
Abstract
Strabismus correction surgery is the most common eye operation in children. Adults have approximately a 4% lifetime risk of developing strabismus. Current treatment options include pharmacological injection of botulinum toxin or bupivacaine, conventional corrective surgery, adjustable suture surgery and minimally invasive surgery. Repeated surgery is common as each operation has a 60%–80% chance of successful correction. The benefits of early surgical correction in large-angle strabismus in children outweigh the risks of anaesthesia. General anaesthesia is suitable for patients of all age groups, for complicated or repeated surgery, and bilateral eye procedures. Regional ophthalmic block reduces the incidence of oculocardiac reflex and emergence agitation, and provides postoperative analgesia, but requires a cooperative patient as many experience discomfort. Topical anaesthesia has been used in pharmacological injection, minimally invasive surgery, uncomplicated conventional strabismus surgery and some adjustable suture strabismus surgery. Its use, however, is only limited to cooperative adult patients. Prophylactic antiemesis with both ondansetron and dexamethasone is recommended, especially for children. A multimodal analgesia approach, including paracetamol, intravenous non-steroidal anti-inflammatory drugs, topical local anaesthetic and minimal opioid usage, is recommended for postoperative analgesia, while a supplementary regional ophthalmic block is at the discretion of the team.
Keywords
Introduction
Strabismus occurs in 3%–5% of children worldwide, 1 and its correction is the most common paediatric eye surgery. The lifetime risk of developing adult-onset strabismus is approximately 4%, with a peak incidence in the eighth decade. 2 The current treatment options include injection of certain drugs into the affected extraocular muscles and conventional corrective surgery. Recent innovative surgical procedures include adjustable suture surgery and minimally invasive surgery such as minitenotomy and miniplication. These treatment options can be performed with either regional anaesthesia or general anaesthesia.
The majority of the published anaesthetic literature focuses on paediatric patients. In addition, there is no discussion of the newer surgical procedures for strabismus and their relevant anaesthetic techniques. The aims of this narrative review article are to provide a brief background on both conventional and innovative strabismus surgery, and discuss the anaesthetic considerations associated with these procedures in both children and adults.
Search strategy
A literature search was conducted in September 2019 using MEDLINE (Ovid) with the aim of identifying English language articles published between January 1998 and September 2019. The search words used included ‘anaesthesia’ in combination with ‘strabismus’. Five hundred and seventy-nine articles were retrieved. The authors examined the articles in term of quality and relevance to anaesthesia for strabismus surgery. Further related key articles were retrieved through their references. As a result, 95 articles related to ocular anatomy and physiology, causes of strabismus, pharmacological and surgical treatment options and anaesthetic practices were included in this review.
Strabismus
Orthotropic alignment of the eyes (both eyes focused at the same spot) occurs by one month of age. 3 The brain then combines the two images, one from each eye, into a single, three-dimensional image and this enables binocular vision (stereopsis). Visual development, resulting in the brain learning to interpret signals from an eye, occurs during the first seven or eight years of life.
Strabismus (misalignment of the eye/eyes) results from an imbalance in extraocular muscle function. Consequently, two different images, one from each eye, are transmitted to the brain, resulting in loss of visual depth. In children, the brain may suppress the image from the weaker eye and this impairs visual development and may result in amblyopia (decreased vision in a normal healthy eye). The prognosis is good if correction of strabismus is performed as early as possible before the child reaches the age of eight years. However, if untreated, amblyopia may become permanent. In adults, strabismus may cause diplopia because the brain cannot suppress the overlapping images.
Strabismus may involve one or both eyes, resulting in different presenting signs and symptoms. The affected eye can be deviated outwards (exotropia), inwards (esotropia), upwards (hypertropia) or downwards (hypotropia). The deviation may be intermittent or constant, large magnitude (large angle) or small magnitude (small angle). Symptoms include diplopia, loss of stereopsis, headache, inability to read comfortably, fatigue when reading and amblyopia. It interferes with normal eye contact with others, often resulting in psychosocial issues.
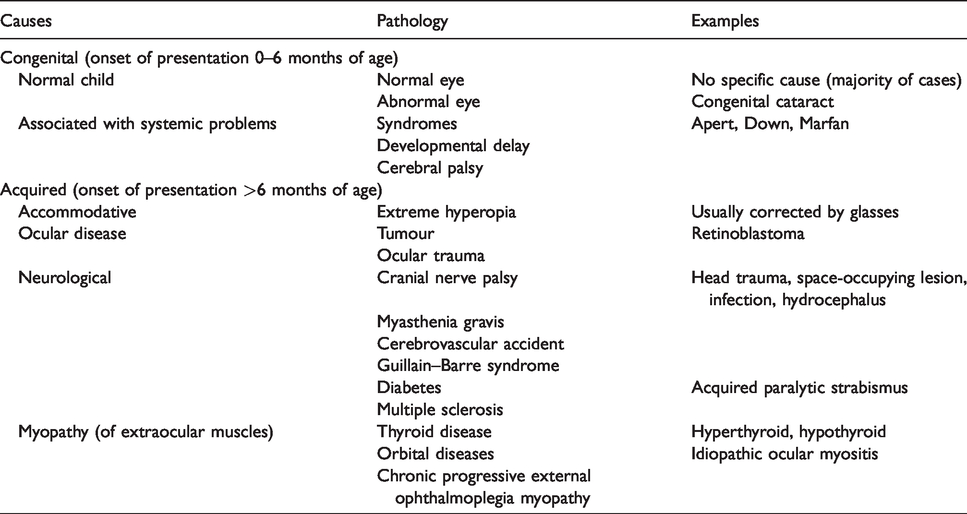
Risk factors for strabismus include premature birth, low birth weight, smoking throughout pregnancy, family history, 4 Down syndrome (29%), 5 cerebral palsy (53%) 6 and syndromes with craniofacial dysostosis (up to 90%). 7 The causes of strabismus are summarised in Table 1.
Causes of strabismus.
Background of strabismus surgery relevant to anaesthetic practice
Anatomical aspects of the eye in corrective strabismus surgery
The movement of the globe is controlled by six extraocular muscles. There are four rectus muscles (medial and lateral rectus muscles (horizontal movement), superior and inferior rectus muscles (vertical movement)) and two oblique muscles (superior and inferior oblique muscles (torsional movement)). The rectus muscles arise from the annulus of Zinn near the apex of the orbit and insert onto the outer surface of the globe anterior to its equator forming an incomplete cone. The superior rectus, medial rectus, inferior rectus and inferior oblique muscles are innervated by the oculomotor nerve (cranial nerve III), superior oblique muscle by the trochlear nerve (IV) and lateral rectus muscle by the abducens nerve (VI). The nasociliary nerves are the sensory nerves to the cornea and the perilimbal and superonasal quadrant of the conjunctiva. Sensation to the remainder of the conjunctiva is mediated by the lacrimal and frontal nerves that lie outside the muscle cone.
Tenon’s capsule, a fascial sheath, surrounds the globe and separates it from orbital fat. Anteriorly, Tenon’s capsule merges with conjunctiva before inserting to sclera 3–8 mm away from the limbus. Posteriorly Tenon’s capsule fuses with meninges around the optic nerve and sclera at the optic nerve exit. The tendons of these six extraocular muscles pierce the sheath as they pass to their insertions on the globe. 8
Treatment options for strabismus
Optical aids
Optical lenses (glasses) are indicated in certain forms of strabismus, for example, accommodative esotropia. Prisms are useful to relieve diplopia especially in small-angle strabismus. Patching of the dominant eye often improves amblyopia; however, it does not correct the visual axis misalignment.
Injection of drugs into extraocular muscles
Injection of botulinum toxin or bupivacaine into affected extraocular muscles is effective in the management of mild strabismus. Within two to four days of an injection of botulinum toxin to the overactive extraocular muscle, the muscle is paralysed and unopposed antagonist muscle(s) strengthen and pull the eye to the opposite direction, often causing an overcorrection. The effect of botulinum toxin lasts up to three months. 9 Repeated injections are often required.
When bupivacaine was injected into animal muscles, an immediate massive degeneration of the muscle fibres occurred, but regeneration began within two days, and the muscle fibres returned to pre-injection size and strength by three weeks. Further regeneration continued and resulted in muscle hypertrophy. 10 Using this myotoxicity cycle, bupivacaine has been injected into the weaker extraocular muscles to promote hypertrophy and strengthen the muscle.
Botulinum toxin and bupivacaine can be used in combination to weaken and strengthen the injected extraocular muscles, respectively, in the treatment of strabismus. 11 In cooperative adult patients, the injection can be performed transconjunctivally with electromyographic (EMG) guidance under topical anaesthesia 10 , 12 while intravenous sedation is required for anxious or younger patients. 9 In children less than six years of age, open exposure and injection into the muscle under direct visualisation is preferred by some surgeons.
Complications of botulinum toxin injection include ptosis and iatrogenic strabismus (due to leakage of botulinum toxin to surrounding muscles). Serious sight-threatening complications, such as scleral perforation, retrobulbar haemorrhage and inadvertent intraocular injection, can also occur. 9
Conventional strabismus surgery
Conventional strabismus surgery attempts to realign the eyes by weakening (recession), strengthening (resection), or changing the position of one or more of the extraocular muscles (transposition). The Faden operation is a more complex myopexy technique (posterior fixation of a suture through the muscle behind the equator without any surgical separation). 13 The extent of surgical correction is influenced by the magnitude of deviation.
Adjustable suture strabismus surgery
Adjustable suture strabismus surgery that allows the surgeon to fine-tune the extraocular muscle position in the immediate postoperative period has become more popular since 1975. It is especially useful in complicated strabismus surgery, such as repeated surgery, trauma and thyroid eye disease. 14 The surgery is commonly performed as a two-stage procedure. Only cooperative adults and selected teenagers are suitable for this procedure.
At the first stage, conventional strabismus surgery is performed with an adjustable suture knot under general anaesthesia or regional ophthalmic block depending on the preference of the surgeon and the patient. The second stage is delayed until the patient and the eyes have recovered from the effects of anaesthesia. In the second stage, eye alignment is assessed and the muscle sutures are adjusted to achieve the desired outcome. It is performed with the patient awake under topical anaesthesia. Intraoperative suture adjustment is possible in a single stage if the procedure is performed under topical anaesthesia, as the extraocular muscle functions are intact. 15
Minimally invasive procedures
Minitenotomy, a muscle-weakening procedure, involves the detachment of the central 3–4 mm of the rectus muscle tendon. 15 Miniplication, a muscle-tightening procedure, is performed by advancing the central 3–4 mm of the rectus muscle and suturing it to the sclera. 16 These are options for the correction of small-angle strabismus. As these procedures do not require hooking or complete resection of the rectus muscle, they can be performed under topical anaesthesia without sedation in cooperative adult patients. In addition, the effect of the initial operation can be assessed immediately before deciding whether a second procedure is required on another muscle.
The ideal timing of strabismus surgery in very young children
Infantile esotropia (inward deviation of eye that begins in the first six months of life), affecting one in every 100–500 people, commonly has large-angle deviation. 17 The main indication for surgery from a patient/parents’ perspective is cosmetic appearance.
From a surgical perspective, early correction (≤10 months of age) has been advocated as there is growing evidence that early surgery improves sensory and ocular motor outcomes with no adverse long-term effects. 17 There are concerns of adverse neurological effects in children exposed to general anaesthesia. The GAS study reported that slightly less than one hour’s (54 minutes) exposure to general anaesthesia in early infancy for inguinal herniorrhaphy did not alter neurodevelopmental outcomes at five years compared with awake regional anaesthesia. 18 In addition, in a large cohort study of over 10,000 siblings paired aged five to six years, children who had surgical procedures under general anaesthesia were not found to be at increased risk of adverse child development outcomes compared with their biological siblings who did not have surgery. 19 As the duration of most strabismus surgery is one to two hours, the benefits of early surgical correction in large-angle (>20 prism dioptres) strabismus in children outweigh the risks of anaesthesia.
Anaesthetic considerations
Preoperative considerations
In children, specific enquiry about upper respiratory tract infections, prematurity and its associated complications, developmental delay, cerebral palsy and congenital syndromes should be made. The clinical features of strabismus-associated congenital syndromes are summarised in Table 2.20–28 Evaluation of the airway and cardiac status is essential because some syndromes are associated with craniofacial and cardiac anomalies.
Syndromes associated with strabismus and their clinical features.

CNS: central nervous system; CVS: cardiovascular system.
As there is usually an underlying cause for adult-onset strabismus, a thorough evaluation should be performed with specific questions about thyroid function, bleeding disorders and anticoagulants. These patients are often elderly and may be on antithrombotic drugs, particularly when the underlying cause is a cerebrovascular accident. The risk of bleeding threatening vision in strabismus surgery is low even if antithrombotic treatment is continued. 29 , 30 Kemp et al. reported three cases of strabismus surgery without any excessive bleeding in the perioperative period in patients taking warfarin. 31
Strabismus surgery for thyroid eye disease should be delayed until the patient is euthyroid and eye disease is stable for at least six months. 32 Routine preoperative investigations are not required in strabismus surgery. However, specific investigations are indicated by patient comorbidities. Echocardiography, for example, may be required in syndromes associated with congenital cardiac anomalies. Magnetic resonance imaging may be required for some patients (e.g. atypical presentations, acute onset, swollen optic disc, neurological causes such as cranial nerve VI palsy, etc.) to exclude intracranial pathology.
Malignant hyperthermia
Strabismus was considered as a risk factor for malignant hyperthermia. This is no longer considered valid. Halsall did not show any association with strabismus in a review of over 2500 patients tested for malignant hyperthermia susceptibility. 33 It is common practice to use volatile anaesthetic agents in children having strabismus surgery and no increase in the incidence of malignant hyperthermia has been reported. 34
Pacemakers and automated implantable cardioverter defibrillators
Bipolar electrocautery, used in strabismus surgery, carries a lower risk of electromagnetic interference associated with implantable cardiac devices compared with monopolar electrocautery. In a survey of ophthalmic anaesthesiologists, 96% of the respondents did not convert a pacemaker to asynchronous mode and 86% did not inactivate an automated implantable cardioverter defibrillator and no adverse incidences were reported. 35 However, modification to these cardiac devices should be considered given the close proximity of the electrocautery to the cardiac device.
Intraoperative considerations
Topical vasoconstrictor
Application of a topical vasoconstrictor (e.g. apraclonidine, phenylephrine), preferred by some surgeons, may cause adverse effects such as raised blood pressure, arrhythmia, pulmonary oedema 36 and cerebrovascular accident. Caution should be exercised in patients with a history of hypertension, ischaemic heart disease and cerebrovascular accident. Furthermore, surgical incision in a pool of eye drops containing a vasoconstrictor 37 or direct application of drops to the raw tissue surface of the extraocular muscles 36 should be avoided as the conjunctival membrane barrier is disrupted and this results in increased systemic absorption with a higher incidence of systemic side-effects. There have been case reports of severe hypertension and pulmonary oedema in children as a consequence. 36 , 37 Phenylephrine also dilates the pupil and may affect adjustable suture strabismus surgery.
Oculocardiac reflex
The oculocardiac reflex (OCR) is defined as an over 20% decrease in heart rate from the baseline or the presence of arrhythmia induced by pressure on the globe or traction on extraocular muscles. OCR often results in sinus bradycardia, but atrioventricular block, complete heart block, ventricular ectopics, ventricular fibrillation, or even asystole have been reported.38–41 Symptoms are generally mild and transient in most patients. 42 Immediate cessation of muscle traction usually restores normal cardiac rhythm. In severe cases, an anticholinergic agent (atropine 7 μg/kg or glycopyrrolate 1 μg/kg) may be required. 43
The incidence of OCR during strabismus surgery is reported to be as high as 86% in paediatric patients. 38 , 44 Risk factors include hypercarbia, 40 hypoxaemia, 42 light anaesthesia (bispectral index >50) 45 and the magnitude and duration of the inciting stimulus. 40 Acute traction on the extraocular muscle is more reflexogenic than gradual traction. Generally OCR decreases with repeated stimulation (fatigue). 40 The medial rectus muscle has shown more resistance to fatigue; however, it was just as reflexogenic as the other extraocular muscles exposed to the same stimulus. 40
The choice of anaesthetic agent or technique also affects the OCR. OCR occurred less frequently in general anaesthesia with sevoflurane than with halothane. 46 There was no difference in the incidence of OCR between sevoflurane and desflurane. 47 Although intraoperative ketamine (1.0–1.5 mg/kg) was more effective than atropine in decreasing the incidence of OCR, 38 , 39 it was associated with increased incidence of postoperative nausea and vomiting (PONV) and prolonged length of stay in the post-anaesthetic care unit. 39 Combined ophthalmic regional block and general anaesthesia reduced the incidence of OCR (from 94% to 13%) in paediatric patients. 48 General anaesthesia maintained with volatile anaesthetic agents decreased the incidence of OCR compared with propofol (22% versus 49%) in paediatric strabismus surgery. 49 Intraoperative administration of a rapid acting opioid (such as fentanyl, sufentanil 50 and remifentanil) 51 or dexmedetomidine 52 potentiates OCR during strabismus surgery.
Prophylaxis with an anticholinergic for OCR is effective 53 , 54 and has been used routinely in some practices. 43 , 54 , 55 However, with the cooperation of ophthalmic surgeons and gentle traction on extraocular muscles, this may not be necessary.
The incidence of OCR is lower in adult strabismus patients (13%–22%). 56 Adult patients undergoing strabismus surgery who received prophylactic atropine (10 μg/kg) had a low risk of OCR and PONV, independent of the general anaesthetic technique. 56 There have been conflicting reports on the association between OCR and PONV. Allen et al. reported that children with positive OCR were three times more likely to vomit than those without the reflex, 44 whereas Aly et al. found no association. 57
Oculorespiratory reflex
The oculorespiratory reflex (ORR), which results in bradypnoea with irregular and shadow breaths, hypercarbia and even respiratory arrest precipitated by traction on the extraocular muscles has been observed in children during strabismus correction. 58 This is less frequent with general anaesthesia with sevoflurane compared with halothane. 46 Atropine, glycopyrrolate or bilateral vagotomy had no effect on ORR in animals while retrobulbar block could completely abolish it. 59
Forced duction test
The forced duction test, performed by gripping the limbus with forceps and moving the globe in multiple directions, is employed by surgeons to detect any restriction in eye movement. 60 Resistance to movement of the globe (positive result) indicates a ‘restrictive’ cause of strabismus while free movement without any resistance (negative result) indicates a ‘neuropathic’ aetiology. The findings of the forced duction test will determine the type of corrective strabismus surgery required. It can be performed in cooperative patients under topical anaesthesia as an office-based procedure. Alternatively, it is performed after induction of general anaesthesia and before commencing surgery in children and uncooperative adults.
Suxamethonium causes a sustained contraction of the extraocular muscles for up to 20 minutes and therefore interferes with the interpretation of the forced duction test. 61 The mechanism of this prolonged effect of suxamethonium on the extraocular muscles compared with other peripheral skeletal muscles is unclear. When suxamethonium is used, the forced duction test should be delayed for about 20 minutes after its injection so that its effects on the extraocular muscles have dissipated. Non-depolarising muscle relaxants do not interfere with the forced duction test. 61
Antibiotic prophylaxis
Routine administration of intravenous antibiotic prophylaxis is not recommended because ophthalmic procedures (except nasolacrimal duct surgery) are not associated with bacteraemia. Infection after strabismus surgery is rare, with an estimated incidence of one in 1100 to one in 1900. 62
The choice of anaesthetic technique
General anaesthesia
General anaesthesia is the most commonly used anaesthetic technique in strabismus surgery because it is suitable for: (a) patients of all ages; (b) complicated or repeated surgery; and (c) bilateral eye procedures. Inhalational induction in children with sevoflurane in oxygen with/without nitrous oxide is commonly used.63–66
Sevoflurane, compared with halothane, is associated with a lower incidence of OCR, dysrhythmia and airway irritability. 46 However, it is associated with an increased incidence of emergence agitation (sevoflurane 33% versus halothane 0%). 67 Maintenance of anaesthesia with propofol, compared with volatile anaesthetic agents, reduces emergence agitation 68 and PONV 69 but increases the incidence of OCR 49 in strabismus surgery.
The airway can be secured with either a laryngeal mask airway63–65 or an endotracheal tube. 70 , 71 Should there be any concern with airway patency with a laryngeal mask airway, it should be changed to an endotracheal tube before surgery commences because manipulation or exchange of the airway device in the middle of the operation may contaminate the surgical field. Assisted or controlled ventilation is preferred over spontaneous breathing as hypercarbia and the additive effects of volatile anaesthetic agents and the ORR increase the risk of an OCR. The non-depolarising muscle relaxants are the preferred neuromuscular blockers because they do not interfere with the forced duction test.
Regional anaesthesia
Ophthalmic regional block can be used as the primary anaesthetic technique for strabismus surgery. However, while complete akinesia is achieved, many patients still experience discomfort during muscle traction and conjunctival manipulation. Consequently, many anaesthetists employ regional anaesthesia only in medically unwell patients. Alternatively ophthalmic regional block can be used to supplement general anaesthesia, especially in children, and it is often performed by the surgeon during surgery. 72 , 73
The advantages of ophthalmic regional blockade include a reduced incidence of OCR and emergence agitation, postoperative analgesia and decreased PONV. 48 , 72 , 74 The contraindications include the presence of scars/adhesions from previous surgery, which can interfere with the spread of local anaesthetic (LA) solution and the insertion of a sub-Tenon’s block. Anatomical distortion, resulting from a large volume of injected LA solution, may interfere with the accuracy in adjustable suture strabismus surgery. Furthermore, the globe occupies nearly 50% of the orbital volume at birth, 33% at four years and only 22% in adulthood. Consequently, the risks of complication from sharp needle block are potentially higher in children than in adults. 75 Clinical conditions associated with enophthalmos (e.g. traumatic orbital fracture, metastatic carcinoma of the breast) are potentially associated with a higher risk of complications from sharp needle block as the globe is displaced posteriorly into the orbit. It is best avoided in patients with thyroid eye disease as the orbit is already congested with adipose tissue and myofibroblasts.
Topical anaesthesia
Topical anaesthesia76–79 avoids the serious complications associated with general anaesthesia and ophthalmic regional blockade. It is suitable for a wide range of corrective treatment for strabismus, including pharmacological injection, conventional surgery, adjustable suture surgery and minimally invasive surgery.
Topical anaesthetic techniques include simple topical eye drops, gel and the application of sponges soaked with LA into the superior and inferior fornices for 10–15 minutes. The anaesthetic effect with gel or soaked sponges is superior to that of topical drops. 78 , 80
Topical anaesthesia is suitable for surgery on medial and lateral rectus muscles. It should be avoided in other extraocular muscle operations and revision strabismus surgery as these often involve difficulties in surgical access resulting in patient discomfort. 80 Pain and discomfort, especially during traction and detachment of the extraocular muscles, are common. 78 , 81 , 82 Intravenous sedation is often required for patient comfort. Careful selection of motivated and cooperative patients is paramount to its success.
Complications of strabismus surgery and implications for anaesthesia
The complications of strabismus surgery are summarised in Table 3. Globe perforation (incidence of 0.08%), 83 potentially leading to retinal detachment, may require conversion from topical anaesthesia to ophthalmic regional block or general anaesthesia for surgical repair. Precautions should be taken, similar to an open globe injury, during the conversion to minimise the risk of the extrusion of ocular content.
Complications of strabismus surgery.
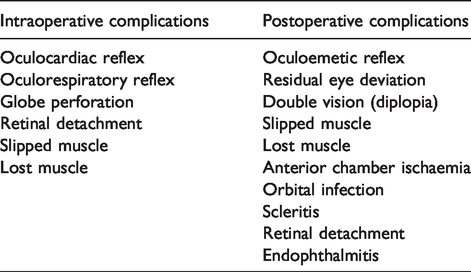
The incidence of slipped muscle (retraction of detached extraocular muscle posteriorly within its muscle capsule) and lost muscle (both muscle and its capsule retract posteriorly into the orbit) is approximately 0.067% and 0.02%, respectively. 83 These complications may require conversion from topical or regional anaesthesia to general anaesthesia to facilitate exploration of the globe.
Postoperative considerations
Postoperative nausea and vomiting
Early (six hours after operation) and late (48 hours after operation) vomiting occurred in 54% (range 18%–88%) and 59% (range 43%–97%), respectively, in paediatric strabismus patients who received no antiemetic prophylaxis. 49 In adult patients, PONV was relatively less (30%), independent of the general anaesthetic technique used. 56 The exact mechanism of the high incidence of PONV following paediatric strabismus surgery is unclear. An oculo-emetic reflex, involving the ophthalmic division of the trigeminal nerve and the vomiting centre in the medulla, has been proposed. 84
Many anaesthetic-related factors influence PONV. Ophthalmic regional blockade inhibits the sensory afferent pathway and reduces the incidence of PONV. 48 Adequate hydration with intravenous crystalloid (15–30 ml/kg), 85 maintenance of anaesthesia with propofol, 69 use of topical LA 48 and minimum opioid usage, 86 have also been reported to reduce the incidence of PONV.
Surgical technique also influences the incidence of PONV. Gentle surgical manipulation was associated with reduced PONV 48 while the Faden operation was associated with increased PONV. 13
In a systematic review and meta-analysis, the addition of a single antiemetic prophylaxis (ondansetron 150 μg/kg or droperidol 75 μg/kg) to inhalational anaesthesia appeared equally effective compared with total intravenous anaesthesia in reducing the incidence of PONV in paediatric strabismus patients. 87 However, the incidence of PONV was still unacceptably high (one in three children) in both groups, indicating that multimodal antiemetic prophylactic measures should be employed. In addition, total intravenous anaesthesia is associated with increased bradycardia from OCR compared with volatile anaesthesia. 87 Hence, a volatile anaesthesia technique with prophylactic antiemetic agents is often employed. 39 , 57
Droperidol is seldom used as the primary antiemetic in children because of risks of extrapyramidal symptoms and drowsiness. 87 It also received a controversial ‘black box warning’ in 2001 from the US Food and Drug Administration because of its prolongation of the QT interval and associated arrhythmia. A lower dose of droperidol (25 μg/kg) has been supported as a second-line antiemetic in the 2016 guidelines by the Association of Paediatric Anaesthetists of Great Britain and Ireland. 88
The current recommendation is prophylactic ondansetron (150 μg/kg, maximum 4 mg) and dexamethasone (150 μg/kg, maximum 8 mg) combination for strabismus surgery in children. 88 The same combination is also often administered prophylactically in adults. 86
Postoperative analgesia
Direct comparisons between intravenous non-steroidal anti-inflammatory drugs (NSAIDs) and intravenous opioids showed no difference in postoperative pain scores or supplementary analgesic requirements (diclofenac versus morphine; ketorolac versus pethidine; ketorolac versus fentanyl). 89
Topical NSAIDs (e.g. ketorolac) or topical LA (e.g. amethocaine) alone provided inadequate analgesia in paediatric strabismus surgery. 90 Pain scores were not reduced by the use of topical NSAIDs compared with placebo or topical LA. 89 , 91 The efficacy of oral or rectal paracetamol as part of multimodal analgesia has not been compared with other agents in several studies. 91
Regional ophthalmic block reduces perioperative analgesic requirements compared with placebo. 72 , 74 , 75 , 92 , 93 It reduces PONV, may improve perioperative analgesia in comparison with opioids, but provides no benefit over topical LA. 89
In general, a multimodal analgesic approach should be employed utilising paracetamol, intravenous NSAIDs, topical LA and minimal opioid usage. A supplementary regional ophthalmic block is at the discretion of the team. As most patients experience pain for a median of three days (range one to nine days), 94 regular analgesia should be prescribed for three days after surgery.
Summary
General anaesthesia, the most commonly used technique, is suitable for patients of all ages, for complicated or repeated surgery and for bilateral eye procedures. The advantages of regional ophthalmic block include reduced incidence of OCR and emergence agitation, as well as providing postoperative analgesia. However, it requires cooperative patients as many experience discomfort especially during traction of the extraocular muscle and manipulation of conjunctiva. Topical anaesthesia has been used in pharmacological injection, minimally invasive surgery and uncomplicated conventional strabismus surgery. Furthermore, it facilitates the completion of adjustable suture strabismus surgery as a single-stage procedure. Its use, however, is only limited to cooperative adult patients.
Prophylactic antiemesis with ondansetron and dexamethasone combination is recommended, especially for children. A multimodal approach, including paracetamol, intravenous NSAIDs, topical LA and minimal opioid usage, is recommended for postoperative analgesia. A supplementary regional ophthalmic block is at the discretion of the team.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.