
Abstract
I describe a case and brief discussion to illustrate the clinical utility of transcranial Doppler ultrasound in suspected posterior reversible encephalopathy syndrome. A 26-year-old female presented with headache, visual disturbance, dyspnoea and hypertension. Past medical history included heart transplantation and hypertension. Cytomegalovirus pneumonia with acute respiratory distress syndrome was diagnosed requiring mechanical ventilation and extracorporeal membrane oxygenation. A brain computed tomographic scan showed changes suggestive of posterior reversible encephalopathy syndrome. Transcranial Doppler showed increased velocities with low pulsatility index consistent with cerebral hyperaemia. After antihypertensive treatment flow velocities and computed tomography normalised with complete clinical recovery.
Keywords
Background
Cerebral blood flow autoregulation maintains a constant blood flow over a range of systemic blood pressure by means of arteriolar constriction and dilatation. If an increase in systemic blood pressure exceeds the upper limit of autoregulation, arterioles dilate and cerebral blood flow increases in a pressure-passive manner. The resulting brain “hyperaemia” may lead to posterior reversible encephalopathy syndrome (PRES) with breakdown of the blood–brain barrier allowing vasogenic oedema, and extravasation of fluid and blood products into the brain parenchyma.2,3
Alternatively it has been postulated that reactive focal vasoconstriction leads to cerebral hypoperfusion and cytotoxic oedema. 3 However, ischaemia is not believed to play the major pathophysiological role in most patients with PRES. 3 A wide variety of medical conditions have been implicated as causes of PRES including hypertension, immunosuppressive therapy, renal disease, eclampsia, transplantation, autoimmune disorders and sepsis, etc.2,3 Clinical manifestations of PRES such as confusion, seizures, headache and visual disturbance are non-specific.2–5 Brain computed tomography (CT) or magnetic resonance imaging (MRI) can be used to exclude an alternative cause for the symptoms, but may not be diagnostic.1–3 The smooth control of high blood pressure and addressing the underlying cause usually results in complete recovery from PRES.2,3
Transcranial Doppler (TCD) can be used to measure blood flow velocity in the basal arteries of the brain.6–8 The flow velocity waveform obtained has a characteristic shape that can be used to differentiate between cerebral hyperaemia and hypoperfusion due either to reduced or elevated downstream resistance, respectively. The specific parameters obtained from the analysis of TCD flow velocity waveform include peak systolic velocity (Vs), end-diastolic velocity (Vd), time-averaged mean velocity (TAV Mean), pulsatility index (PI) and resistive index (RI). 8 Increased cerebral blood flow due to loss of cerebral arteriolar tone results in specific changes in TCD velocity waveform including increased Vs, Vd, TAV Mean, and decreased PI and RI. In contrast, cerebral hypoperfusion due to either high cerebrovascular resistance, or high intracranial pressure, leads to reduced diastolic and mean velocities, and a high PI. 7 Intracranial cerebral artery vasospasm can also cause increased velocities, but may be differentiated from hyperaemia by calculating the Lindegaard ratio, which is the ratio of mean velocity of middle cerebral artery (MCA) to mean velocity of ipsilateral extracranial internal carotid artery flow. 9 Elevated flow velocities with a Lindegaard ratio of less than 3 are suggestive of hyperaemia. Thus TCD may provide valuable diagnostic information in cases where other brain imaging has been inconclusive. Also TCD may be used to monitor the cerebral blood flow response to antihypertensive therapy.
Case presentation
A 26-year-old female presented to the hospital with acute-onset headache, blurring of vision, shortness of breath and labile hypertension. Her past medical history included a heart transplant for idiopathic restrictive cardiomyopathy ten years earlier, a second heart transplant for chronic rejection seven years later, labile hypertension, and hypertensive nephropathy with nephrotic range proteinuria. Her medications included mycophenolate, tacrolimus, prednisolone, everolimus, prazosin and lercanidipine.
She was admitted to the intensive care unit with worsening respiratory failure secondary to cytomegalovirus (CMV) pneumonia and CMV viraemia. Quantitative blood CMV polymerase chain reaction analysis revealed more than 8 × 106 copies per ml. An ophthalmologic examination showed hypertensive changes. The patient was intubated and ventilated for severe acute respiratory distress syndrome with extensive bilateral infiltrates on chest radiograph and required continuous renal replacement therapy (CRRT) for acute on chronic kidney disease. Veno-venous extracorporeal membrane oxygenation (ECMO) was commenced when hypoxia was refractory to lung protective ventilation. The patient had persistently elevated blood pressure ranging from 180 to 220 mmHg systolic despite oral and intravenous antihypertensive medication. A TCD ultrasound examination was performed on the day ECMO was commenced (Day 0) and serially for the next three days. A brain CT scan was performed on the day ECMO was commenced and three days later (Day 3).
Transcranial Doppler imaging
The TCD was performed using a commercially available ultrasound machine with a 2 MHz phased array probe (General Electric Vivid S70N, Horten, Norway) placed over the acoustic temporal window for insonation of the M1/M2 section of the MCA at a depth ranging from 45 to 55 mm. The measurements were obtained from the right MCA, although both MCAs were insonated and showed similar values. The spectral Doppler showed markedly elevated blood flow velocities and reduced pulsatility and resistive indices on day 0. Serial TCDs were performed to track changes in MCA blood flow velocities with institution of antihypertensive therapy including sodium nitroprusside and labetalol infusion (Table 1). Blood pressure was maintained within a range of 140–160 mmHg systolic.
Transcranial Doppler right middle cerebral artery blood flow velocities.
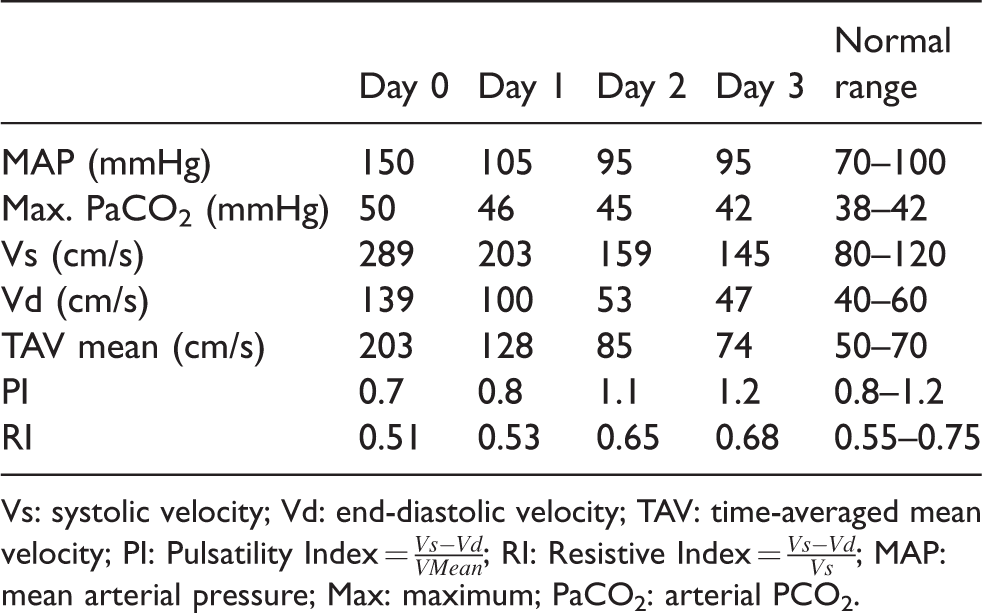
Vs: systolic velocity; Vd: end-diastolic velocity; TAV: time-averaged mean velocity; PI: Pulsatility Index =
Radiological findings and response to treatment
The initial CT brain revealed a hypodense lesion in the left occipital lobe, small-volume extra-axial bleed in the right frontal lobe and effacement of sulci (CT Day 0, Figure 1(a–d)), findings suggestive of PRES. A follow-up CT brain three days later (CT Day 3, Figure 2(a–d)) revealed prominent sulci and near complete resolution of occipital lobe hypodensity, reflecting reversibility of the pathology consistent with the diagnosis of PRES. On day 0, right MCA TCD showed significantly increased systolic, diastolic and mean velocities with reduced PI indicating presence of marked cerebral hyperaemia. The Lindegaard ratio was less than 3, showing absence of vasospasm. Serial TCD examinations (TCD images, Figure 3 (a–d)) revealed a gradual decrease in Vs, Vd and TAV mean velocities and a rise in PI and RI over a period of four days (Table 1). The TCD performed on Day 3 revealed near normal values of flow velocities, and PI and RI. The right posterior cerebral artery (PCA) was visible, but due to a poor angle of insonation we could not accurately estimate the velocities. However, the vessel showed a mosaic pattern of colour even at colour velocity scale of 63 cm/s that indicated increased flow velocities. The basilar and vertebral vessels could not be examined because of difficulty in positioning the head while patient had an ECMO return cannula in the right internal jugular vein.
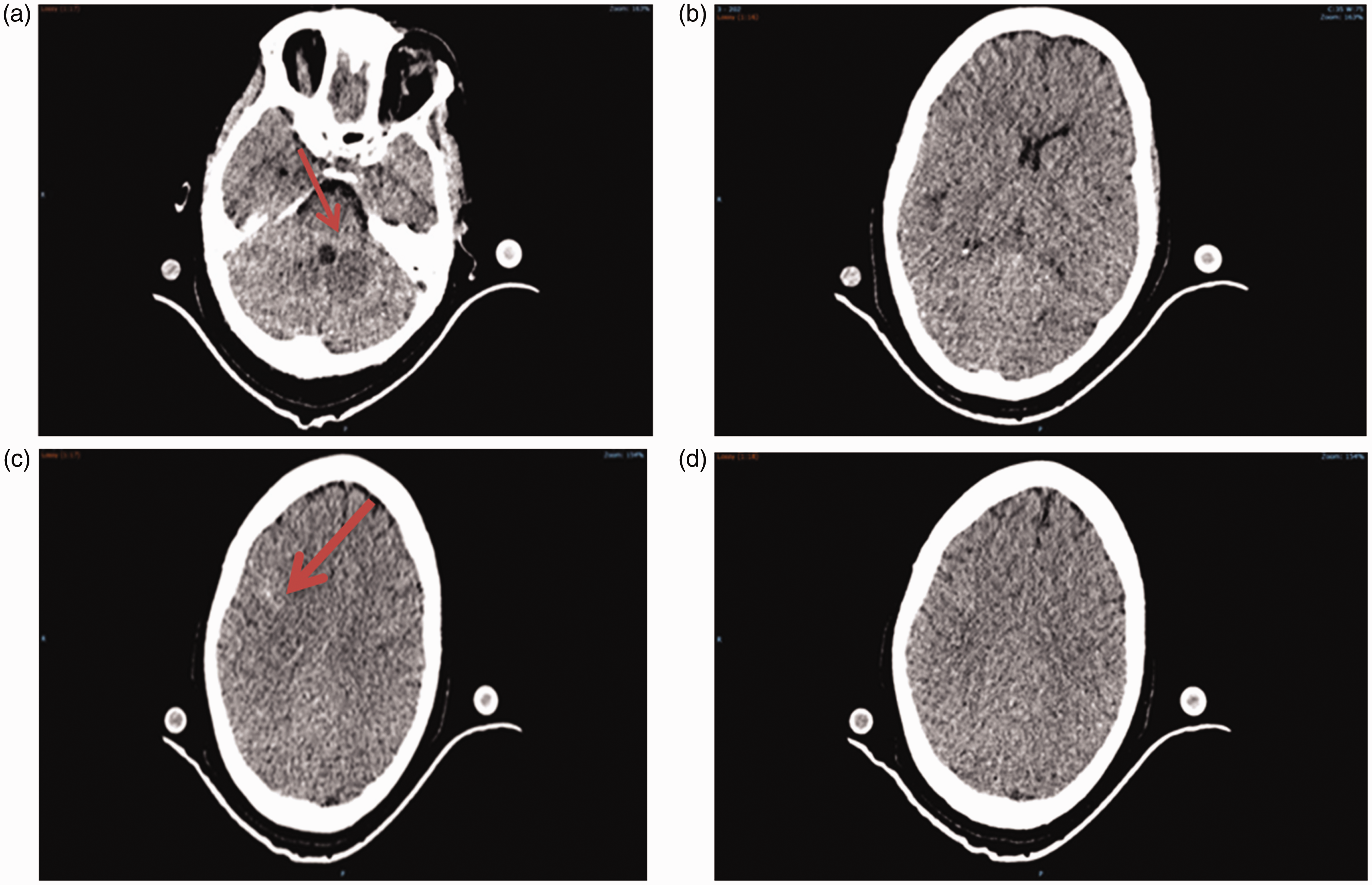
CT (Day 0) showing left occipital lobe hypoattenuation, right frontal lobe extra-axial haemorrhage and effacement of sulci.
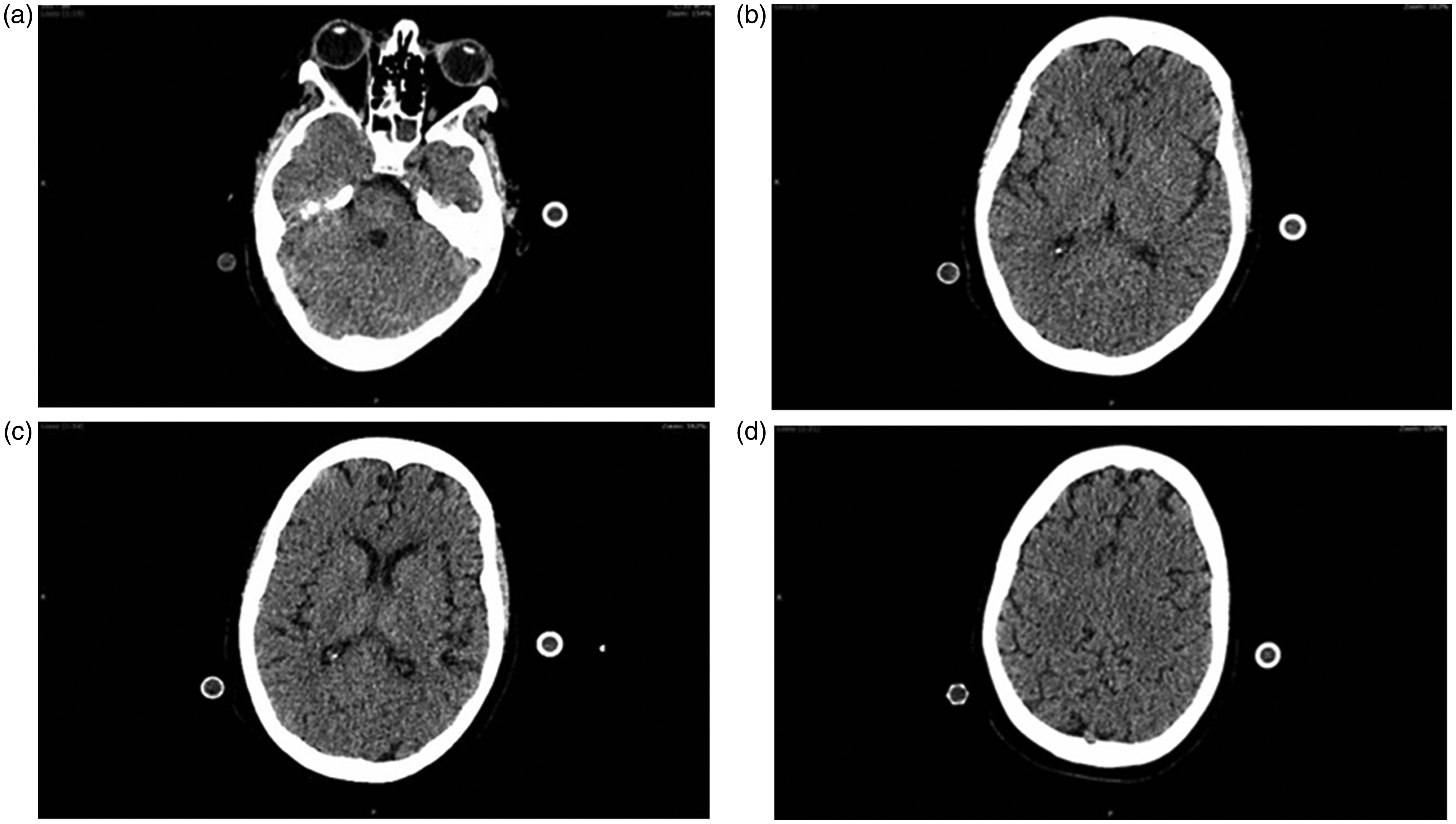
CT (Day 3) showing resolution of occipital hypoattenuation with prominent sulci following control of hypertension.
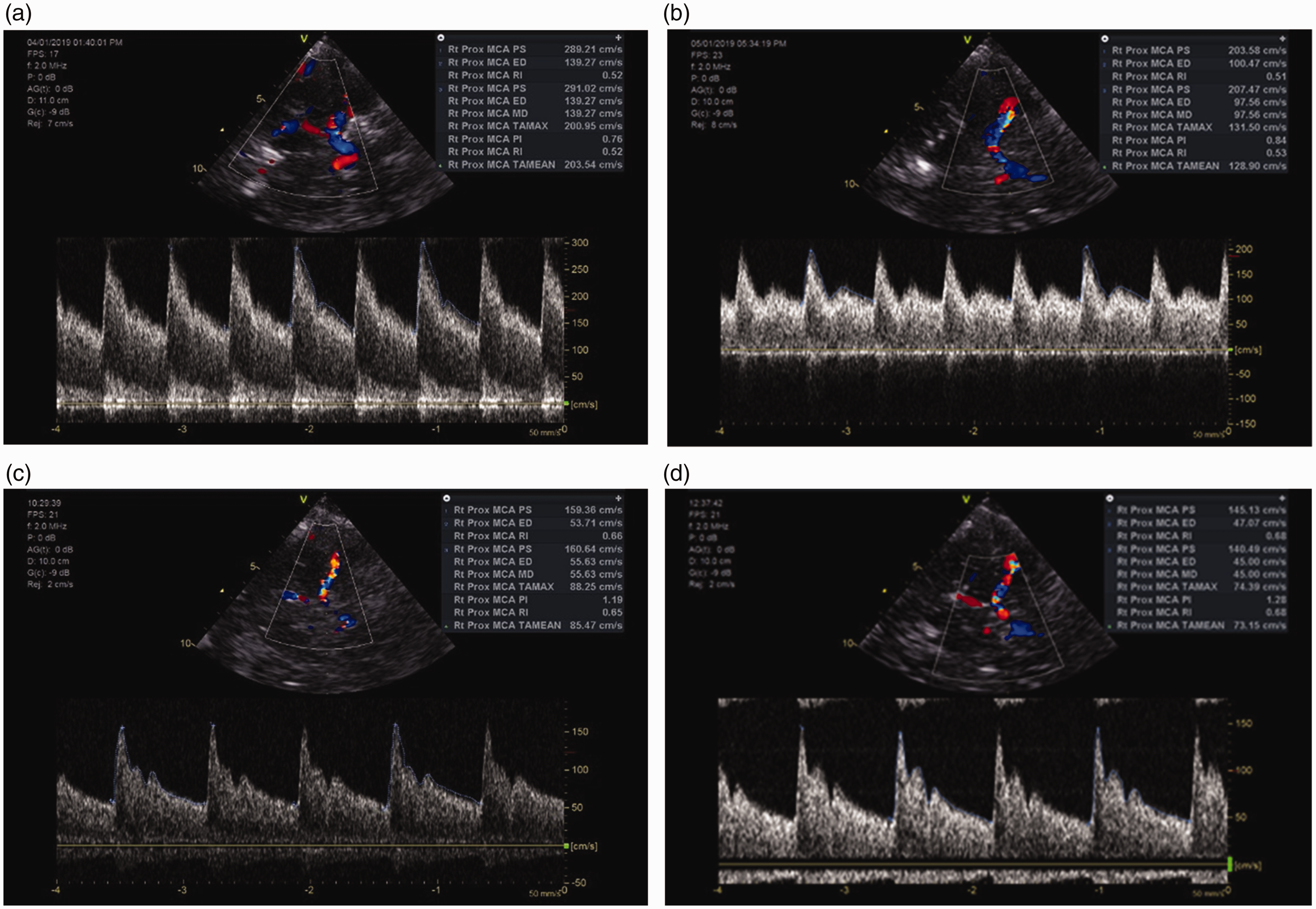
TCD images. (a) TCD Image 1 (Day 0). Significantly elevated Vs, Vd, TAV mean velocities and reduced PI indicating cerebral hyperaemia; (b) TCD Image 2 (Day 1). Decreased velocities and a decreasing PI compared with previous day’s values; (c) TCD Image 3 (Day 2). Markedly decreased flow velocities and PI after 48 hours of antihypertensive therapy; (d) TCD Image 4 (Day 3). Normal flow velocity envelope. The values of Vs, Vd, TAVmean and PI are within normal range. TCD: transcranial Doppler; Vs: peak systolic velocity; Vd: end-diastolic velocity; TAV mean: time-averaged mean velocity; PI: pulsatility index.
Discussion
In this patient, the symptoms and clinical context raised suspicion of PRES. The CT brain showed changes consistent with but not diagnostic of PRES. The patient became clinically inaccessible to neurological examination because of the severity of her respiratory failure, and a brain MRI was not possible because of the intravenous wire reinforced ECMO cannulae. The resolution of cerebral oedema and hypodensities with blood pressure control strongly favoured the diagnosis of PRES. In this case the TCD changes, which improved with antihypertensive therapy, proved valuable in the diagnosis of PRES and monitoring the response to therapy. A state of cerebral hyperaemia explains the mechanism of cerebral oedema in this case and it may also indicate that intracranial pressure was not high enough to cause cerebral hypoperfusion.
PRES is mostly a posterior circulation problem; however, involvement of carotid territory has been reported. Patients with PRES can be divided into two groups: (a) exclusively in posterior zones; and (b) anterior plus posterior zones or exclusively anterior zones. 10 Patient falls in the second group, and radiological findings were consistent with generalised cerebral oedema, and a small haemorrhage and a hypodensity in the MCA and PCA territories, respectively. TCD showed evidence of increased flow velocities in both MCA and PCA.
The patient had severe sepsis and mild hypercapnia before and after initiation of ECMO, and one may consider a systemic vasodilatory state with hypercapnia to be a cause of cerebral hyperperfusion. However, the evidence suggests that cerebral microcirculation alterations related to sepsis are characterised by a decrease in the density of perfused microvessels and decrease in the density of perfused microvessels would cause an increase in cerebrovascular resistance. 11 The PI, as an indicator of cerebrovascular resistance, has been found to be higher in septic patients, compared with normal controls. 12 Another study suggested presence of cerebral vasoconstriction in septic compared with non-septic patients. The pCO2 values were higher in septic patients (mean (standard deviation) 46 (12) versus 39 (4) mmHg, P < 0.01). No statistically significant higher values of MCA mean velocities were found in septic patients. Higher values of PI and RI were found in septic patients. 13
Conclusion
These findings suggest that PRES is a state of cerebral vasomotor paralysis leading to increased cerebral blood flow that can be assessed with TCD imaging. A patient presenting with neurological symptoms, severe hypertension, inconclusive brain imaging and cerebral hyperaemia on TCD should raise the suspicion of PRES. In addition, it may be difficult to make a diagnosis of PRES if the patient has only mild to moderate hypertension and a normal CT brain. In these patients, TCD may potentially show a low resistance velocity waveform and increased flow velocities to reflect loss of arteriolar resistance, and hence help in the diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
A verbal consent for the publication of this case report was obtained from the patient and next of kin.