
Abstract
Transthoracic echocardiographic evaluation of the right ventricle is more difficult than the left ventricle and has not been well characterised in the parturient during delivery. As a preliminary investigation, our goal was to use bedside transthoracic echocardiography to evaluate right ventricular myocardial function before and after caesarean delivery. Term parturients undergoing caesarean delivery under spinal anaesthesia were enrolled. Echocardiography was performed pre- and postoperatively. Assessment of myocardial function included longitudinal myocardial strain using 2D-speckle tracking for both ventricles, and fractional area change for the right ventricle. Troponin-T, creatine kinase-muscle/brain and brain natriuretic peptide were measured pre- and postoperatively. One hundred patients were enrolled; 98 completed the study. Adequate images from both timepoints (pre- and postoperatively) were obtained in 85 patients for left ventricle assessment, and 66 for the right ventricle. Right ventricular fractional area change (mean (standard deviation)) (24.9% (8.9%) to 24.9% (9.2%); P = 0.99) and strain (−19.7% (6.8%) to −18.1% (6.5%); P = 0.08) measurements suggested mild baseline dysfunction and did not change after delivery. Left ventricular strain values were normal and unchanged after delivery (−23.8% (7.4%) to −24.3% (6.7%); P = 0.51). One patient had elevated troponin-T and demonstrated worse biventricular function. Elevation of brain natriuretic peptide (n=7) was associated with mildly decreased left ventricular strain, but creatine kinase-muscle/brain (n=4) was not associated with consistent changes in cardiac function. Further investigations into peripartum right ventricular function are required to validate the findings in this preliminary study. Findings of baseline mild right ventricular dysfunction and functional changes associated with troponin-T and brain natriuretic peptide warrant rigorous investigation.
Introduction
The peripartum period results in rapid and significant haemodynamic changes, such that even previously healthy parturients might demonstrate changes in myocardial function, potentially with myocardial stress or injury. Signs of potential myocardial injury such as new onset ST-segment changes on electrocardiography (ECG), 1 and elevations of cardiac biomarkers, 2 have been identified after delivery. The clinical consequences of these findings remain unclear,3,4 with previous studies primarily focusing on the left ventricle (LV) to determine a cause. 5
We theorised that signs of cardiac injury, such as ST-segment changes or elevations in cardiac biomarkers, may be due to right ventricular (RV) stress from supply–demand imbalance due to rapidly increased loading conditions that occur at the time of delivery. Unfortunately, RV function in the parturient is not well described in the literature, and virtually no data have been collected during the period of clinical care when the physiological changes occur. RV function can be challenging to measure due to the geometric configuration and thin walls. 6 Additionally, unlike the LV, the contraction of the RV is not concentric, making observation of ejection fraction a less reliable indicator of RV function. 7 The gold standard measure of RV function, cardiac magnetic resonance imaging, is expensive, time consuming, and cannot be easily used in the perioperative clinical setting. Changes in myocardial function may be transient during this period and would benefit from real-time imaging.
Transthoracic echocardiography (TTE) provides a number of modalities to assess right ventricular function.8,9 Laboratory assessment of RV function using TTE can achieve results that correlate well with magnetic resonance imaging, 7 and we hypothesised that bedside TTE might capture the physiological changes associated with delivery. The aims of this study were: (a) quantifying RV myocardial function during clinical care using bedside TTE; (b) and collecting biomarkers of myocardial injury to determine whether there is any association with TTE measures of RV function.
Methods
This prospective, longitudinal cohort study was approved by the institutional review board (Committee for Clinical Investigations) at the Beth Israel Deaconess Medical Center, study #2015P000387. This study was supported internally by the Beth Israel Anesthesia Foundation and did not receive any external funding. This manuscript adheres to the applicable Equator guidelines (STROBE). The study was conducted from February 2016 to April 2017. Given the limited data available on the topic and exploratory nature of the investigation, no power analysis was performed, and an enrolment of 100 patients was chosen. Potential study subjects were identified via the daily schedule for planned caesarean delivery under spinal anaesthesia. All patients enrolled in the study signed written, informed consent, which included consent to future publication of any results including echo images. Consent was obtained on the day of procedure and prior to the scheduled caesarean delivery. Inclusion criteria were: 18 years of age or older, scheduled caesarean delivery, singleton, term pregnancy, and American Society of Anesthesiologists (ASA) physical status of 2 (the ASA now defines pregnancy as ASA 2). 10 Subjects were excluded if they had a body mass index >45 kg/m2, or a history of cardiac surgery, coronary artery disease, valvular heart disease, or renal failure.
Anaesthesia for caesarean delivery was performed using hyperbaric spinal 0.75% bupivacaine (11.25 mg) with fentanyl (25 µg) and preservative-free morphine (250 µg). All patients received an infusion of lactated Ringer’s solution as crystalloid, with a co-load during spinal placement of approximately 10 ml/kg. Spinal-induced hypotension was treated using phenylephrine (100 µg bolus) to maintain systolic blood pressure to within 20% of baseline, and ephedrine (5 to 10 mg) if the heart rate was less than 70/min. After delivery of the neonate, all patients received an infusion of oxytocin (20 Units in 1000 ml) at an initial rate of 20 Units/h, which would be reduced upon achieving adequate uterine tone. Additional uterotonics were administered based on the clinical situation.
Transthoracic echocardiography
We evaluated subjects using TTE Philips CX50, (Philips North America Corporation, Andover, MA, USA) at two discrete timepoints: in the holding area immediately prior to surgery, and in the recovery room, 1–2 h after surgery. The preoperative and postoperative examinations of the heart focused on ECG-gated parasternal long axis, parasternal short axis and apical four-chamber views. Due to the presence of the gravid uterus in this patient population, subcostal views were not obtained. All TTE images for any given subject were obtained by only one of the investigators (ADS or HY). Each of these investigators first underwent rigorous simulator-based training followed by clinical training demonstrating proficiency in the limited TTE image acquisition required for this analysis. Descriptions of this training have previously been reported. 11 Neither of the investigators obtaining TTE images had any concurrent clinical duties. Image quality sufficient for evaluation was defined as a view of the entire ventricle with clear delineation of endocardial borders. Images were analysed offline for myocardial strain and fractional area change using TomTec Software (TomTec Imaging Systems, Unterschleissheim, Germany) by a single investigator. TomTec is a vendor-independent computer program that allows for offline analysis of any echocardiographic images stored in DICOM format. RV speckle tracking was performed using the TomTec LV strain package, which has been validated for this use. 12
Fractional area change was performed by tracing the endocardial border of the RV in both systole and diastole. The program then performed the following calculation
Fractional Area Change (FAC)%
= (EDA – ESA) × EDA−1
where EDA is end-diastolic area and ESA is end-systolic area. For reference, in the non-pregnant population, values for the RV of >35% are considered normal, while 25%–35% represents mild abnormality, 18%–24% is moderately abnormal, and values less than 17% represent severe dysfunction.8,13 Of note, the cut-off values for severity of mild/moderate/severe vary somewhat by source.
Strain is a unitless measure of tissue deformation defined by the change in length during muscle contraction compared with baseline uncontracted length. 14 Speckle strain was performed using previously described methodology. 15 For this analysis, the endocardial borders were manually traced in the end-systolic frame. The TomTec software tracks the distance between speckles along the endocardium and myocardium throughout the cardiac cycle, then producing a global strain value. Global longitudinal speckle strain was calculated for both the RV and the LV. RV measurements were performed using the free wall alone, which is consistent with American Society of Echocardiography 2018 guidelines. 16
For reference, normal non-pregnant female LV longitudinal strain is approximately −16.4% (6.0%) (mean (standard deviation, SD)) 17 performed using 3D WM tracking software (Toshiba Medical Systems, Otawara, Japan) and RV strain is −27% (2%) 18 performed with Automated Functional Imaging (GE Healthcare, Chicago, IL, USA); however, these values differ slightly based on the software used for calculation, 19 as well as gender, age, body surface area and cardiac chamber size.
Cardiac biomarkers
Cardiac biomarkers, consisting of troponin-T, creatine kinase-muscle/brain (CK-MB) and brain natriuretic peptide (BNP), were obtained from patients immediately prior to surgery, and again approximately 4–6 h after surgery. The preoperative phlebotomy was performed during placement of the intravenous cannula for surgery, while the postoperative phlebotomy was timed with another routine collection, or drawn as an independent sample, as required. The normal values in our laboratory were:
CK-MB, 0–10 ng/ml Troponin-T, 0–0.01 ng/ml BNP, 0–178 pg/ml
Biomarker concentrations that were found to be above the normal range on the postoperative sample were identified and were classified as being elevated if the change was greater than 10% from the preoperative baseline value.
Statistical analysis
Data were evaluated for normality using the Kolmogorov–Smirnov test. Comparison of TTE variables from pre- and post-surgery was performed using a paired t-test or Wilcoxon test, as appropriate. Analysis of variance was used to compare the LV and RV strain measures based on postoperative biomarker elevation, with Tukey–Kramer’s correction for multiple measures. A P-value ≤0.05 was considered significant. Analysis was performed using NCSS 11 Statistical Software (2016), (NCSS, LLC. Kaysville, UT, USA, ncss.com/software/ncss).
Results
We enrolled 100 patients in our study; two (2%) patients were eliminated due to exclusion criteria discovered after enrolment. The baseline characteristics of the 98 patients in the study are described in Table 1. All patients had uncomplicated caesarean deliveries under spinal anaesthesia. Mean crystalloid administration was 2280 (SD 580) ml and there were no transfusions of blood products. Six patients received supplementary uterotonics: four received rectal misoprostol 1000 µg, and two intramuscular carboprost 250 µg.
Patient and obstetric characteristics.
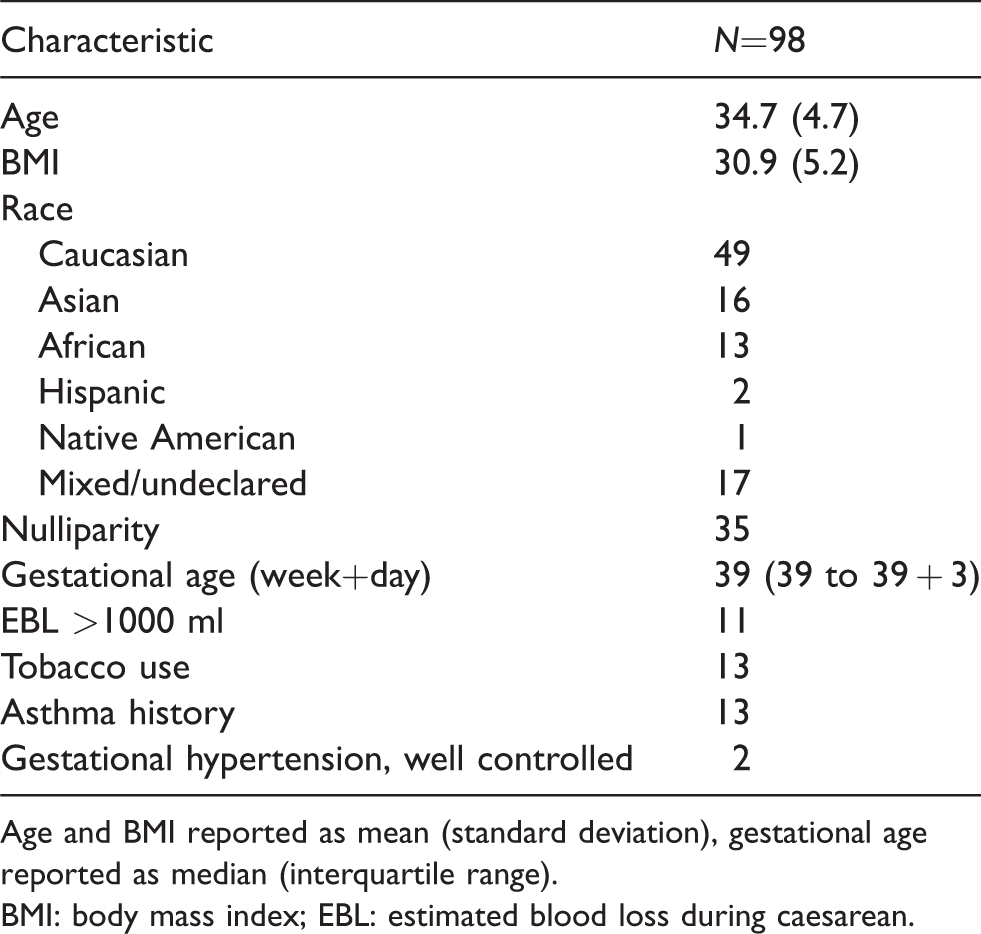
Age and BMI reported as mean (standard deviation), gestational age reported as median (interquartile range).
BMI: body mass index; EBL: estimated blood loss during caesarean.
The change in echocardiographic measures after delivery.
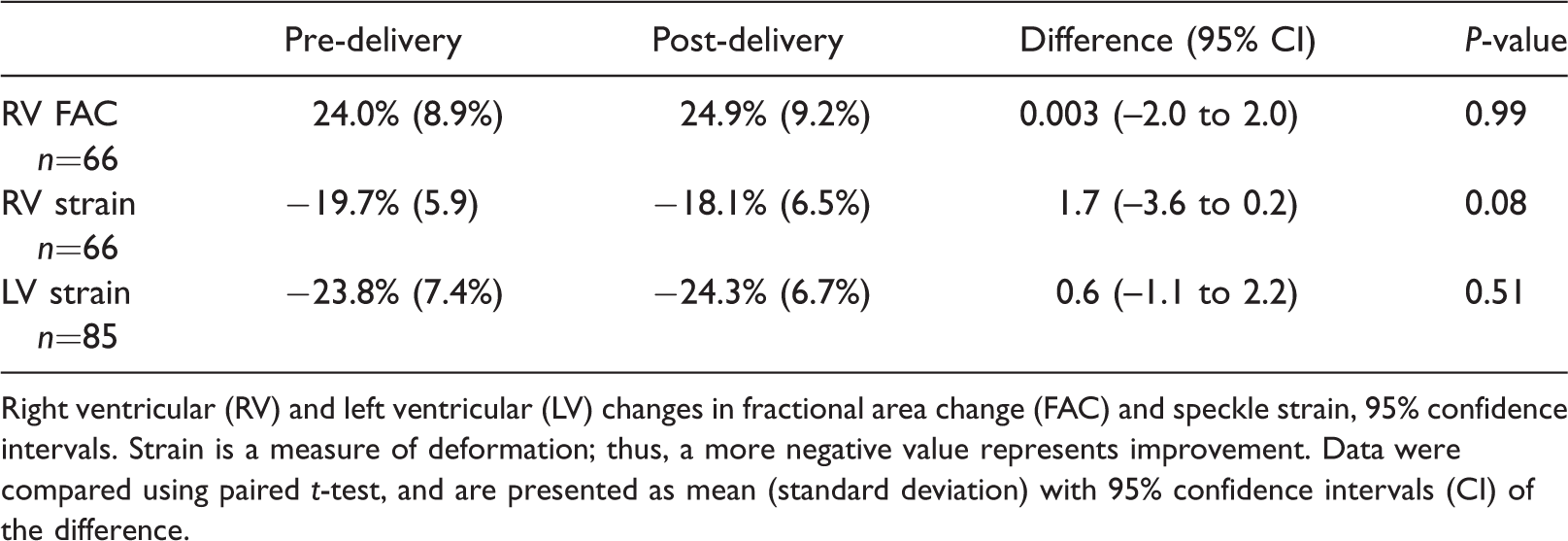
Right ventricular (RV) and left ventricular (LV) changes in fractional area change (FAC) and speckle strain, 95% confidence intervals. Strain is a measure of deformation; thus, a more negative value represents improvement. Data were compared using paired t-test, and are presented as mean (standard deviation) with 95% confidence intervals (CI) of the difference.
The change in ventricular function in patients with elevated biomarkers.
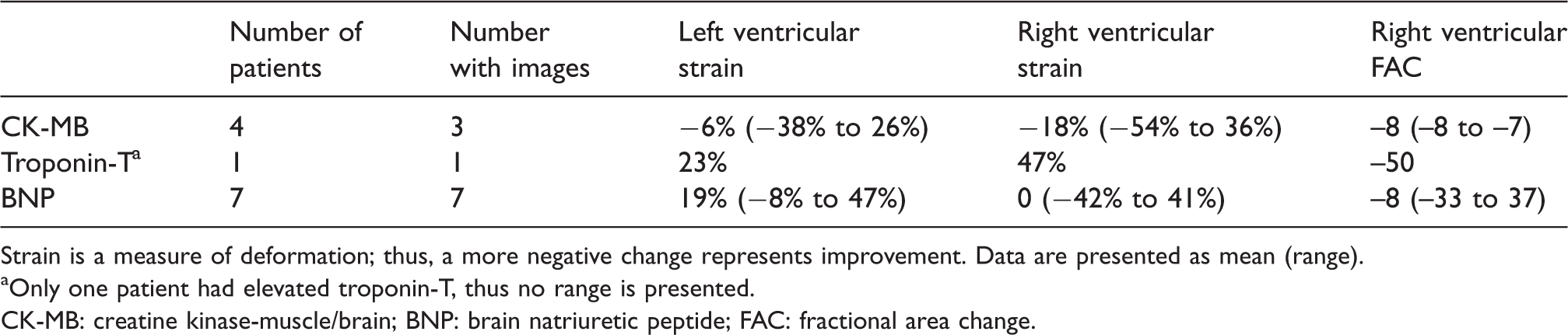
Strain is a measure of deformation; thus, a more negative change represents improvement. Data are presented as mean (range).
Only one patient had elevated troponin-T, thus no range is presented.
CK-MB: creatine kinase-muscle/brain; BNP: brain natriuretic peptide; FAC: fractional area change.
The description of elevations of biomarkers and TTE derived measures is found in Table 3. Five patients had elevation of their CK-MB (>10 ng/ml after surgery); however, one patient had the same value preoperatively and was not categorised as elevated, leaving four patients (4.1%). Seven patients had elevation of their BNP (>178 pg/ml) after surgery; one of these also had elevated CK-MB. Unfortunately, this patient had breast augmentation which made capturing adequate imagery for software analysis impossible. Patients with an elevated BNP had reduced LV strain (mean difference 5.9%, 95% CI of difference 0.8% to 11.0%; P-value=0.024) but not RV strain (mean difference –2.1%, 95% CI of difference –8.2% to 4.0%; P-value=0.49) compared with those with a normal BNP (P-value=0.04). Only one patient in our cohort had a postoperative elevation of troponin-T, and this patient had sizeable decreases in both LV and RV strain, as well as RV FAC (Table 3), but did not develop wall motion abnormalities; no statistics were examined as this was a single case. CK-MB was not associated with LV or RV changes (P-value=NS for both).
Discussion
The RV is likely to experience acute stress during childbirth as volume expansion occurs due to uterine autotransfusion, coupled with increased cardiac output; however, we could find minimal description of the RV function during parturition. In the absence of literature with which to conduct sample size estimates, we undertook an initial investigation to collect data that would inform further research into RV function during the peripartum period.
In this study, we identify that assessment of RV myocardial function with TTE in term pregnant patients in a real clinical setting is challenging, although not impossible. In agreement with prior investigators, we found that imaging windows and quality are often severely limited in this population, due to the complex shape of the RV, body habitus, patient positioning, and upward and anterior cardiac displacement by the gravid uterus.20,21 Our preoperative image capture was comparable to other investigations performed in the laboratory. 21 The inability to capture adequate quality images occurred primarily with the postoperative examination of the RV, in which the displacement of the heart resulted in preoperative and postoperative images that were significantly different. Furthermore, we were limited in the time available and in ability to optimise recordings due to the clinical situation. We did not find that patient body habitus impacted the postoperative image more than the preoperative exam, but patient discomfort from surgery did limit positioning. Taking these considerations into account, we believe that further research using real-time clinical evaluation is both possible and warranted.
Second, based on preliminary data, we found that both RV FAC and strain values were slightly depressed on average during the baseline evaluation. The LV, on the other hand, demonstrated baseline strain values above the average usually seen in non-pregnant patients. We hypothesise that both findings may represent the individual ventricular response to volume expansion that occurs during gestation and peaks just before delivery. Since these findings are based on our feasibility study, further investigation is warranted. The TTE-derived measures of myocardial function suggested that there was no change in ventricular function on average after caesarean delivery compared with pre-delivery values. As the vast majority of parturients have no clinical evidence of cardiac injury or symptoms, no change in myocardial function should be expected.
We found that two cardiac biomarkers might be useful for further investigation. If evidence of transient, subclinical myocardial stress or injury is to be found in this population, the use of sensitive biomarkers would likely be needed. Serum cardiac biomarkers can be useful in identifying myocardial ischaemia, injury, and infarction; however, these markers must be used with some caution in the parturient. Both troponin-I and troponin-T are biomarkers that can be found with myocardial injury, with the rise in troponin-T concentration in the serum appearing earlier than does troponin-I. 22 Cardiac troponins do not increase with labour and delivery, 23 and have been found to be elevated in 4% to 8% of patients undergoing caesarean delivery.5,24 We chose to measure troponin-T as this was readily available to us in our laboratory. We found only one patient with a postoperative elevation of troponin-T, and she had evidence of reduced LV and RV function compared with her baseline, as well as with non-pregnant normal values, without obvious wall motion abnormalities. As this was found in only one patient, we cannot draw a scientific conclusion.
We also measured BNP, which is a biomarker released with stretch of the ventricles, based on our hypothesis that postpartum volume expansion may exacerbate RV stress. Seven patients had elevation of their BNP postoperatively, demonstrating an apparent mild reduction in LV strain compared with those without, but without change in RV parameters. Our preliminary data suggest that volume expansion may not be the mechanism of RV injury in the healthy parturient without underlying heart disease, but further investigation into the finding of mildly reduced LV strain will be required.
CK-MB is frequently used to identify myocardial ischaemia but may not be the best choice for the parturient—especially those who undergo labour. CK-MB can be found in the placenta and the serum concentration increases during labour, but not necessarily with caesarean delivery.2,23,25 This likely explains why one patient in our study had a preoperative elevation of her CK-MB. Interestingly, the four patients in our study who had postoperative elevation of their CK-MB had minimal and inconsistent changes in LV and RV function.
We chose to conduct our study with two measures, FAC and strain, that may identify global RV function and subclinical myocardial dysfunction, respectively. FAC is a global measure of the longitudinal and radial components of contraction. FAC is a recommended volumetric method of quantitatively estimating RV function; it has been validated in adults, is a good predictor of cardiovascular morbidity, and correlates well with the gold standard, cardiac magnetic resonance imaging.7,9 Additionally, postpartum RV FAC has been found to predict recovery among patients with peripartum cardiomyopathy. 26 RV FAC has been criticised due to poor inter-observer reproducibility, 7 and further work would need to be performed to demonstrate intra- and inter-observer reliability in the clinical bedside setting, and to validate the results.
Echocardiographic speckle tracking analyses the degree of myocardial deformation, known as strain, throughout the cardiac cycle. Speckle tracking allows for the measurement of longitudinal, radial and circumferential strain and these can be used to evaluate ventricular function. 27 We limited our study to only longitudinal strain to improve the capture of patients. Strain is a sensitive marker of myocardial dysfunction, is angle independent, relatively load independent and not subject to large intra-observer variability. 26 Changes in LV and RV strain have identified subclinical systolic dysfunction in women with pre-eclampsia.15,21 Global RV longitudinal strain may be an objective measure of systolic function with clinical prognostic value. 28 We believe that if delivery were to be associated with a subclinical myocardial injury, it would most likely be identified by a reduction in strain.
Our study is subject to several limitations. Our findings are exploratory in nature and need to be considered with caution. Considering the LV parameters were as expected based on these prior studies, we believe that our finding of baseline mild RV dysfunction may represent a real signal, but more work is needed to define this. In a recent study using TTE in the peripartum period on healthy, pre-eclamptic and HIV positive parturients, Dennis et al. reported that 10% of healthy patients had depressed baseline LV function as measured by fractional shortening. 29 As well, this group reported on a variety of measures of RV function which were similar between groups but did not include RV FAC or RV strain. RV strain measurements may not be as accurate as those studied in the LV. 2D strain software was initially designed for measurements of the LV; the ventricles have different geometry, with the RV inflow and outflow tracts lying in separate planes. This limits the ability of the software to track the myocardial border especially when the imaging quality is poor, as was noted in the post-caesarean images. Strain values also vary amongst different software vendors; this makes comparison of data across studies difficult. Strain values were measured by one observer; this is a considerable limitation in our study as we do not know the degree of inter-observer reliability. Previously reported studies show good intra-observer reliability in the laboratory setting.17,19 Bedside TTE in the clinical environment is inherently more challenging and potentially fraught with errors that may not occur in the quiet setting of a laboratory. The degree of intra- and inter-observer reliability needs to be assessed in this setting. Because of the clinical situation, we only had time to capture longitudinal strain—radial or circumferential values may differ. The normal limits for the measure of FAC in these patients is unknown—we can find limited previous work to compare or to describe normal values in pregnancy. Elucidation of the baseline normal limits of each of these TTE measures in the term parturient would be necessary. We examined patients when available after surgery and given the dynamic changes in this period there may be a difference between exams done at 1 h versus 2 h. Finally, the incidence of elevations in cardiac biomarkers was below that expected from other studies in the literature. While this was beneficial for our patients, it limits evaluation of any potential association. A larger study is required to fully evaluate any associations.
In conclusion, our study demonstrates that it is difficult but possible to assess RV myocardial function using bedside TTE during clinical care. Based upon strain and FAC results these preliminary findings suggest that term mothers have mild RV dysfunction which is unchanged 2 h after caesarean delivery. Finally, we noted a potential association between subclinical myocardial depression and elevation of troponin-T and BNP.
Footnotes
Acknowledgements
Author contribution: AK: study design, manuscript preparation; AS: image acquisition, image interpretation, manuscript preparation; HY: image acquisition; PH: study design, data analysis, manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Beth Israel Anesthesia Foundation (internal funding).