
Abstract
Anaesthetists are key members of teams caring for burn-injured children in almost every aspect of their management. Their role can involve initial resuscitation, intensive care, analgesia, and anaesthesia for multiple procedures both acutely and subsequently for scar management. As key members of burns management teams, effective communication with patients and their families as well as other members of the burn care team is vital. There is little guidance, however, addressing how the anaesthetist might communicate and optimise anaesthetic burns care of children pre-, intra-, and postoperatively. Advances in the understanding of the neurobiology of communication suggests that we need to consider positive (placebo) or negative (nocebo) subconscious processes. Learnable language structures GREAT (Greeting, Rapport, Expectations, Addressing concerns, Tacit agreement) and LAURS (Listening, Acceptance, Utilisation, Reframing, Suggestion) can facilitate any patient or family interaction ensuring children and their parents feel they are being heard and understood. Talking about finishing rather than starting when about to perform a potentially painful procedure can also facilitate burns care with children. Other strategies include the avoidance of nocebo communications or apologising before a painful procedure and, instead, focusing on therapeutic (placebo) alternatives. Children do not view pain in the same way as adults do, and techniques such as play therapy and hypnosis can be valuable adjuncts to traditional analgesia administration in burns care, with the added benefit of minimising side-effects. The use of regular time-outs during prolonged burns surgeries is a helpful communication strategy between the anaesthetist and other members of the burns team that can optimise patient safety. Communication is a core clinical skill in the practice of anaesthesia during paediatric burns care and is an area for future research.
Introduction
Anaesthetists are key members of teams caring for burn-injured children in almost every aspect of their management. 1 Their role can involve initial resuscitation, intensive care, 2 analgesia, 1 and anaesthesia for multiple procedures both acutely and subsequently for scar management.
Although major burns in children are uncommon, even minor burns are painful and can cause major disability and morbidity with requirements for multiple procedures both in theatre and on the ward. These children pose well-recognised physiological and psychological challenges. 1 Although management of the physiological adverse effects of burns on patients is reasonably well established,1,3 little attention has been paid to the pivotal role that communication can play in enhancing a sense of control, recovery, and the optimisation of patient comfort.
The benefits of optimising anaesthesia communication skills have been reviewed in general terms in the context of the pre-anaesthetic visit 4 and perioperatively. 5 Despite this, there is no research or guidance addressing how communication might be optimised in the perioperative management of children suffering burns or how communication could be improved intraoperatively and postoperatively in this population.
In this setting, anaesthetists have traditionally focused on pharmacological management, resuscitation (including fluids and blood product transfusion) and technological advances in airway management and vascular access. Although communication with patients frequently goes well, there is little guidance on the communication strategies that could be utilised in more challenging cases, or how these might be taught to less experienced practitioners and trainees. Communicating effectively with other members of the burns team, patients and their families plays a pivotal role in optimising care.
Neurobiology of communication
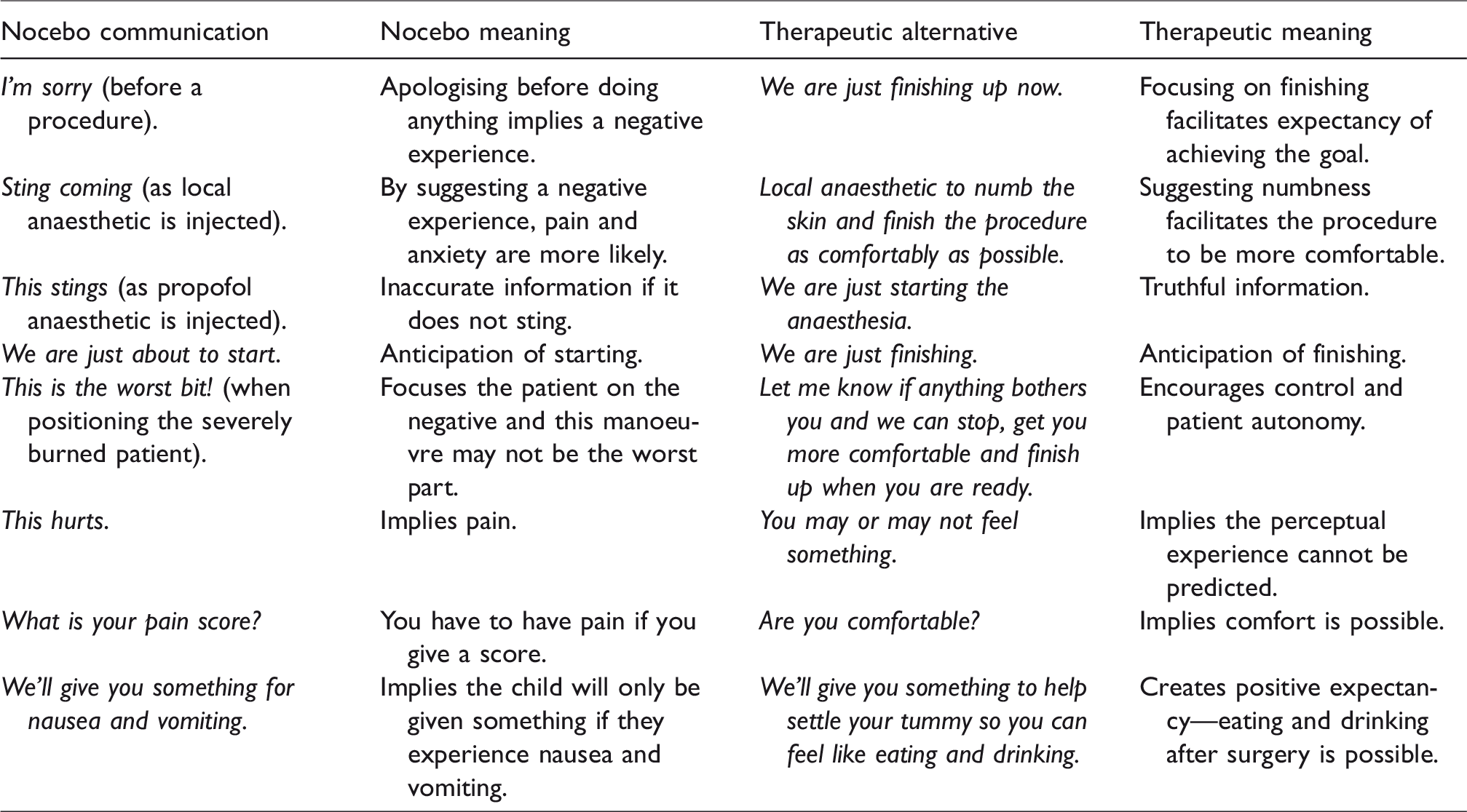
Advances in our understanding of the neurobiology of our communications and interactions suggest that we consider positive (placebo) or negative (nocebo) subconscious processes known as suggestion.6–9 Suggestions are verbal or non-verbal cues that can lead to changes in perception, mood or behaviour. There is a growing body of evidence that to warn patients using words that predict negative sensory experiences, may be unhelpful. 10 In contrast, an explanation around the meaning behind the need for a procedure rather than trying to predict a perceptual experience such as a ‘sting’, can be therapeutic (Table 1).
Inadvertent nocebo communications (negative suggestions) in the burns setting with children, and therapeutic alternatives.
Children with burns and the nocebo response
Children with burns are frequently overwhelmed by the sensory overload of their injury and the incomprehensible technology of the external environment—the wards, the intensive care unit, the operating room and anaesthesia machine. This results in little reality testing, with the patient being extremely vulnerable to the effects of the suggestions embedded in nocebo or placebo communications. For example, a young child informed by one of the theatre staff that the propofol would be like ‘little ants crawling up his arm’ was distressed for several hours postoperatively and complained of experiencing ants crawling up his arm. Children are responsive to authority figures and live in a world of play and make-believe, frequently responding subconsciously. Although staff need to be mindful of the possible nocebo effects of their interactions, therapeutic placebo communications can facilitate children experiencing potentially painful procedures more comfortably and with a sense of control. Indeed, they frequently respond in surprising ways that are therapeutic and can facilitate their recovery.
Language structures to consider
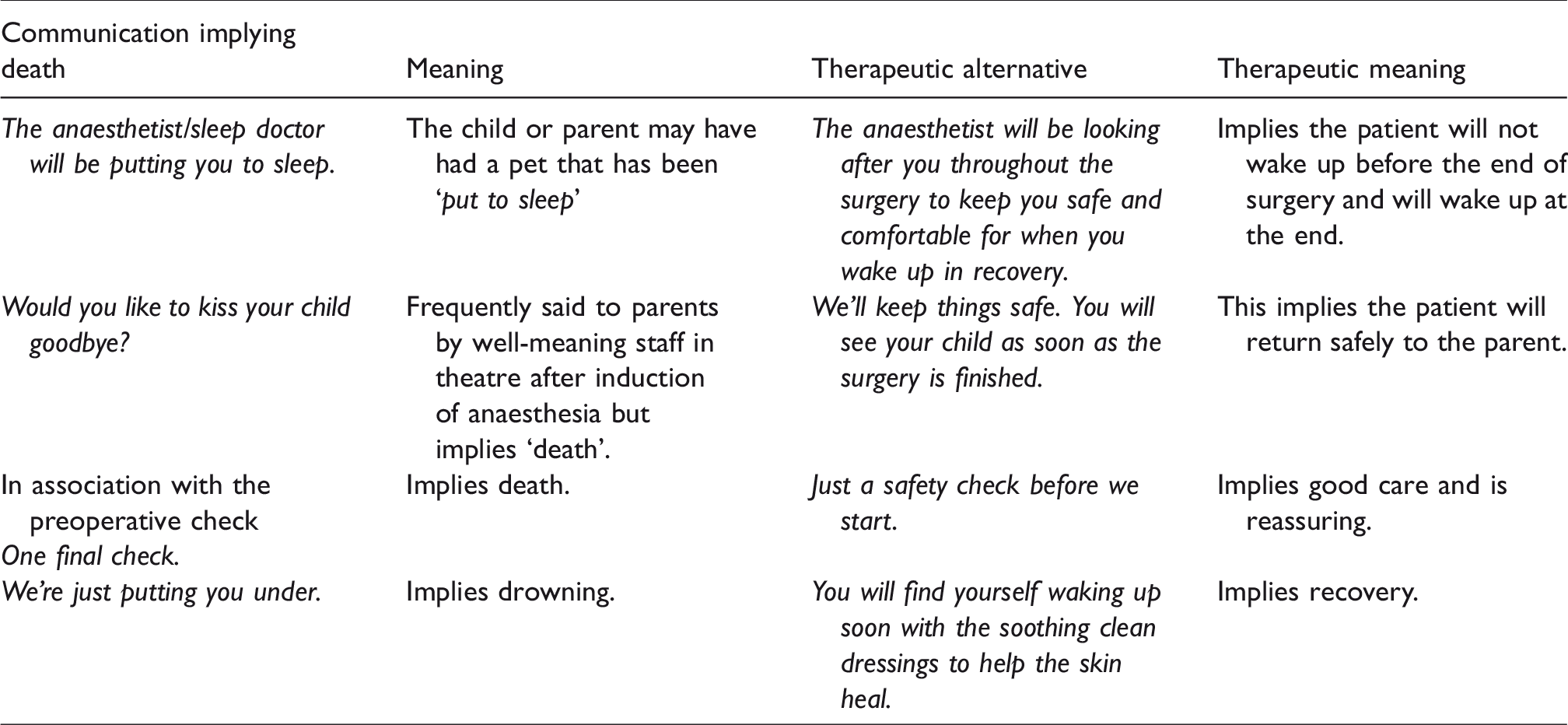
In the stressful environment of anaesthesia management of patients suffering burns, the GREAT and LAURS concepts 11 can be used as a learnable framework for effective communication in burns care. The GREAT template (Greeting, Rapport, Expectations, Addressing concerns, Tacit agreement) can be used to structure and teach burns care interactions. The LAURS structure (Listening, Acceptance, Utilisation, Reframing, and Suggestion) facilitates the development of rapport and primarily ensures that children and their families are heard, listened to for meaning, and feel understood.12,13 This involves a checking-in process- i.e. repeating back to the child or parent the words they have used so that the content or meaning can be verified and reframed, where necessary, in a therapeutic way (Tables 1 and 2).
Inadvertent communications with children and their parents implying death, their therapeutic alternatives and meanings.
The taxi driver metaphor
When we take a taxi and state where we wish to go, imagine what would happen if the driver was informed, ‘I don’t want to go to the beach’ or ‘I don’t want to go to the CBD’. Similarly, and unfortunately, in healthcare generally, patients are frequently informed where we would rather they did not go, rather than where we would like them to go (Table 1). Communicating about pain, nausea, itching, and so forth, before the patient experiences these symptoms may induce or exacerbate them. 14 In contrast, providing information pertaining to goal-directed outcomes such as comfort, healing, recovery, and things settling down can be therapeutic.
Apologising before a procedure
If the patient moves or voices pain, there is a temptation for the nurse or doctor to say, ‘Does that hurt?’ if it is assumed that pain was experienced. It is perfectly acceptable to say ‘Sorry’ if a child expresses distress after or during a procedure, for example, ‘I’m sorry that was uncomfortable for you. You did really well helping us to finish the procedure’. Apologising before a procedure is usually unhelpful as it implies there is something for which to apologise. This can lead to anticipatory anxiety. If the patient is asked instead, ‘What’s happening? Is something bothering you?’ the response may be, ‘Yes that hurts!’ or, ‘I thought I felt something’. Rather than asking about pain, the clinician might ask, ‘Is it bothering you? Are you comfortable?’ or, ‘Is it OK to carry on?’ when performing a potentially painful burns procedure. If the patient says something is sore, this perception needs to be validated and the anaesthetist can use the hurt or sore word and refocus the patient with, for example, ‘I know it hurts just now but we are giving some medicine so that it can feel more comfortable’.
Communication structures when the anaesthesia interaction is challenging
Engaging the parents may on occasion be best conducted when addressing the child. Similarly, communicating with the child may be conducted whilst addressing the parents if the child does not wish to engage directly with the anaesthetist. Appearing not to pay attention, saying something one does not believe is true, patronising or sympathising with phrases such as ‘There is nothing to worry about’, ‘Try to relax’ or, ‘I know how you feel’ are unlikely to be helpful.
In the acute setting, remembering to optimise our communication requires conscious effort. Even with repeated anaesthesia episodes where there are numerous technical tasks to complete during the induction of anaesthesia, it is important to remind oneself of the importance of focusing and engaging with the parents and child during this time. Patients whom we perceive as being demanding frequently respond positively when they feel they are being heard and understood. This involves ensuring words are heard correctly and the message being conveyed is reflected back to the child or parent so that they can confirm their intended meaning has been heard and understood.
Double binds
Giving children some control and choice over what is happening to them can be facilitated by the use of a double bind. Double binds are choices of comparable alternatives. For example, ‘Would you like to take three breaths or five before we finish placing the clean dressings?’ Alternatively, a helpful behaviour can be utilised and reinforced. Listening to and addressing children’s, parents’ and other relatives’ concerns frequently reveals opportunities to provide them with control without compromising anaesthetic care.
Sabotage and failure words
Try is a failure word. 5 If a child is asked to try, the expectation is that they will not be able to do it. Well-meaning parents may thus inadvertently sabotage therapeutic communications on the ward and in theatre. For example, by stating that ‘There is nothing to worry about’, the child may interpret this to mean ‘There is something to worry about’. Similarly, it may be stated, ‘This won’t hurt’ or that there is a ‘sting coming’. Such language can be mitigated, at least in theatre, by explaining to the parent that children find it easier to stay calm when they focus on one voice. The parent can then be asked, ‘Would it be OK if one person does the talking during the start of the anaesthetic? … Would it be OK if that person was me?’ (the anaesthetist). If the parent agrees, interruptions and inadvertent nocebo communications are likely to be avoided.
The importance of meaning
A child who had already had multiple procedures for debridement and grafting, developed infected and weeping skin over her facial burns. She required thrice daily cleaning of the infected wound on the ward and was extremely distressed, preventing the wounds being cleaned in a timely fashion despite opioid analgesia prior to and during the procedures that were taking up to two hours to complete. Prior to one of the scheduled procedures, the anaesthetist asked the girl what she planned to do when the skin had healed and she went home. The child replied that she would be able to play with her baby brother—her mother was pregnant at the time. The anaesthetist asked whether she knew why she was having her face cleaned and she replied that she did not. She was then asked whether she knew that by cleaning the infected skin it would heal faster and she would feel more comfortable (a positive suggestion for comfort), and would then be able to go home and see her baby brother. When she again replied that she had not known this, the anaesthetist asked whether it would be OK to clean the skin to help the skin recover and feel more comfortable so that she could go home sooner and see her baby brother. He also said that if at any stage she wanted the nurses to stop they would pause and only continue when she was ready for them to finish up. The patient agreed to this plan and despite three or four pauses she allowed the skin to be cleaned and the procedure only took 20 min. Further procedures took 10–15 min and within two weeks the infection had abated.
Starting versus finishing
Talking about finishing rather than starting when about to perform a potentially painful procedure appears to decrease anxiety and pain. This simple word change orientates the patient to the goal of having completed a successful procedure rather than approaching a less than certain outcome. We have found that warning children of impending dressing changes generates anxiety and anecdotally increases pain and distress. If the staff are fully prepared before engaging with the patient, they can then ask if it is ‘OK to finish putting the clean dressings on gently so that everything can heal and recover more comfortably?’
Perioperative care
Psychological approaches such as the use of hypnosis may have benefits alone or act as an adjunct to pharmacological analgesia. 15 Many patients with burns complain of itching during their recovery. This symptom can be extremely distressing but can be mitigated by simply explaining to the child that the medication to keep things comfortable (opioids) is working effectively. Alternatively, the pruritus can be given a therapeutic meaning by explaining to the child that this itch is because the skin is now beginning to recover and heal so everything can start feeling better.
Anaesthetists with some training in hypnosis may utilise more advanced techniques with some patients such as asking children what colour or sound or shape the itch is and how they might change it into a more comfortable colour or shape, for example, with their (imaginary) remote control.
A child having repeated debridement and grafting in the anaesthetic room was complaining of severe itching. A technique previously used with a five-year-old severely needle-phobic boy requiring intravenous immunoglobulin for Bruton’s disease was utilised. 16 The switch–wire imagery technique was discussed with the child prior to induction of anaesthesia for his debridement of burns and skin grafting. He was asked to close his eyes and take part in a favourite activity using the ‘Lived in Imagination’ technique where the boy chose an activity he found exciting—a technique that can be utilised to experience hypnotic responses more effectively. 12 He was then asked to let the anaesthetist know when, during the imagined activity, he had found the switch or dial controlling the itch. After 30 s he signalled with a nod of the head that he had found the switch and when asked to describe it he stated it to be a grey dial with numbers. The anaesthetist asked what number the dial was reading and he responded that it was set at ‘6’. The anaesthetist then asked the boy to turn the dial up to ‘7’ and see what happens—this was to see whether a perceptual change could be generated, as it is usually easier in the first instance to turn the pain or itch up rather than down. The child became distressed saying the itch was much worse. The anaesthetist then asked him to turn down the itching to ‘6’ again and on doing this he said it was better. Realising that he could change the itching with the metaphorical ‘dial in his brain’, he subsequently turned the dial to the ‘4’ setting at which level he could not feel the itch any more. He was then asked to keep the dial at this level unless he needed to turn it down further. He remained in hospital a further two months and never complained of pruritus again during his hospital stay.
Team communication: intraoperative ‘time-outs’
One of the main characteristics of anaesthesia and the management of major burns is the need for prolonged anaesthesia on multiple occasions during the initial series of debridement and grafting—sometimes as frequently as two or three times per week over several weeks or even months. Although sequestration has dramatically reduced the need for blood transfusion and frequent corrections of physiological instability, unrecognised blood loss and instability can still occur. To minimise the adverse effects of this risk, a series of time-outs can be conducted where the surgeon, anaesthetist and other team members can discuss progress, for example, the latest haemoglobin or arterial blood gas results, any changes in the surgical plan and address other concerns. The frequency can be initially at two-hourly intervals although this can be more frequent if need be.
Conclusion
Children do not view pain in the same way as adults, and techniques such as play therapy and hypnosis can be valuable adjuncts to traditional analgesia in burns care with the added benefit of minimising side-effects. 1 Effective communication with patients, their families and with other team members is a core clinical skill in the practice of anaesthesia 5 during burns care and is an area for future research. Children suffering from burns frequently respond in ways that surprise themselves, their parents and clinicians by doing more than they think they can, and more than we think they can.
Footnotes
Acknowledgements
Thanks to Evelyn Hood and Scott Simmons for proofreading the draft manuscript.
Declaration of conflicting interests
The author(s )declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.