreed that smartphones improve patient safety, compared to 62.5% of those with more than 30 years’ experience agreeing with this statement (Figure 2).
Perceptions of smartphone use.
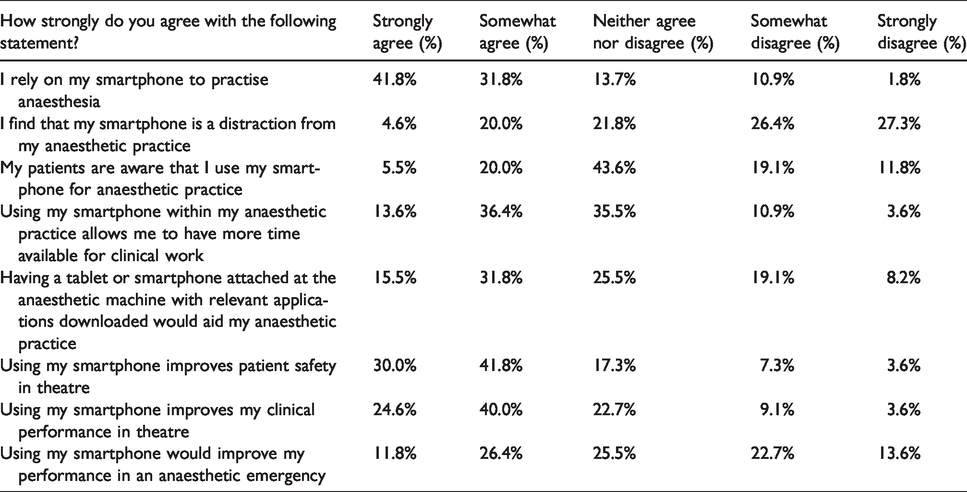
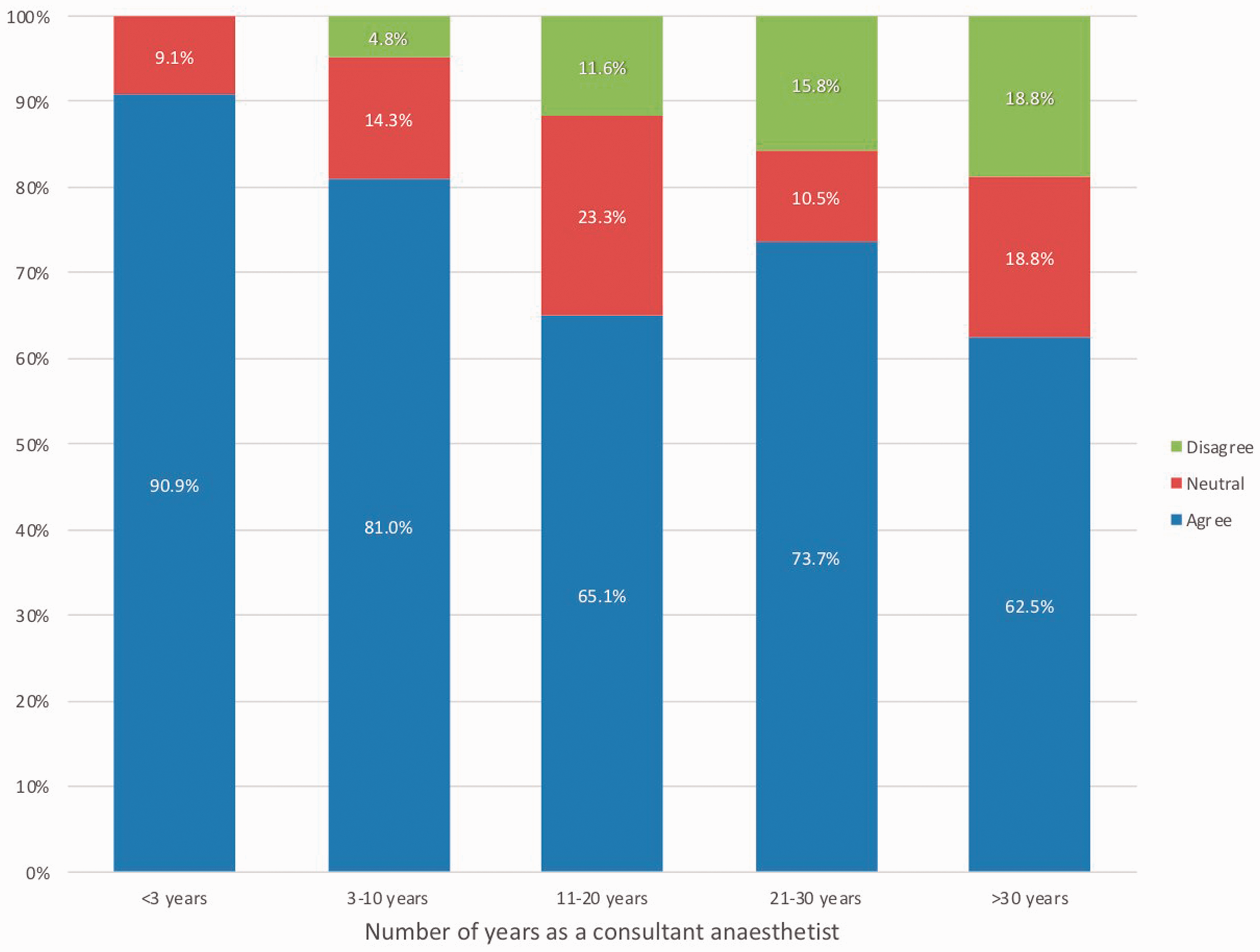
Perceptions on whether smartphone use improves patient safety in theatre.
Smartphones improving time efficiency in anaesthetics
Overall, 49.9% (n = 55) of respondents agree that smartphone use allows them to have more time available for clinical practice, while 35.4% (n = 39) neither agree nor disagree. Surveyed anaesthetists with less than three years’ experience as a consultant were more likely (72.1%) to agree that using a smartphone allows them to have more time available for clinical work compared to anaesthetists with more than 30 years’ experience (31.3%).
Smartphones as a distraction
Most (51.7%, n = 59) of the respondents disagreed that smartphones are a distraction from their anaesthetic practice. Whether or not smartphones were viewed as a distraction had some association with the number of years of experience as a consultant anaesthetist that participants had. Of those who had less than three years’ experience, none believed that their smartphone is a distraction from their work. When respondents had more than three years’ experience as a consultant anaesthetist, up to 27.3% (n = 27) agreed that their smartphone is a distraction.
Completion of survey on smartphone
There were differences in the perceptions of anaesthetists when comparing those who completed the survey on their smartphone compared to those who did not. Most (84.9%, n = 45) of those completing the survey on their smartphone agreed that they relied on their smartphone to practise, compared to (63.2%, n = 36) of those who did not. In a similar vein, (54.7%, n = 29) of those completing the survey on their smartphone perceived that their smartphone would improve their performance in an anaesthetic emergency, compared to (22.8%, n = 13) who did not.
Discussion
The results of our study suggest that the use of smartphones is ubiquitous during modern anaesthetic clinical practice. All respondents used their smartphone to aid anaesthetic practice in some way, with most using them several times per day. A multitude of various applications is currently being used in a professional capacity, most commonly drug reference and dosing and prescription applications. An ability to access such important information has the potential to improve patient safety according to the large majority (71.8%) of the respondents.
The use of other smartphone features such as the camera, torch and stopwatch were also perceived to be relevant to practice, suggesting that the smartphone has the potential to consolidate many different tools used within anaesthetics into one hand-held device. Along with allowing efficient retrieval of necessary information, this may explain why the majority of survey respondents felt that the use of smartphones allows them more time for clinical practice.
Our results suggest that anaesthetists’ use and dependence on smartphones varies with clinical experience. Respondents with less than three years’ experience report using smartphones more often in clinical practice, identify as being more reliant on them and report that smartphones improve patient safety. Moreover, respondents with less than three years’ experience did not believe that smartphones act as a distraction from work. This may be explained by the fact that less experienced anaesthetists are generally younger and are more likely to have undergone their training within a climate of ubiquitous smartphone technology use. However, this result may also reflect a lack of insight into the potential distractions posed by smartphones. This subset of respondents incorporates smartphones into their practice more frequently and perceives that these devices enable rather than hinder efficiency. Perhaps less clinical experience increases one's reliance on guidelines for practice, as well as requiring regular communication and support from their colleagues, both of which are enabled by smartphones. 7 A perceived lack of confidence among these less experienced clinicians has been proposed as the reason why professional society guidelines are more relied on in this cohort. 8
Notwithstanding the limitation that the emailed recipients represented less than a third of the currently registered anaesthetists in Victoria, and that there were only 113 respondents, we feel the results are to a degree representative of Australian consultant anaesthetic practice with respondents from a total of 55 hospitals. In addition, the demographic data of age, gender and private versus public practice of the respondents to this survey were comparable to Australian government published data. We feel our sample of the respondents in our survey is generally representative of the population of anaesthetists in Australia and adds strength to our results. 9 The poor response rate may be due in part to the likelihood that many email invitations were not received. The email list was obtained from a local anaesthetic department which was unaware if all of the listed emails were still in use. The primary limitation of this paper is difficulty in interpreting the survey results. Obviously, by design, this study is open to a degree of responder bias, particularly with regard to the estimated degree of distraction. Another potential limitation is that the data were collected by an electronic survey. Therefore, it is possible that individuals who are already inclined to use smartphones and electronic devices more were more likely to complete the survey, potentially skewing the results.
Previous studies conducted overseas have attempted to encapsulate the utility (and to a lesser degree the perceptions of) smartphone use by anaesthetists. 5 , 10 , 11 Nearly a decade ago, a study of smartphone usage among English anaesthetists noted the burgeoning potential for ‘innovative developments in patient care and monitoring’ made possible with smartphone integration with anaesthesia practice. 11 A study conducted in 2016 among Irish anaesthetists found similar results to our study that drug reference apps were the most commonly used application during clinical practice. 10 However, that study showed that nearly 10% of participants reported owning no apps related to anaesthesia. This is in comparison to just 2.7% of respondents in our study. This may be due to smartphones becoming more universal in recent years. In addition, a survey completed in 2015 found a similar trend regarding the reliance on smartphone usage among Turkish anaesthetists: those with less experience being more likely to use and have a greater reliance on smartphones in clinical settings. 5
Although it has been shown that smartphones are being used more broadly and frequently within professional contexts, the main criticism of their use within this environment is their potential to be a distraction. Within anaesthetics, situational awareness is paramount, as mistakes caused by distraction may have significant consequences for patients. 12 It has been proposed that smartphones act as a unique mechanism of distraction, and that interruptions caused by smartphones may impair an individual’s ability to multitask. 6 Jorm and O’Sullivan intimated that due to trainee anaesthetists having less experience and a narrower margin for cognitive overload, they are more at risk of distraction from smartphones. 6 Therefore, they concluded that junior anaesthetists should avoid the use of smartphones in theatre to reduce their risk of distractions and errors.
In contrast to this, our results suggest that anaesthetists with less experience perceive that their smartphones improve performance in both routine theatre cases and during anaesthetic emergencies to a greater degree than their more experienced colleagues. Less experienced respondents disagreed with the suggestion that smartphones are a distraction to clinical practice and instead perceive that they allow them more time for clinical work. Further clinical studies into distraction would be required to ascertain whether this perception is accurate or falsely reassuring.
Various medical associations such as the American Society of Anesthesiologists (ASA) and American College of Surgeons (ACS) have published recent statements focusing on various potential distractors in the operating room. The ASA make no mention of smartphones, instead urge for greater ‘education about distraction and mitigation strategies’. 13 Comparatively, the ACS directly acknowledges that smartphones ‘may pose a distraction and may compromise patient care’, but refrain from any direct bans of the devices, instead urging hospital organisations to incorporate ‘tools to overcome distraction’. 14 Despite the increasing use of smartphones within clinical practice, a study found in 2012 that no ASA closed claims injuries were attributed to distraction from smartphone use. 15 As of February 2020, the ASA closed claims database continues not to include smartphone use as a parameter of distraction. Notably, there is currently no published guideline or statement from the Australian and New Zealand College of Anaesthetists regarding smartphone usage in clinical practice.
In conclusion, this study explores the perceptions of currently practising anaesthetists in Australia with regard to the benefit and potential detriment of smartphone use within clinical practice. Our results suggest that the majority of anaesthetists in Australia are using smartphones regularly in their practice, and that many now perceive that they are now dependent on the advantages they offer. Our primary data indicate that anaesthetists use smartphones in many different ways, as their uses are broad and varied, and that smartphones make it possible to condense many useful functions into one device. Many of the respondents felt that smartphones not only improve clinician efficiency, but also aid in enhancing patient safety. In contrast to existing perceptions, respondents in our survey did not perceive smartphones to be a distraction from their work. These perceptions were more prominent in respondents with less than three years of specialist experience. These findings suggest that perhaps future generations of anaesthetists will have an increasing reliance on smartphones, and that smartphones are now perceived to be a useful aid for anaesthetic practice in Australia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.