
Abstract
Community harm associated with prescription opioids is causing global concern, and post-hospital discharge prescribing is contributing to the problem. We surveyed anaesthetists in Australia and New Zealand to determine which opioid stewardship measures are currently in place, and to gauge interest in participating in future health services research on introducing an opioid stewardship bundle of care. A total of 87 anaesthetists from 87 hospitals were invited to participate, and 45 (52%) responded. The extent of nine current opioid stewardship measures reported was highly variable. One respondent (2%) reported no measures introduced at their hospital; 12 (27%) one to two measures; 16 (36%) three or four measures; 13 (29%) five to seven measures; and 3 (7%), all nine measures were in place. Respondents were often interested in being contacted about future trial participation (n = 33, 73%); however, concerns regarding feasibility of introducing an opioid stewardship bundle of care were widespread (n = 22, 49%). It is possible that the variability in Australian and New Zealand opioid stewardship practice is due, in part, to the current limited evidence base for the individual measures, in addition to challenges in research translation. We have found that interest in further research on opioid stewardship is high. Comprehensive, locally adapted, evidence-based opioid stewardship measures may increase the safety of patients and the community following opioid therapy.
Introduction
Patient and community harm resulting from opioid use and misuse are undisputed. There is a high level of concern in the international community regarding the role of prescribed opioids in the total opioid burden. Post-hospital discharge, and more specifically post-surgical care, is emerging as an area of concern in the evolution of the opioid crisis, as inappropriate opioid prescription and use in this period is common.1–6 This complex problem requires a multifaceted solution.
The opioid crisis was initially recognised and has been best described in the United States.7,8 Whilst the factors relevant in the United States do not necessary apply directly to Australia and New Zealand, suboptimal opioid handling has been demonstrated in our region.9,10 Local measures are being developed at a national regulatory level, 11 and also at the individual health service or state level.12,13 However, current stewardship measures relating to prescribed opioids after surgical care across our region are unknown, and likely highly variable. To investigate the current situation, in anticipation of health services research around a bundle for opioid stewardship, we surveyed anaesthetists across Australia and New Zealand about current opioid management approaches. We also called for interest in participation in a clinical trial involving an opioid stewardship intervention, to gauge the feasibility of such an undertaking.
Methods
No existing survey tool was able to meet our study aims therefore we (MA, DS, KL and AP) developed a fit-for-purpose survey. We first produced a draft survey, then we simplified and shortened it to essential information only and ensured that the crucial questions were asked first. We then piloted the survey with three anaesthesia clinician researchers from selected local health services and requested feedback on any difficulties with comprehension and useability. No modifications were suggested by our pilot users and so our survey was finalised and used in our study (Appendix 1). 14 The survey consists of ten questions divided into four sections. We used a combination of yes/no, tick box and free text response options, with some questions requiring a response (Appendix 1). It was not possible to skip a question and continue the survey.
Our target population was anaesthetists who were engaged with the Australian and New Zealand College of Anaesthetists (ANZCA) Clinical Trials Network (CTN). Following ethics approval (MH QA 2018.116) the survey was distributed via email with a preamble introducing the investigators and detailing the research goals. Permission was obtained from the ANZCA CTN executive to utilise their researcher database and to perform the distribution. The database includes anaesthetists who had either attended the annual strategic workshop or had previously undertaken ANZCA CTN-endorsed research. This separation from the investigators allowed blinding to the recipients’ identities and ensured that responses were voluntary. Invitations were restricted to one researcher per hospital, selected by the ANZCA CTN, with the recipient having the option to delegate to a more suitable colleague. This strategy resulted in 87 invitations for participation being simultaneously sent (75 Australia and 12 New Zealand). Responses were submitted via a link to the REDCap electronic data capture tool hosted at The University of Melbourne. 15
Survey completion was accepted as inferred consent for the component exploring current institutional opioid practice. Explicit consent was sought for expression of interest in participation in a future study on an opioid stewardship intervention program. A reminder email was sent two weeks after the invitation. Two weeks after all invited anaesthetists had been sent their reminder, the available data were exported from the REDCap database and analysed in STATA version 12 (StataCorp. 2011. Stata Statistical Software: Release 12. College Station, TX, USA: StataCorp LP). Analysis consisted of descriptive statistics (counts, percentages). With 45 respondents from the identified target population of hospitals in Australia and New Zealand,16–20 the maximum half-width of a two-sided 95% confidence interval around a proportion is ±15% (Clopper–Pearson).
Results
Responses were received from 45 of the 87 recipients (52%) by survey close; 38 (51%) of the Australian anaesthetists and 7 (58%) of the New Zealand anaesthetists responded. The Australian respondents were from Victoria (n = 16; 42%); New South Wales (n = 11; 29%); Queensland (n = 5; 13%); Western Australia (n = 2; 5%), South Australia (n = 1; 3%) and Tasmania (n = 1; 3%). Most respondents (n = 38; 84%) were working in major public acute hospitals with a 24-h emergency department, intensive care facilities and a broad range of surgical specialties. The remainder were working at smaller public acute general hospitals (n = 6; 13%) or in private acute major hospitals (n = 1; 2%). We did not receive any responses from anaesthetists at specialist hospitals or private acute general hospitals. This distribution is supported by the reported number of operating theatres at the employing institution: 11 or greater (62%); six to ten (31%) and five or less (7%). All respondents reported having an acute pain service at their hospital.
Table 1 shows the opioid stewardship measures from the list in our survey instrument already introduced across the hospitals at which the respondents worked and how commonly these measures have been implemented in their region. Additional stewardship measures reported included routine conversion of patients on Oxycontin™ to Targin™ and restrictions on hydromorphone prescribing. The most commonly reported stewardship measures were analgesia adjunct co-prescribing (n = 40, 89%) and junior medical staff education (n = 35, 78%). Less than half of respondents reported that their hospital had a discharge opioid prescribing guideline including restricted opioid quantity unless approved by the acute pain service. The least commonly reported measures included routine communication with general practitioners about opioid prescribing at hospital discharge (n = 10, 22%) and advice to general practitioners about how to access assistance if they are having difficulty ceasing the prescribed opioids (n = 8, 18%). Three respondents (7%) reported having all surveyed measures of opioid stewardship in place and only one respondent (2%) reported that none of the measures were currently introduced at their hospital. Between these extremes, anaesthetists from 12 hospitals (27%) reported one or two measures were in place; those from 16 (36%) reported three or four measures; and those from 13 (29%) reported five to seven measures.
Number (%) of respondents by opioid stewardship component currently introduced in their hospital.
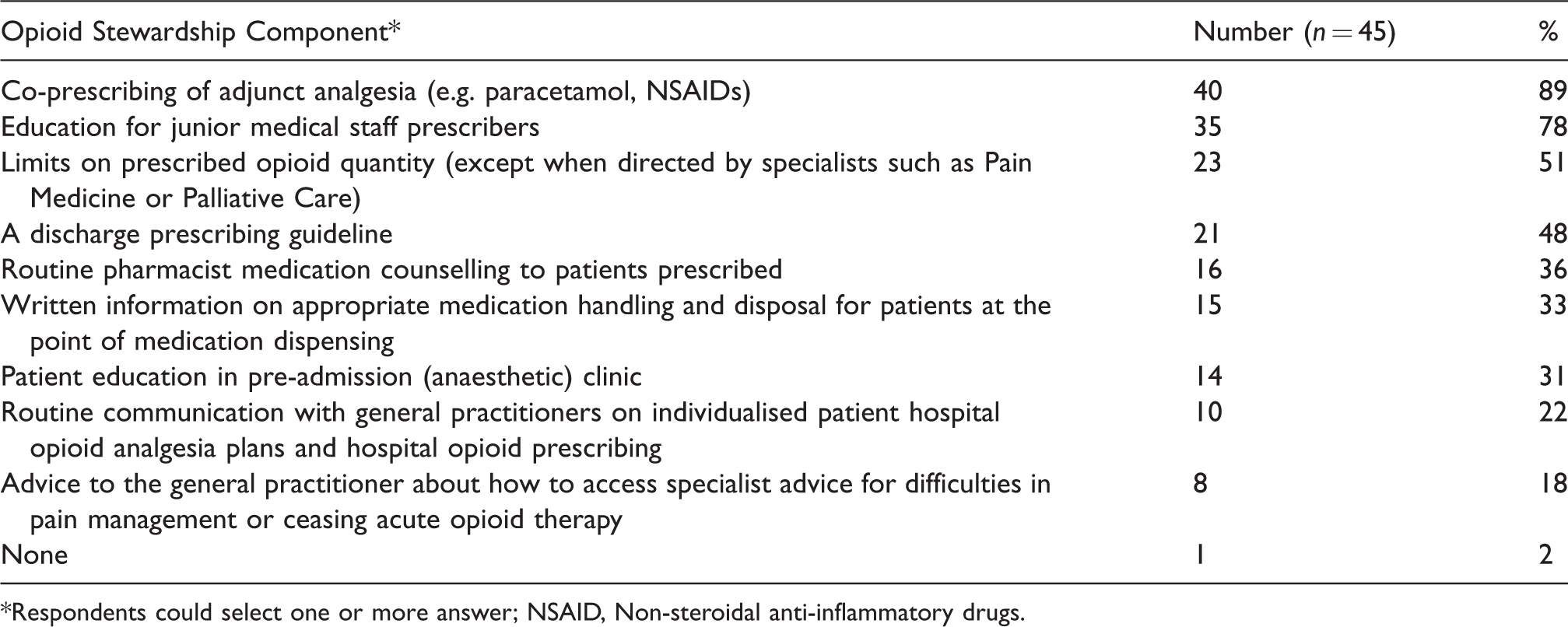
*Respondents could select one or more answer; NSAID, Non-steroidal anti-inflammatory drugs.
A high proportion of respondents (n = 33; 73%) were willing to be contacted about participating in future research involving the introduction of an opioid stewardship program. However, several concerns were reported. A total of 22 respondents (49%) raised resourcing as a major barrier that may be insurmountable in their hospital, even if there was trial funding available. One respondent had concerns that an opioid stewardship intervention may inadvertently result in patients receiving inadequate analgesia. Another reported that, in their practice, discharge prescribing is the remit of the surgeons and not an area in which anaesthetists could intervene; five (11%) reported a potential conflict of already having some stewardship measures or local guidelines in place in their hospital, but not a complete program.
Discussion
We conducted a survey of research active Australian and New Zealand anaesthetists on current practice and possible future research into opioid stewardship. Our results indicate that it is common for some measures to be in place to promote good practice in opioid prescribing, use and disposal following surgical care in hospitals in Australia and New Zealand. However, comprehensive programs were unusual and communication with general practitioners was poor.
In our study, the use of patient education brochures to guide disposal of surplus opioids was reported by only one-third of respondents. This is despite evidence that patient education can be effective.21,22 In one US study, 23 provision of simple written information significantly increased opioid disposal rates (22% vs 11% without information) in patients from two weeks to three months post-surgery. Whilst these rates remain low and the findings are from a small pilot study the results are encouraging for such a simple measure. Similarly, education of opioid prescribers, which was a common component of opioid stewardship in our study, is associated with reducing prescribed opioid quantities. 23
Guidelines were in place in just under half of the hospitals whose anaesthetists responded to our survey, and having such a guideline may be associated with reducing opioid prescribing. 24 In a single-centre US study, the quantity of opioids prescribed was reduced without any increase in reported pain scores or increased requests for repeat opioid prescriptions after guideline introduction and education. 24 However, the total prescribed opioid dose was significantly greater than Australian practice, 9 and so investigation of whether this approach translates into our region would be interesting.
Opioid stewardship programs are relatively new so the evidence base for the included measures is incomplete and local acceptability is unknown. The structure of the US health care system is such that surgeons undertake proportionally more of the total opioid prescribing and family physicians a smaller percentage compared with Australian practice.25,26 Of note, this is total opioid prescribing, not specifically perioperative opioid prescribing. Australia and New Zealand have strong primary health care systems with general practitioners as the cornerstone. This presents an opportunity in Australia and New Zealand to investigate the role of collaboration with general practitioners to manage post-discharge opioid therapy, and liaison options when cessation of therapy is problematic.
Despite responsible post-surgical opioid management being an important area to investigate, many respondents in this study cited logistic and resource barriers to future study participation. Bundle-of-care interventions, such as opioid stewardship programs, are particularly challenging to implement and assess. This is because they involve multiple adjustments to routine care, and supersede established institutional practices rather than targeting a single intervention such as occurs in clinical trials. Assessment of efficacy is challenging as such programs are also subject to shifts in standard care over time. Assessment of opioid stewardship programs within a quality assurance framework with repeated audit cycles would be ideal if the barriers could be overcome.
Strengths of our study include the use of a targeted and piloted instrument and a good response rate. 14 It revealed that opioid stewardship programs in the hospitals at which our respondents work are common, but the components vary.
The general limitations of survey research (non-response bias, voluntary response bias and unrepresentativeness) may apply to this study. Mitigating factors include the strong response rate and survey distribution determination by the ANZCA Clinical Trials Network as the regional peak research body. A further limitation is that current stewardship measures were reported by respondents without objective verification of actual practice. Additionally, only one (2%) respondent was answering on behalf of the private sector with the remainder working in public hospitals. Private hospital practice could possibly be closer to the American system, where the surgeon or perioperative physician prescribe discharge opioids, rather than anaesthetists or junior medical staff with access to acute pain service expertise. However, the true state of opioid stewardship in the private hospital sector in Australia and New Zealand remains undetermined and warrants further investigation.
It is possible that the variability in Australian and New Zealand opioid stewardship practice is in part because of the current limited evidence base for the individual measures, in addition to challenges in research translation. Whatever the reasons, current opioid stewardship practice across Australia and New Zealand is non-standard and likely suboptimal. We have found that interest in further research on opioid stewardship is high. We plan further investigations, including a feasibility study of an opioid stewardship bundle of care for post-surgical patients. Comprehensive, locally adapted, evidence-based opioid stewardship measures may increase the safety of patients and the community following opioid therapy.
Supplemental Material
AIC880904 Supplemental material - Supplemental material for Post-surgical opioid stewardship programs across Australia and New Zealand: Current situation and future directions
Supplemental material, AIC880904 Supplemental material for Post-surgical opioid stewardship programs across Australia and New Zealand: Current situation and future directions by Megan L Allen, Kate Leslie, Anna V Parker, Charles C Kim, Sally L Brooks, Sabine Braat, Stephan A Schug and David A Story in Anaesthesia and Intensive Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.