
Abstract
The aim of this prospective cohort study was to describe the anaesthetic practices, rates of postoperative pain and the recovery trajectory of children having urgent dental extractions at our institution. Demographic, anaesthetic and surgical details of children undergoing dental extractions were obtained by case note review. Parent-proxy pain scores were collected via telephone on the day of surgery and on postoperative days, as well as details of analgesia given, behavioural disturbance, and nausea and vomiting. Follow-up was continued until each child no longer had pain. Datasets were analysed for 143 patients. Fasting times were prolonged, with 81 children (56.6%) fasted for over four hours from fluids. Moderate or severe pain was recorded in 14 children (9.8%) postoperatively on the day of surgery, with higher rates in children who had a greater number of teeth extracted. Low rates of moderate to severe pain were observed during follow-up, affecting six children (4.2%) on postoperative day 1 and three children (2.1%) on postoperative day 2 with primarily simple analgesia administered at home. Only eight children (5.6%) had nausea and/or vomiting on the day of surgery. Rates of reported behavioural disturbance at home were low, extending beyond the second postoperative day in only two children (1.4%), and only four children (2.8%) attended a dentist during the follow-up period. In conclusion, the low rates of pain and nausea and vomiting reported in the days following surgery for urgent dental procedures suggest that children can be cared for at home with simple analgesia.
Introduction
Paediatric day case surgery has become increasingly common and it is imperative that such cases are followed up to assess patient outcomes once discharged home. 1 However, there are little data to date on the trajectory of the return to normal function following dental extractions. Pain following paediatric dental treatment is likely the most common and prolonged symptom of postoperative morbidity; however, published studies vary widely in rates of pain after dental treatment, as they also vary in types of dental procedures, and anaesthesia and analgesia used. Some have demonstrated more significant morbidity related to postoperative pain, particularly in studies with longer procedures, 2 , 3 whereas others have shown low rates of moderate to severe pain and a faster recovery pain profile. 4 Early postoperative pain is associated with postoperative behavioural problems after day-case surgery for up to four weeks 5 and can result in unplanned healthcare re-attendances. 1 Effective pain management is therefore vital to enable patients to return to their normal activities and reduce the healthcare system burden.
Pain in children has traditionally been under-researched and under-treated. 1 , 6 For some day case surgical procedures, pain and behavioural disturbance occur for a number of days afterwards but this is often underappreciated by the healthcare profession as patients are at home and commonly not followed up closely. 7 In addition, there is mixed concordance between the parental perception of pain and the child’s rating of pain, 4 , 8 as well as parental misconceptions leading to the withholding of analgesia even when pain may be recognised. 9
This study was a quality improvement initiative reviewing the entire patient journey of children undergoing urgent dental procedures, from the immediate preoperative phase into the recovery phase, with a focus on anaesthetic practices, pain and behavioural disturbances, and specifically if it differed between trauma versus other reasons for dental extraction. The aim was to provide health professionals and parents with insight into pain levels and functional limitations postoperatively as well as the likely extent of the recovery period.
Materials and methods
Study design
The study was a prospective cohort study of children undergoing dental procedures at Princess Margaret Hospital (PMH), now known as Perth Children’s Hospital, the state paediatric tertiary care teaching hospital in Western Australia, with the aim of identifying the severity and duration of postoperative pain and other pain-related variables during the recovery period. Patients were enrolled opportunistically from the population presenting to the same-day procedure unit over a period of four years. The study was a quality improvement audit (QA12345) and written informed consent was deemed unnecessary by the institutional ethics committee. Verbal consent was obtained during the initial telephone call to each family. The Human Research Ethics Committee at the University of Western Australia recognised this audit (RA/4/1/5964).
Participants
Patients were included if they were under 18 years of age and had an urgent dental procedure at PMH, identified from the theatre management system (including emergency and semi-elective cases) requiring at least one extraction for trauma or dental caries/abscesses. Patients were excluded if they were having an additional non-dental painful procedure, if the child was under the care of the state, or if there were language or other communication barriers that would interfere with data collection. Patients were not excluded on the basis of their American Society of Anesthesiologists physical status.
Patients were recruited postoperatively and verbal consent was given by the parents or legal guardians of the patients during the first and each subsequent phone call. We aimed to contact families second or third daily and recorded data for each postoperative day. Patients were deemed ‘lost to follow-up’ if we were unable to contact the family within four days of patient discharge or within four days of the previous contact, or if consent was withdrawn at any time. This aimed to reduce recall bias and permit withdrawal of consent at any time.
Anaesthesia, analgesia and surgical techniques
Data on the preoperative, intraoperative and postoperative course until discharge were collected retrospectively from patient files and the online theatre management system. Data collection was observational without affecting the clinical management of patients. The anaesthetic technique was at the discretion of the treating anaesthetists and surgical techniques were at the discretion of the treating dentists. Medications given at discharge were at the discretion of the treating team, with standardised information sheets on analgesic advice given for patients with dental extractions.
Variables and data measurement
A standardised survey was used for data collection. Follow-up continued until reported pain scores were zero and patients were no longer taking any analgesic medications. A parental-proxy numerical rating scale was used for assessment of pain severity, both in hospital as well as postoperatively, and advice on how to use this scoring system was given to parents during the initial telephone contact. We classified scores 1–3 as mild pain, 4–6 as moderate pain and 7–10 as severe pain. In addition, we collected data on postoperative nausea and vomiting (PONV), unplanned healthcare re-attendance and a subset of the behavioural measures from the Parent’s Postoperative Pain Measure (PPPM) tool. These included whether the parent considered their child was having trouble sleeping, behavioural issues, interest in normal activities, whether the child was more easily upset and whether they were eating normally. A parental satisfaction rating was also collected.
Data analysis
Case details were entered into a database created for the audit. Data were collated using Microsoft Excel 2003 (Microsoft Corporation, Redmond, WA, USA). Data processing, the calculation of descriptive statistics and plot generation were performed using the R statistical environment (version 3.3.2 R Foundation for Statistical Computing, Vienna, Austria) and Jupyter (version 5.2.1; NumFOCUS, TX, USA). Demographic data are presented as median and range. Graphs are presented as mean pain scores per day (with error bars displaying the 10th to 90th percentiles) and proportions for other variables.
Results
Of 263 parents/carers approached postoperatively, seven were excluded as they did not meet inclusion criteria, three declined to be involved, 94 parents did not respond to two phone calls and a phone message if available and there were incomplete datasets for 16 patients once enrolled. Datasets were completed for 143 patients and these were included in the analysis. Table 1 summarises the patient demographics, surgical data and the anaesthesia management.
Patient demographics, surgical and anaesthetic characteristics.
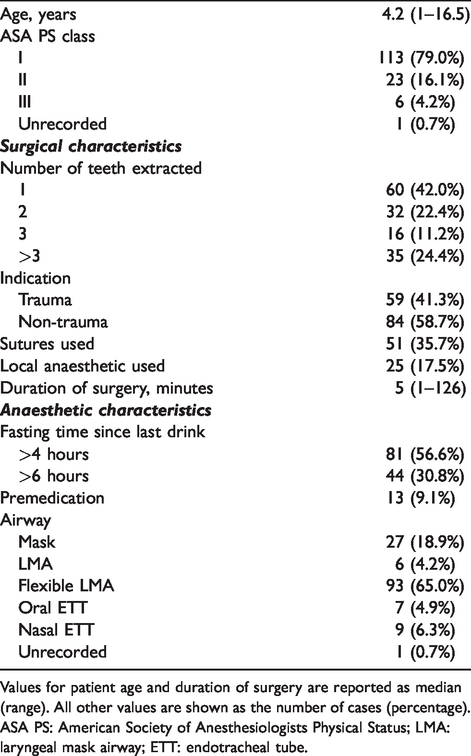
Values for patient age and duration of surgery are reported as median (range). All other values are shown as the number of cases (percentage).
ASA PS: American Society of Anesthesiologists Physical Status; LMA: laryngeal mask airway; ETT: endotracheal tube.
Pain severity and duration
In this review 12 patients (8.4%) had pain on waking, with two patients receiving rescue fentanyl in the post-anaesthesia care unit (PACU). Pain scores were not consistently recorded in the medical notes postoperatively, with only 83 children (58%) having a pain score documented at any time between arriving on the ward and before discharge. Of these, 14 patients had moderate to severe pain (score of 4 or more). Rates of moderate to severe pain following discharge were low and resolved by day 3, with six (4.2%) patients on postoperative day 1 and three (2.1%) patients on postoperative day 2 (Figure 1). Moderate to severe pain was more commonly reported in patients who had a greater number of teeth excised (Figure 2).
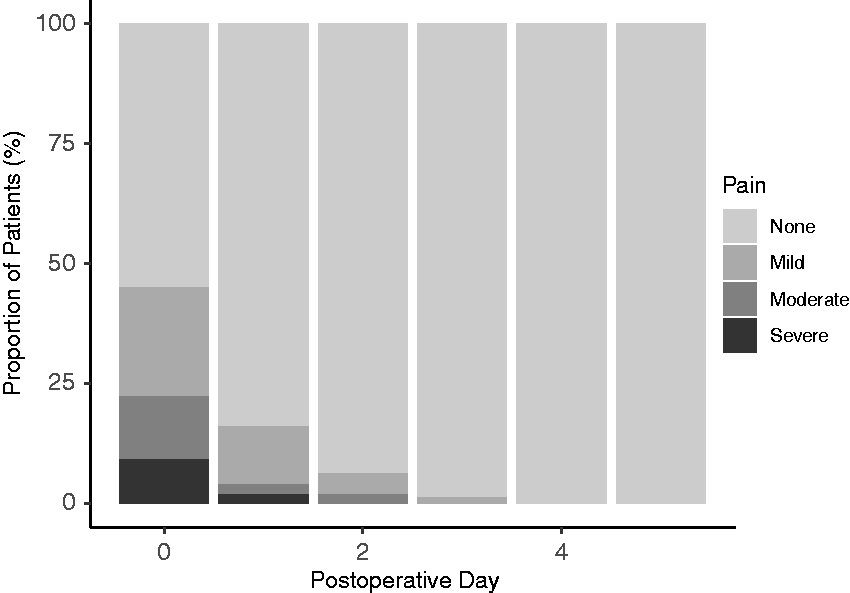
Rates of postoperative pain by severity during the follow-up period.
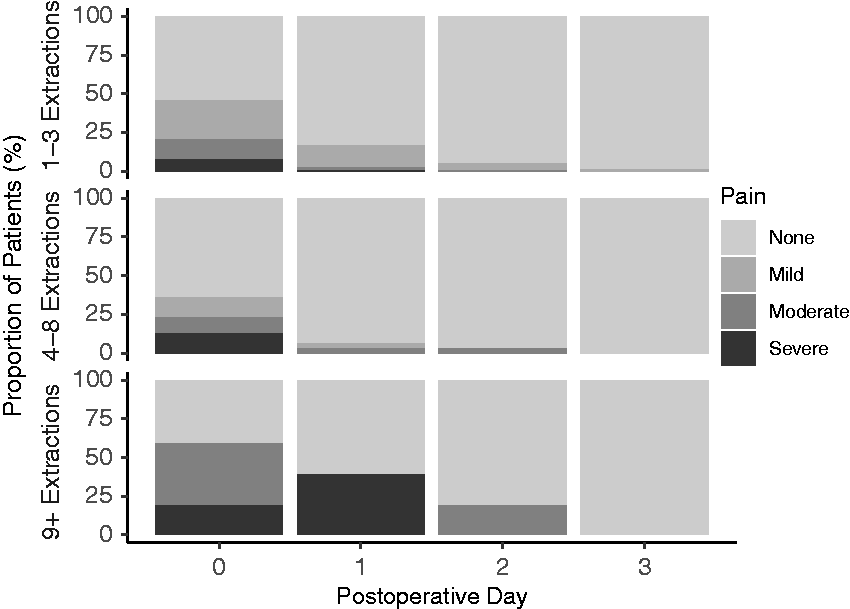
Rates of postoperative pain divided into categories based on the number of teeth extracted.
Local anaesthesia (lidocaine with adrenaline) was used intraoperatively in 25 children (17.5%); however, apart from a minor improvement in pain on waking, it did not seem to affect the number of patients with moderate to severe pain on the ward (12% with local used versus 9.3% without local used) or the amount of analgesia administered postoperatively (Supplementary Table 1). Cases that were indicated for trauma seemed to have lower rates of moderate to severe pain than infective cases (5.1% versus 13.1%) and this is likely related to having fewer teeth removed (mean 1.8 versus 3.2) (Supplementary Table 2). Patients who had at least one posterior tooth removed had more pain and more analgesia administered compared with patients who had anterior teeth extracted only; however, they also had a greater number of teeth removed (mean 3.5 versus 2.1) (Supplementary Table 3).
Analgesia
Table 2 summarises the analgesia used in pre-, intra- and postoperative stages. Intraoperative analgesia varied between patients with 129 children (90.2%) receiving intraoperative opioid, with fentanyl being used in all but seven children, who received morphine. On the general ward after discharge from the PACU, paracetamol was the most commonly administered analgesic and oxycodone the most commonly administered opioid. During the entire hospital stay, 129 children (90.2%) received an opioid, 72 children (50.3%) received paracetamol and 26 children (18.2%) received a non-steroidal anti-inflammatory drug (NSAID).
Different types of analgesia administered during the perioperative period and following discharge home. Values reflect the number of children (percentage).
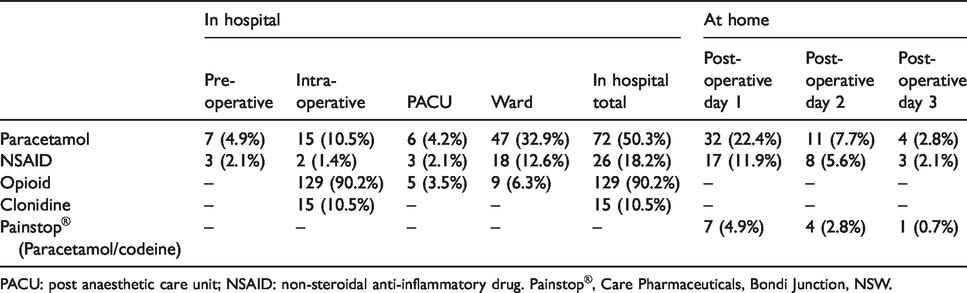
PACU: post anaesthetic care unit; NSAID: non-steroidal anti-inflammatory drug. Painstop®, Care Pharmaceuticals, Bondi Junction, NSW.
Nausea and vomiting
Intraoperative antiemetic agents were administered in 51 cases (35.7%), with ondansetron the most commonly used agent, followed by dexamethasone. Rates of PONV were low on the day of surgery. Only 3/143 children (2.1%) had postoperative nausea in PACU, two of whom had received intraoperative dexamethasone and intravenous fluid, whereas the remaining patient had received no antiemetic agents. On the postoperative general ward, 5/143 patients (3.5%) received antiemetics for nausea, with only two of these patients having vomiting episodes. On postoperative day 1, 5/143 (3.5%) patients were reported to have PONV and only one patient (0.7%) had PONV on day 2 and 3 postoperatively (Figure 3).
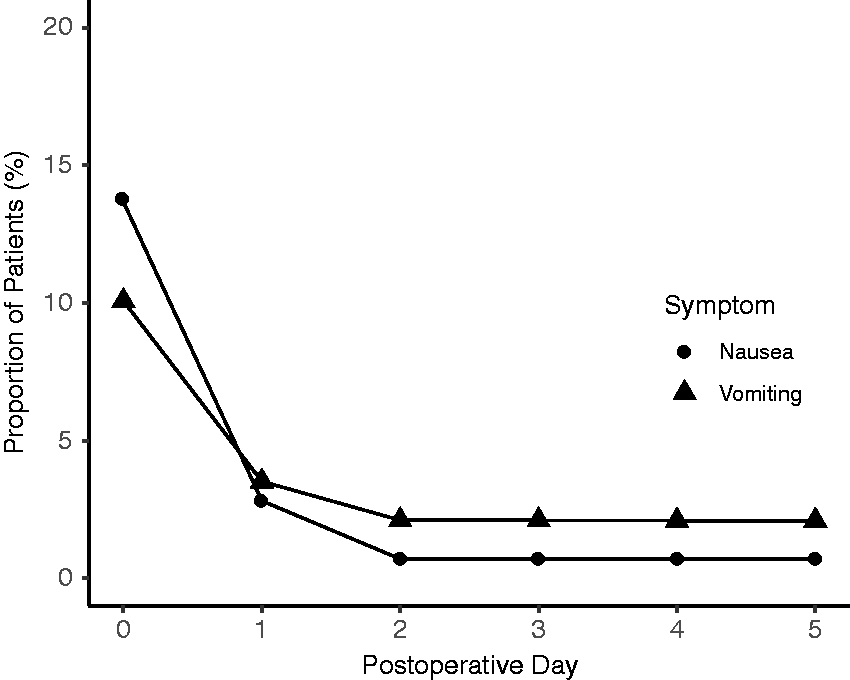
Rates of postoperative nausea and vomiting during the follow-up period.
Discharge information
Pain management information was communicated to parents by verbal and written means, with an information handout sheet on postoperative paracetamol and ibuprofen suggesting required dosing, with next dose times included. Only one patient had an analgesic prescribed for discharge (Painstop® Daytime, oral syrup containing paracetamol 24 mg/ml and codeine 1 mg/ml, Care Pharmaceuticals Pty Ltd, Bondi Junction, NSW). Painstop was a non-prescription drug in Australia until February 2018.
Behavioural disturbances
During follow-up, behavioural disturbances extended beyond the second postoperative day in only 2/143 children (1.4%). The most common behavioural disturbance was not eating normally, which affected 41/143 children (29%) on day 0, but this reduced to 14 children (10%) on day 1 and two children (1.4%) by day 3. Figure 4 demonstrates rates of behavioural disturbances postoperatively.
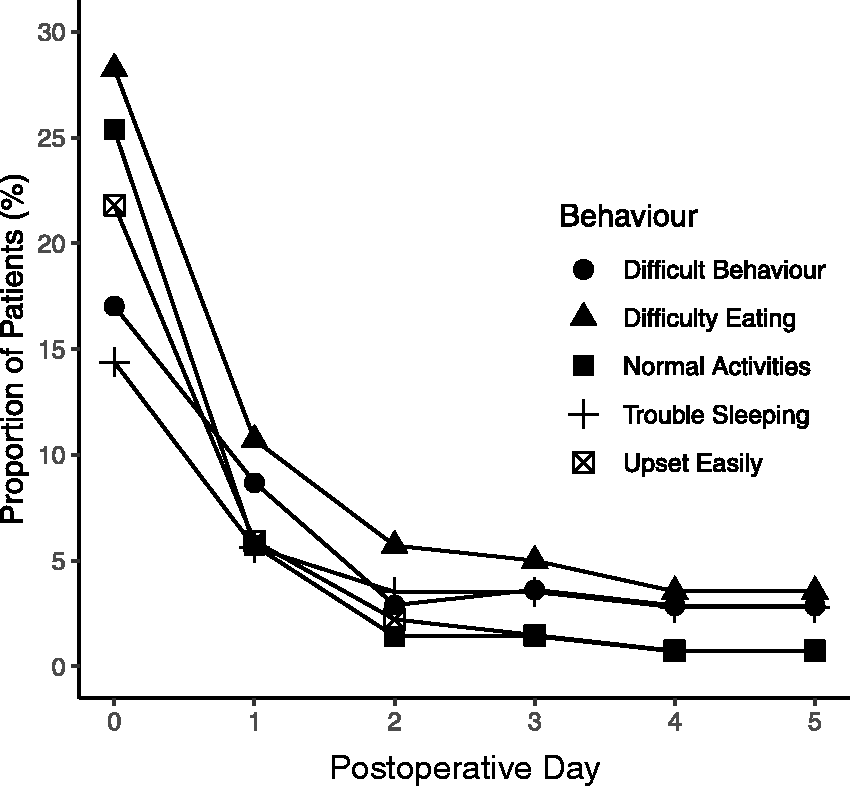
Rates of behavioural disturbances during the follow-up period.
Medical re-attendance
There were no cases of medical re-attendance to the hospital or general practitioner; however, 4/143 children (2.7%) did attend a dentist in the follow-up period.
Parental satisfaction
Parental satisfaction was very high overall, with only 6/143 cases (4%) where parents reported a score of being less than satisfied. The most common reason for this was concern about the long fasting times for their children.
Discussion
This study revealed anaesthetic practices for children receiving dental extractions in our institution and the patterns of pain and behavioural disturbances in these children until they have reached full recovery at home, which was generally within one to two days.
Over 90% of children received a dose of an intraoperative opioid, with fentanyl the most commonly used drug. Conversely, simple analgesics were used much less commonly. Low rates of intraoperative use may be at least partially explained by the short duration of the procedure with limited time to administer drugs, whereas low preoperative use may reflect anaesthetist preference or lack of time to plan or administer premedication for emergency cases. Nevertheless, this represents a missed opportunity to implement simple analgesia, in particular more cost-effective oral analgesia preoperatively instead of intravenous formulations intraoperatively. Premedication with NSAIDs has been shown in some studies to result in less pain following dental procedures in children. 10 , 11 Their use as a premedication in fasted patients is well established, for example preoperative ibuprofen in paediatric tonsillectomy 12 as well as dental extractions. 11 In addition, evidence that taking NSAIDs with food actually reduces adverse effects is weak 13 and in fact taking a single dose on an empty stomach results in more rapid absorption and therefore better analgesic effect in adult dental pain models. 14
There were low rates of pain reported in PACU on waking, with only 3.4% of children receiving a dose of opioid protocol. Although pain scores were poorly documented on the ward in general, 9.8% of children reported moderate or severe pain and 6.8% of children received an opioid on the ward, with oxycodone the most common opioid used. The low incidence of moderate or severe pain may be a reflection of both the short duration of cases in our study as well as the high rates of intraoperative analgesic use when compared to others. 15 The low use of NSAIDs peri-operatively and at home was disappointing given the dental extraction model is commonly used in acute pain studies and NSAIDs are positioned at the top of the Oxford league table. 16 We have tried to address this by encouraging ibuprofen use with paracetamol, and improved education and discharge information for use at home in children having more than three extractions. With this recommendation we feel there is little requirement for opioids post discharge. Reassuringly, pain largely resolved within the first 24 hours, as only 4.2% of children were reported by their parents as having pain from the first postoperative day and this tended to be associated with a greater number of teeth extracted. The time to recovery from pain is shorter in our study compared to others that looked at longer and more invasive procedures. 2 , 3
Interestingly, local anaesthetic use did not seem to affect the rates of moderate to severe pain observed; however, the overall numbers of patients receiving local anaesthetic were low. Despite potential benefit in reduction in risk of bleeding, the use of local anaesthesia in paediatric dental procedures under general anaesthesia is complicated by a number of factors. These include the risk of postoperative hyperalgesia, 17 , 18 risk of postoperative self-induced soft tissue trauma in the form of lip- and cheek-biting lesions and the potential delay in onset or reduction in efficacy of local anaesthesia administered in an area of infection (for example, a dental abscess). 19 A Cochrane review of this topic was unable to reach a conclusion on the benefit of local anaesthesia use in children having dental procedures under general anaesthesia, largely due to the heterogeneity of the studies. 20
Despite low rates of prophylactic antiemetic administration, rates of nausea and vomiting were low in the postoperative period, likely in part due to the short duration of anaesthesia. This supports previous findings that routine prophylactic administration of antiemetic drugs in paediatric day case surgery may be unnecessary. 21 On follow-up, 23 children (16.1%) were reported to have nausea or vomiting in the first 24 hours following surgery and this persisted beyond the first postoperative day in one case only. These low rates do not justify prescription of discharge antiemetics for all cases; however, identifying patients at increased risk, for example with the use of Eberhart’s simplified risk score, 22 may allow for targeted therapy and improved outcomes at home. Similarly, behavioural disturbance rates were low and largely resolved after the second postoperative day.
With regard to other anaesthetic practices, it was disappointing to note the prolonged fasting time for fluids, with 56.8% of patients having a greater than four-hour fast from fluids. The reasons for prolonged fasting in our study are likely multifactorial, including the low priority of these cases on the emergency list, in addition to parents erring on side of caution in following fasting guidelines, to avoid delays in the procedure. This has been noted frequently in other centres and is probably due to cases of greater clinical urgency being prioritised on emergency theatre lists ahead of patients for dental extractions. 23 , 24 Internationally, fasting guidelines for children have been undergoing scrutiny, with evidence to support the safety of more liberal fasting regimens. 25 , 26 Nevertheless, prolonged fasting was a recurrent complaint from parents in our study and a new guideline has been introduced in our institution that allows for clear fluids up to one hour prior to surgery, with active encouragement of clear fluid intake by day surgery nursing staff and ongoing review by the theatre coordinator if there are list order changes.
There was a high rate of use of the flexible laryngeal mask airway (LMA) for airway management (65% of cases), even in cases where surgery was a short duration. This is supported by a long history of safe use with evidence suggesting reduced perioperative respiratory adverse events compared to endotracheal intubation, 27 but may potentially be exposing patients to increased risk when compared with use of a facemask alone. 28
Study limitations
Our study included a wide range of patient ages and procedure durations, therefore a wide range of experiences may be expected in the recovery profiles seen. Half of all patients were aged four years or younger and half of all cases lasted no more than five minutes, which represents the typical patient presenting to our institution for urgent cases, for example, following dental trauma or abscess. Elective cases for complete oral rehabilitation, which are longer duration, were excluded from the study unless they had become urgent.
Parent-proxy pain scores are a useful alternative to the gold standard of self-reporting and parental 0–10 numerical rating scale has been shown to be a valid tool. 29 , 30 However, they have also been associated with underreporting of pain and this is a potential weakness in our study. 31 In addition, parents were not educated on how to evaluate nausea in children, which can also be difficult and may have resulted in underreporting of nausea in our study.
We did not use the complete PPPM questionnaire as it was deemed too onerous for parents, therefore potentially leading to reduced participation rates and increased selection bias. A subset of behavioural items from this tool was used instead and difficulty eating, which is not part of the formal questionnaire, was added as an important consideration in oral surgery.
Follow-up was continued until patients were not taking analgesia and pain scores reached zero; however, patients were not followed up further to ensure pain scores remained at zero. Furthermore, parental recall bias was a potential problem in our study given the nature of our phone call survey.
Conclusion
A minority (less than 10%) of children experience moderate or severe pain following urgent dental extraction procedures under anaesthesia. Moderate or severe pain was more common in patients having a larger number of teeth removed but did not seem to be related to the reason for extraction.
Overall, health professionals and parents can be reassured that the expected trajectory for patients who have short extraction dental procedures is a good recovery and return to normal activities within 48 hours with simple analgesia following discharge home. Efforts to avoid prolonged fasting times and use of simple analgesia in hospital and by parents could improve the overall perioperative patient experience.
Footnotes
Author Contributions(s)
Data curation; Formal analysis; Writing-original draft; Writing-review & editing.
Data curation; Writing-review & editing.
Data curation; Writing-review & editing.
Formal analysis; Writing-review & editing.
Data curation; Writing-review & editing.
Conceptualization; Writing-review & editing.
Conceptualization; Project administration; Writing-review & editing.
Conceptualization; Supervision; Writing-original draft; Writing-review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.