
Abstract
Research on the nocebo effect has shown that some words can hurt. Pain is defined as ‘unpleasant’ and ‘associated with actual or potential tissue damage’. So, a sensation described as ‘pain’ may function as a negative suggestion or nocebo communication. This can lead to pain being experienced or exacerbated where it would not have been otherwise. The nocebo effect has also been implicated as adversely affecting the pain experience during the assessment of pain postoperatively. Words that avoid this potential nocebo effect such as ‘comfort’ may represent a more satisfactory alternative. We therefore aimed to determine whether ‘comfort’ and ‘pain’ scores correlate when assessing patients postoperatively at the same timepoint. Patients were questioned before routine post-anaesthesia rounds to rate their pain and comfort levels, with the sequence of questions randomised. Patients were asked to rate pain and comfort on a 0–10 verbal numerical rating scale, where 0 represents ‘no pain’ or ‘no comfort’ and 10 ‘worst pain’ or ‘most comfort’ imaginable, respectively. To provide a clinically relevant correlation of approximately 0.7 between pain and inverted comfort scores, a sample size of 100 would provide adequate precision (95% confidence interval (CI) 0.58–0.79). A P-value of <0.05 was considered significant. We recruited 100 patients. A positive correlation of 0.62 was found between pain and inverted comfort scores (95% CI 0.47–0.72; P<0.0001). The question sequence of asking about pain or comfort did not affect either score. Comfort and pain scores are moderately correlated. This finding represents a first step in validating comfort scores and suggests that they could be considered a suitable alternative to pain scores when assessing patients postoperatively. As comfort is not an exact antonym to pain, caution is required when using these measures interchangeably.
Keywords
Introduction
Research on the nocebo effect has shown that some words can hurt 1 whilst others can help. 2 The use of negative suggestions (nocebo communications) when delivering healthcare interventions (e.g. ‘this will sting’ when injecting local anaesthetic) can increase patient anxiety and pain.1,3–5 The term ‘nocebo’ is often used interchangeably with ‘negative suggestion’ to describe a verbal or non-verbal cue that has the potential to lead to a subconscious patient response, resulting in a negative perceptual experience.6–9 Advances in neuroimaging indicate that nocebo communications are associated with increased anterior cingulate activity, suffering and pain exacerbation.10,11 Such negative suggestions also appear to be involved in cholecystokinin release.3,12
As the term ‘pain’ is defined by the International Association for the Study of Pain as always unpleasant and ‘associated with actual or potential tissue damage’, 13 sensations described as ‘pain’ to a patient may function as a negative suggestion or nocebo. 4 This phenomenon can lead to pain being experienced or exacerbated4,8where it would not have done so otherwise. The nocebo effect has also been implicated in adversely affecting the pain experience during the assessment of pain postoperatively, particularly with the repeated use of pain scores. 14 Words that avoid the potential nocebo effect of pain, such as ‘comfort’, when assessing patients’ recovery from surgery may avoid this phenomenon. In the context of postoperative sensations, some carers and patients might interpret these experiences as tissue damage following surgical trauma, whilst others might consider the same sensations as healing and recovery. In clinical practice, postoperative pain assessment typically involves the use of validated pain measures such as verbal numerical rating scores (VNRS) or the visual analogue scale (VAS). These pain-rating scales are considered well correlated with each other and valid for assessing the intensity of pain.15–17 In routine post-anaesthesia rounds at our institution, healthcare providers typically ask patients to rate their postoperative pain using the VNRS. However, using pain scores may be inadvertently communicating a negative suggestion that has the potential to affect the patient’s pain experience and recovery adversely. 18 When considering an alternative scoring system that avoids the use of the word ‘pain’, it would be important to determine whether the alternative measure correlated with pain. If such a correlation was found, the use of comfort rather than pain scores might still provide useful information about the postoperative experience in much the same way as pain scores do now but without the potential for nocebo effects. We therefore aimed to determine whether comfort scores correlate with pain scores when assessing patients postoperatively at the same timepoint.
Materials and methods
Following local Human Research Ethics Committee approval (LNR/17/Nepean/153), this study was conducted over a six-month period (1 January 2018 to 1 July 2018) in a large tertiary referral centre for surgical care in Western Sydney, Australia. Patients older than 18 years of age and scheduled to receive routine post-anaesthesia review were eligible for inclusion provided they had sufficient English language proficiency, were not cognitively impaired and had no history of chronic pain or opioid abuse.
We recruited a convenience sample of patients according to researcher availability. Written informed patient consent was obtained after the postoperative questioning was completed. Where consent was declined, responses were recorded in the case notes as per usual post-anaesthesia care and patient data excluded from further analyses and reporting.
Participants were assessed and interviewed by one of the researchers postoperatively (MWM) with the questions listed in Table 1. All participants had baseline demographic data recorded. The order in which the questions were administered (pain scores or comfort scores first) was randomised, and allocation occurred immediately prior to seeing the patient. The randomisation was by computer-generated random-number sequence and allocation concealment by consecutively numbered opaque sealed envelopes containing the sequence. Participants rated their pain on a 0- to 10-point VNRS, where 0 was ‘no pain’ and 10 ‘the worst pain imaginable’, and also their comfort, where 0 was ‘no comfort’ and 10 ‘the most comfortable’. Inverted comfort scores were measured and calculated as 10 minus the comfort score. Patients also rated their pain on an unmarked VAS of 0 to 100 mm, where 0 was ‘no pain’ and 100 mm ‘the worst pain imaginable’, and also their comfort, where 0 was no comfort and 100 mm ‘the most comfortable’. The VNRS was subsequently compared to the VAS using the Mann–Whitney U test, and a P-value of <0.05 was considered significant.
Interview questions of comfort and pain asked to all participants.
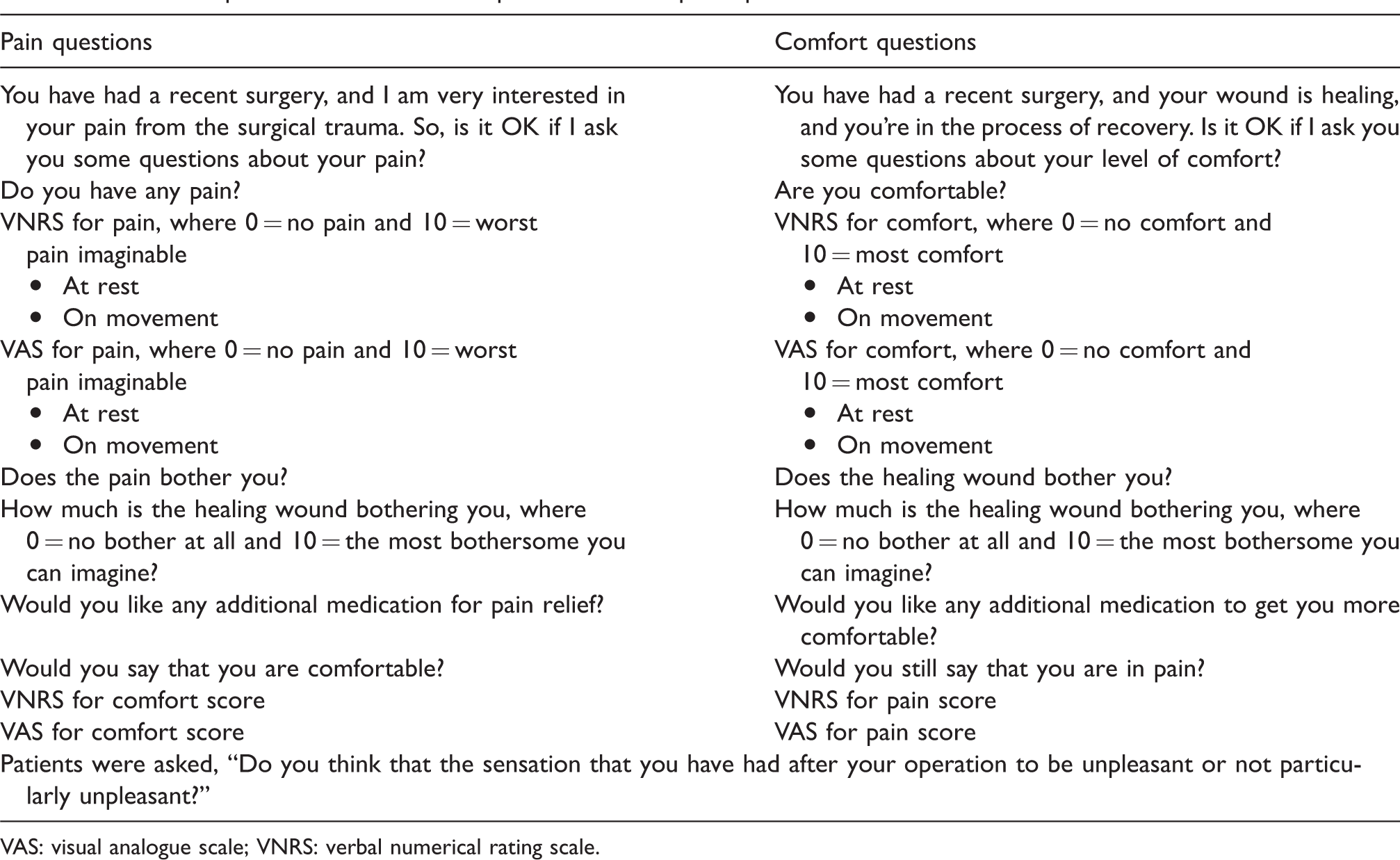
VAS: visual analogue scale; VNRS: verbal numerical rating scale.
Pain and inverted scores of comfort were also grouped into mild (1–4), moderate (5–7) and severe (8–10) categories, as used by previous pain assessment studies.19,20 These scores were compared to the sensation of the surgical wound being bothersome or unpleasant and the need for further analgesia, as shown in Table 4.
Data were collected about participants’ type of surgery, anaesthesia used, postoperative analgesia, the environment of the interview such as patient activity and other people present. All data were transcribed and stored electronically on a password-protected Microsoft Excel spreadsheet (Excel version 2013). The association between pain scores and inverted comfort scores was characterised using linear modelling and a Pearson correlation coefficient calculated. We assumed a clinically relevant correlation of 0.7 between pain and inverted comfort measures, and we targeted a sample size of 100 to provide adequate precision, with a 95% confidence interval (CI) of 0.58–0.79.
Results
We assessed 114 patients for eligibility, and 14 patients were excluded. Ten patients had insufficient English skills, and four had a history of chronic pain or opioid abuse. No patients subsequently withdrew from the study, and there were no losses to follow-up. Table 2 shows baseline characteristic data. The mean age of participants was 52 years (SD = 19.3 years). All patients were interviewed between 0 and 11 days postoperatively (median 2 days; interquartile range 1–3 days).
Baseline characteristic of patients.
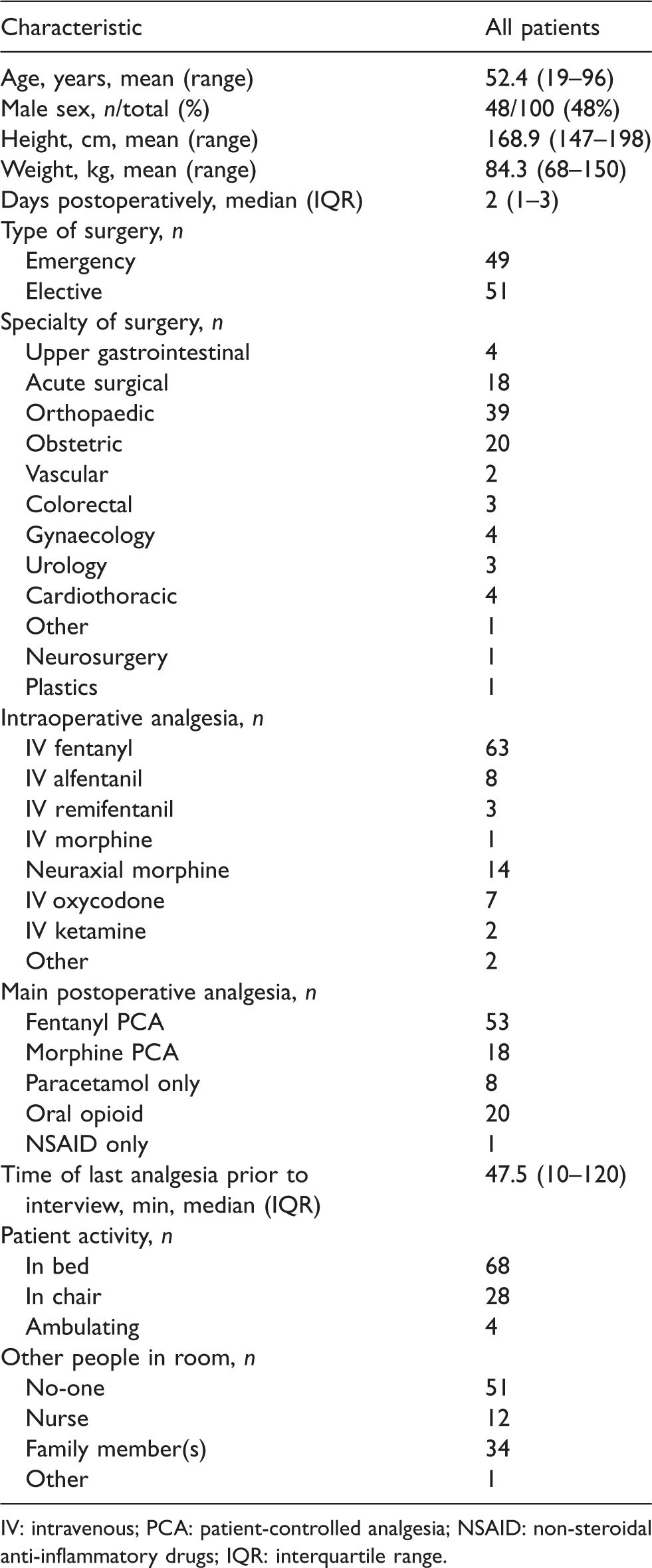
IV: intravenous; PCA: patient-controlled analgesia; NSAID: non-steroidal anti-inflammatory drugs; IQR: interquartile range.
The correlation of inverted comfort scores with pain scores postoperatively at rest are presented in Figure 1 with a regression line. The correlation between these measures was 0.62 (95% CI 0.47–0.72; P<0.0001). When patients were asked specifically, ‘Do you have pain?’, an equal number of patients reported pain, irrespective of whether pain or comfort were asked first. There was also no difference between any measure of pain, comfort, bothersome sensations or the need for analgesia. No differences in the VNRS or VAS of patients concerning the question sequence of either pain or comfort were found (Table 3).
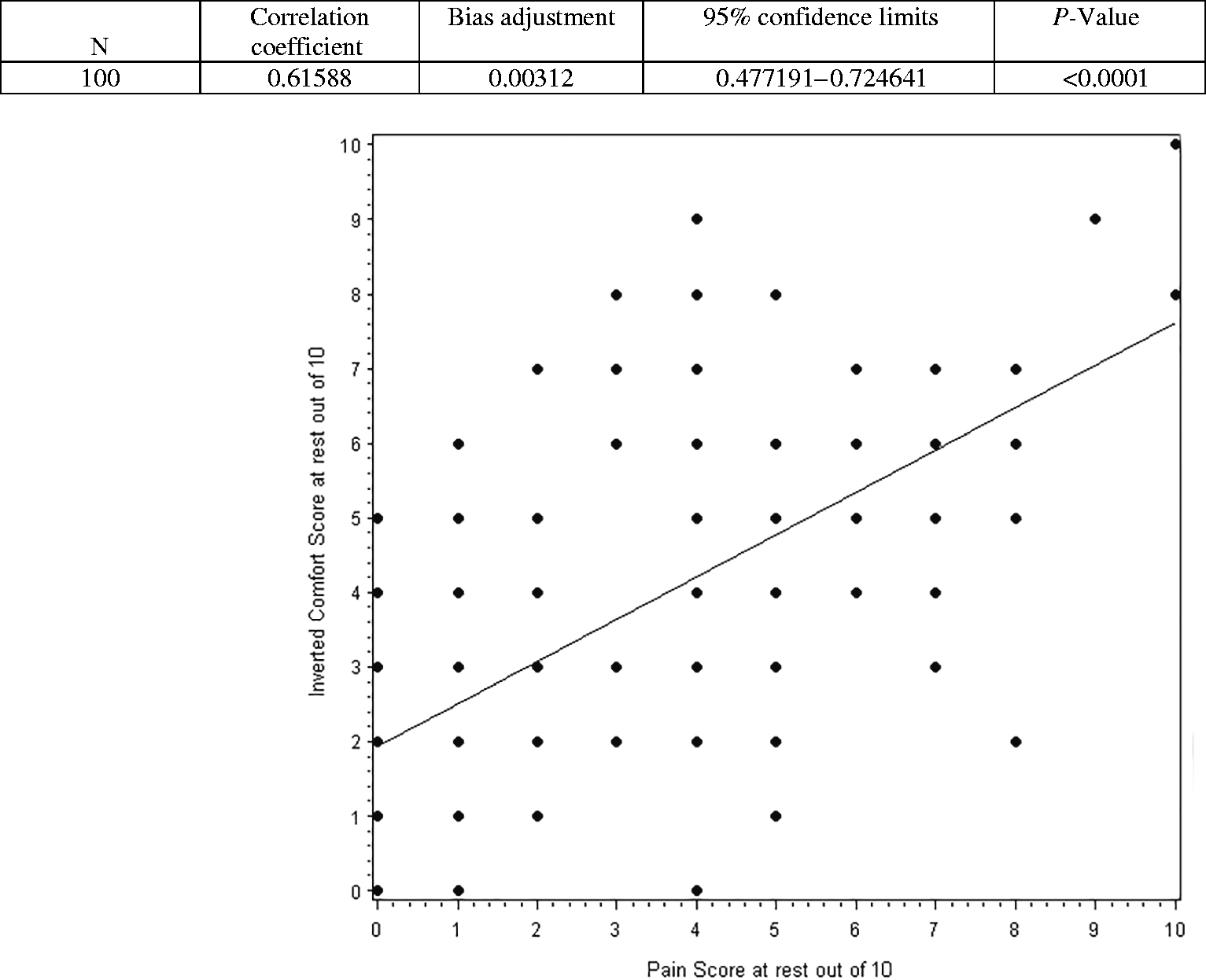
Inverted comfort scores compared to the pain scores of postoperative patients.
Verbal numerical rating scale and visual analogue scale according to question sequence: pain or comfort asked first.
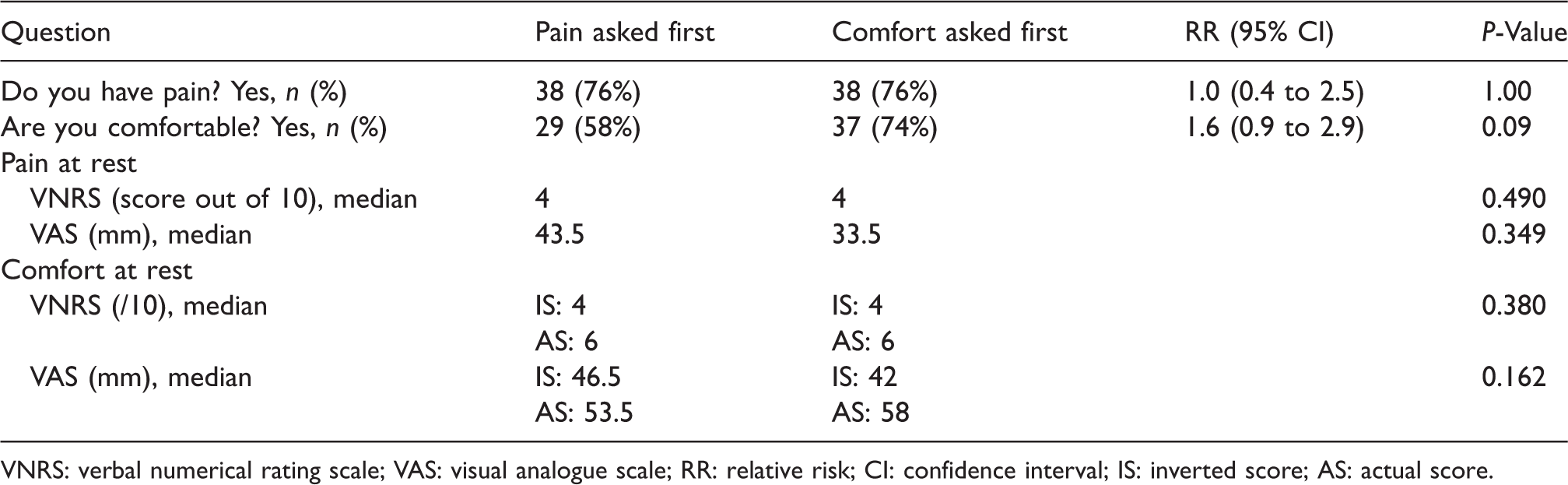
VNRS: verbal numerical rating scale; VAS: visual analogue scale; RR: relative risk; CI: confidence interval; IS: inverted score; AS: actual score.
Pain and comfort scores of patients compared to the surgical wound being reported as bothersome or unpleasant and the need for further analgesia.
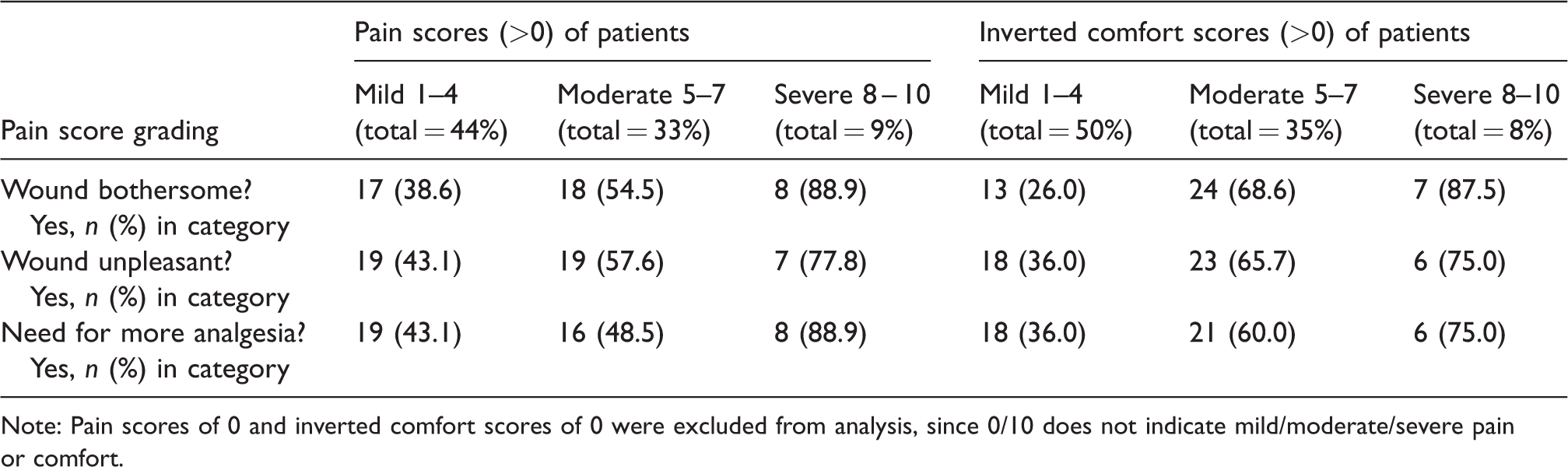
Note: Pain scores of 0 and inverted comfort scores of 0 were excluded from analysis, since 0/10 does not indicate mild/moderate/severe pain or comfort.
The pain and inverted comfort scores of patients, grouped into mild (1–4), moderate (5–7) and severe (8–10) categories, were also compared to the sensation of the surgical wound being bothersome or unpleasant and the need for further analgesia. As expected, a lower proportion of patients in the mild category found the wound bothersome or unpleasant or needed more analgesia. A higher proportion of patients in the severe category found the wound bothersome or unpleasant and requested more analgesia. This pattern was shown to be similar for both pain and comfort scores (Table 4). Interestingly, 40% of patients in the mild category of both inverted comfort and pain scores reported the postoperative experience as bothersome or requested analgesia. Similarly, 10% of patients scoring in the severe category reported that they were not bothered by pain or required no analgesia.
Discussion
The concept of nocebo communication affecting patient experience has only been reported in the medical literature for about 15 years 1 and in the anaesthesia literature for only five years. 18 Alternative measures of pain that might avoid inadvertent nocebo effects in adult patients have not been studied to date. The lack of studies investigating the effects of pain assessment on the pain experience likely reflects inadequate awareness amongst clinicians of the effects of negative suggestion or nocebo communication outside the psychology and hypnosis literature.1,21,22
The key finding of this study is that pain and comfort scores are moderately well correlated. This correlation was assumed in a previous randomised controlled trial where these assessment measures were examined in two groups of patients following caesarean section. 18
Our findings suggest that patients who are not expressing pain spontaneously could be asked about their comfort as part of their postoperative assessment. This approach has the advantage of avoiding the word ‘pain’ and its possible nocebo effects.1,3,4,9 Interestingly, the Academy of Family Physicians voted to drop pain scores as the ‘fifth vital sign’, suspecting that this measure was playing a role in the recent increase in postoperative opioid use. 23 This was also a finding consistent with that of Chooi et al., who found requests for analgesia decreased fourfold in the context of postoperative caesarean section pain when pain scores were avoided. 18 It appears likely that the use of comfort score assessments may represent a useful alternative measure postoperatively that would minimise the likelihood of negative patient perceptions and experiences being induced or exacerbated.14,18
There was no difference between the VNRS or VAS in terms of whether patients were asked first about either their pain or their comfort (Table 3). This suggests that the order of questioning about pain or comfort did not influence our findings of a correlation between pain and comfort scores.
Not surprisingly, a lower proportion of patients in the mild pain category, as shown in Table 4, found the wound bothersome or unpleasant or needed more analgesia compared to those patients with severe scores. Interestingly, irrespective of whether patients were asked about their pain or comfort first, several patients in the mild pain category found the sensations bothersome or requested analgesia (Table 4). Similarly, one patient in the severe pain category did not want analgesia, and one did not find the sensations bothersome, suggesting that pain scores cannot be relied upon to determine whether a patient requires analgesia. This is consistent with findings of previous research on this topic 24 and suggests that some patients will be unable to provide a meaningful pain or comfort score.
There were several limitations to this study. A wide age range of participants and the variation in numbers of postoperative days may have contributed to differences in the scores of pain and comfort. However, by including all patients scheduled to be seen on the pain round as per our hospital routine, external validity was maximised, making it likely that our findings are applicable in other postoperative pain round settings. Other variables, such as the timepoints for pain and comfort assessments on the same patient were within minutes of each other, likely limiting individual variability in patient responses. Second, the variability in the conduct of participant interviews may have potentially impacted our study findings. However, given the standardised, structured nature of the words used in each questionnaire and the use of a single researcher, the likelihood of variability was limited. In clinical practice, it is common that open and closed questions are used in patient assessments. In this study, we restricted the assessment to the use of closed questions, which may have influenced patient responses. It might have been helpful to include an initial open question such as ‘How are you feeling?’ However, some patients may be unable to describe what bothers them. It is frequently easier for many patients, especially in the context of pain and stress, to respond to closed questions where minimal cognitive effort is required. Another potential limitation is that recruited patients were exposed to questions by other doctors, nurses and allied health staff prior to our assessment of pain and comfort. This may have influenced patient perceptions and responses prior to their participation. Such differences in staff interactions are inevitable in any hospital environment. As our assessments were conducted in a clinical setting, our findings would be expected to have good external validity. Correlation may also have been influenced by patients’ uncertainty or unfamiliarity with comfort scores. Patients appeared on occasion to have varying interpretations of ‘pain’ and ‘comfort’. Some patients reported their responses were based on their physical postoperative sensations only, whilst others reported they also considered external influences in their responses such as mood, position and sleep disturbance. These factors may be more likely to be described as ‘bothersome’ when asking patients about comfort rather than pain. The diversity of deeply held sociocultural and psychological ideas about pain and its alleviation may also have contributed to our pain assessments in different ways.5,25 Subconscious influence on patient responses by knowledge of the study prior to questioning was avoided by obtaining informed consent after the survey was completed. Traditionally, researchers are required to obtain written informed consent from study participants prior to collecting any data. In studies investigating communication and its potential for subconscious responses, obtaining consent after conducting the study has been accepted as a necessary aspect of research methodology in this context in order to avoid influencing outcomes of interest. 17 Because of this potential contamination and the benign nature of the intervention, patient consent has sometimes been waived altogether. 8
Our findings imply that healthcare providers can usefully assess patients’ postoperative experiences and need for analgesia in ways that do not necessarily involve the use of pain scores. 26 Simply asking patients whether they need postoperative analgesia whilst avoiding nocebo may be more helpful. 24 For example, by asking a patient whether anything is needed to help them feel more comfortable may better reflect a patient’s need for pain-relieving medication than some arbitrary number that varies widely between individuals and can be misleading with regards to meaning. 24
In conclusion, our study findings demonstrate a moderate correlation between pain scores and comfort scores. This is a first step towards validating comfort scores as a potentially useful measure when assessing patients postoperatively. However, as comfort is not an exact antonym to pain, caution is required if using these measures of assessment interchangeably.
Footnotes
Acknowledgements
We acknowledge the support and assistance of patient participants at Nepean Hospital in New South Wales, Australia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.