
Abstract
Lack of continuing education and physician anaesthetist support are commonly cited problems amongst Ethiopian anaesthetic providers. Whilst operating at Jimma University Medical Centre (JUMC), Operation Smile volunteers identified a clear need for improvement in anaesthetic care delivery at JUMC. JUMC is a 450-bed university teaching hospital 350 km southwest of Addis Ababa. At the start of this programme it had two physician anaesthetists, with the majority of anaesthesia historically having been provided by non-physician anaesthesia providers. A visiting lecturer programme was established at JUMC in 2012 following collaboration between two consultant anaesthetists, working for Operation Smile and JUMC respectively. UK trainee anaesthetists in their final years of anaesthetic training volunteered at JUMC for periods of two to six months, providing sustainable education and consistent physician anaesthetist presence to support service provision and training. Over its six-year history, nine visiting lecturers have volunteered at JUMC. They have helped establish a postgraduate training programme in anaesthesia, assisting in the provision of a future physician anaesthetist workforce. Four different training courses designed for low- and middle-income countries (LMICs) have been delivered and visiting lecturers have trained local anaesthetists in subsequent course delivery. Patient safety and quality improvement projects have included introducing the World Health Organization Surgical Safety Checklist, Lifebox pulse oximeters, obstetric spinal anaesthesia packs, improving critical care delivery and establishing two post-anaesthetic care units. Development of partnerships on local, national and global platforms were key to the effective delivery of relevant sustainable education and support. Instilling local ownership proved fundamental to implementing change in the local safety culture at JUMC. Sound mentorship from anaesthetic consultant supervisors both in the UK and in Jimma was crucial to support the UK trainee anaesthetists working in a challenging global setting. This model of sustainable capacity building in an LMIC with a significant deficit in its physician workforce could be replicated in a similar LMIC setting.
Background
Ethiopia has a population of 99 million (median age 18.2 years). Access to healthcare is poor with a physician density of 0.25 per 10,000 of the population (Europe 30 per 10,000). 1 Jimma University Medical Centre (JUMC) is a 450-bed teaching hospital 350 km southwest of Addis Ababa. As the only referral hospital for south-western Ethiopia it provides services for 175,000 patients annually with a catchment population of 15 million. It currently has a six-bed intensive care unit (ICU) with capacity for three ventilated patients.
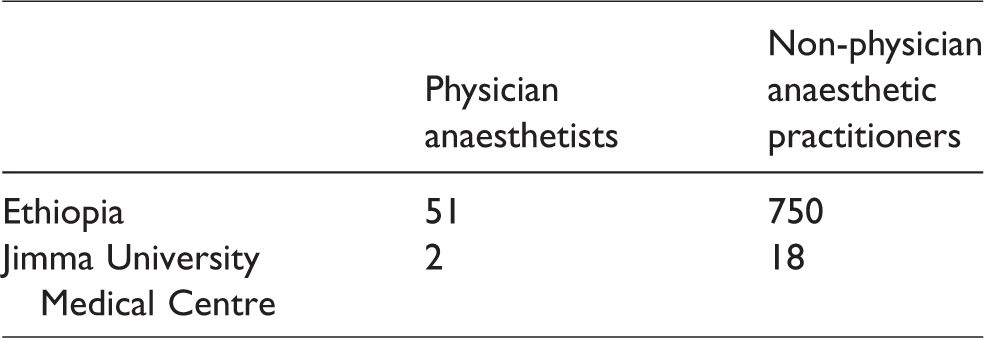
Anaesthetic task shifting or sharing is employed by over 100 countries worldwide to help meet surgical demand and involves non-physician anaesthesia providers (NPAPs) sharing provision of anaesthesia with specialist anaesthetists. 2 Anaesthesia in Ethiopia is provided by 51 physician anaesthetists and 750 NPAPs. 3 At the outset of this programme in 2012, there were two physician anaesthetists working at JUMC, the majority of anaesthesia being provided by NPAPs (Table 1).
Numbers of physician anaesthetists and non-physician anaesthetic practitioners across Ethiopia as a whole and at Jimma University Medical Centre.
As in many other low- and middle-income countries (LMICs), 4 training of NPAPs in Ethiopia is not regulated or standardised and varies from three months’ practical anaesthetic training ‘on the job’ to a formal three-year Bachelor of Science (BSc) degree in anaesthesia. NPAPs working at JUMC all complete such a three-year BSc at Jimma University, a programme that has been running in Jimma since 2005, and some have then undertaken a further one-year Master of Science course in anaesthesia in Addis Ababa. In 2012, development of a structured three-year postgraduate programme in anaesthesia for JUMC medical graduates was also being considered.
The problem
Surgery has been estimated to account for 28%–32% of the global burden of disease. 5 The Lancet Commission for Global Surgery reported inadequate development of essential, safe, life-saving surgical care in LMICs. 6 Safe surgery has increasingly been recognised as an important tool in improving LMIC health outcomes.
Historically, anaesthesia is one of the least developed disciplines in Ethiopian medical practice. This is reflected in other LMICs where anaesthesia often suffers from a low status compared to other medical specialties.7,8 In LMICs, particularly within anaesthesia, problems with workforce recruitment and retention are well described.9,10 In this setting it is challenging to develop and maintain a strong professional body in anaesthesia. There is little incentive to enter the profession, resources are limited and working conditions are often poor. 10 Whilst 27 physician anaesthetists have been trained in Addis Ababa, only 17 currently serve Ethiopia. Lack of access to continuing professional development and physician anaesthetist support are commonly cited issues amongst Ethiopian anaesthetists. 11
JUMC anaesthesia providers also reported their professional status was often undermined by surgeons and managers alike. As non-physicians, they felt a lack of respect for the gravity of their clinical acumen and decision-making, a dynamic frequently challenging patient safety. 10 Poor relationships with managers, 12 lack of professional satisfaction, lack of career progression, poor access to resources and high workload have all been cited as factors pushing healthcare workers out of LMICs. 13 Unfortunately these are all prevalent in anaesthesia in Ethiopia and have been linked with increased rates of burnout. 12
Operation Smile, a charity undertaking global cleft lip and palate surgery, 14 has been operating annually at JUMC since 2006. Volunteer anaesthetic consultants working with Operation Smile in Jimma identified a clear need for anaesthetic training and education to facilitate safer access to surgery. Operation Smile’s UK Medical Director recognised that positive anaesthetic role models could challenge surgical and managerial attitudes and reinforce the importance of the anaesthetist in delivering safe surgical care. There was a demand for a sustainable education programme with consistent physician anaesthetist support for local NPAPs.
Methods
A collaborative vision formed by Operation Smile and the Head of JUMC Anaesthesiology proposed that senior UK anaesthetic trainees in their final years of training volunteer at Jimma University for pre-defined time periods as visiting lecturers (VLs). The focus of the educational programme was on the needs of the hospital and the community it serves, providing training and capacity building for the future.
VLs were all in the final three years of their seven-year training programme and had passed the Final Fellowship Examination of the Royal College of Anaesthetists. Time working in LMICs is supported and encouraged by the Royal College of Anaesthetists’ curriculum which includes an optional Higher Level Unit of Training in ‘Anaesthesia in developing countries’, 15 an option which may be more difficult or not available to trainees within shorter programmes in other parts of the world.
Pilot period and needs assessment
In order to gather information regarding the proposal’s value, in August 2012 the first VL ran a two-month pilot project. The VL was supported from the UK by Operation Smile’s Medical Director and locally by the Head of Anaesthesiology. A needs assessment was conducted in conjunction with Jimma University by observing routine practice in the operating theatres, ICU, obstetric unit and postoperative wards, which highlighted the key needs to be addressed by future VLs.
The initial goals were to improve morale and retention of anaesthetic providers, establish a postgraduate physician training programme in anaesthesia, introduce post-anaesthetic care units and incorporate the use of the World Health Organization (WHO) Surgical Safety Checklist 16 as standard practice. Specific areas identified for improvement were reducing the ICU mortality rate, increasing the use of regional anaesthesia in obstetric practice and improving pain management in surgical patients.
During the pilot, the VL began training medical students in life support, taught aspects of the NPAP three-year BSc course, conducted theatre-based emergency simulation using a donated manikin and introduced the WHO Surgical Safety Checklist. New pain management guidelines for postoperative ward staff were introduced and a framework for a postgraduate syllabus to train future JUMC doctors in anaesthesia was established. A detailed analysis of the ICU identified key areas for improvement. 17
Development of the VL programme
Following the pilot period, the feasibility of the VL programme was clear. Several standards of care had already been investigated and small changes implemented with demonstrable improvements. Funding was secured to support further UK anaesthetic trainees wishing to volunteer to work at JUMC for two- to six-month periods. The VL programme was made available to senior UK trainees who had completed four years of specialist anaesthetic training and had a specific interest in anaesthesia in LMICs. They were initially selected from within Kent Surrey and Sussex Deanery in the UK. More latterly ‘Lifebox Fellows’ have been recruited nationally via a competitive application and interview process.
Whilst time, finances, poorly outlined objectives and lack of preparation can all present potential barriers to volunteering, these issues can be overcome by collaborating with key programme partners. Securing funding to assist with the VL programme costs helped to ensure that financial disincentives were less problematic. Whilst VLs did not receive their full UK salary, they received a bursary of £1000 per month whilst volunteering in Jimma to help cover their costs.
Jimma University provided the clinical demand, local mentorship and objectives for VLs whilst allowing individual creativity and innovation. A consultant anaesthetist in the UK provided remote support and was easily contactable by telephone, Skype or email. The Head of the Department of Anaesthesiology at JUMC (a physician anaesthetist) provided educational supervision in Jimma. He undertook the Royal College of Anaesthetists’ educational supervisor training, enabling UK trainees to sign off workplace-based assessments whilst in Jimma and to count their Ethiopian experience towards their UK anaesthetic training if they so wished as ‘Out of Programme Training’. VLs were all encouraged to complete the Higher Unit of Training in ‘Anaesthesia in developing countries’ according to the Royal College of Anaesthetists’ curriculum. 15
In March 2014, a further needs assessment was conducted by a series of interviews with key staff at JUMC and Jimma University. It was evident that the programme had made a significant impact on doctors’ and nurses’ training and there was a keen desire from JUMC and the university for its continuation. Key future initiatives for VLs included training Ethiopian faculty to deliver teaching courses and assisting with the further development of the postgraduate programme in anaesthesia.
Results achieved
From August 2012 to 2018, nine VLs have volunteered at JUMC. Gaps with no VL presence in Jimma have reflected periods of political instability and recruitment difficulty. Table 2 summarises the principal changes that have been implemented. These have incorporated the introduction of training courses, patient safety initiatives and quality improvement projects.
Summary of the principal changes implemented by UK Visiting Lecturers over the six-year programme at Jimma University Specialised Hospital.
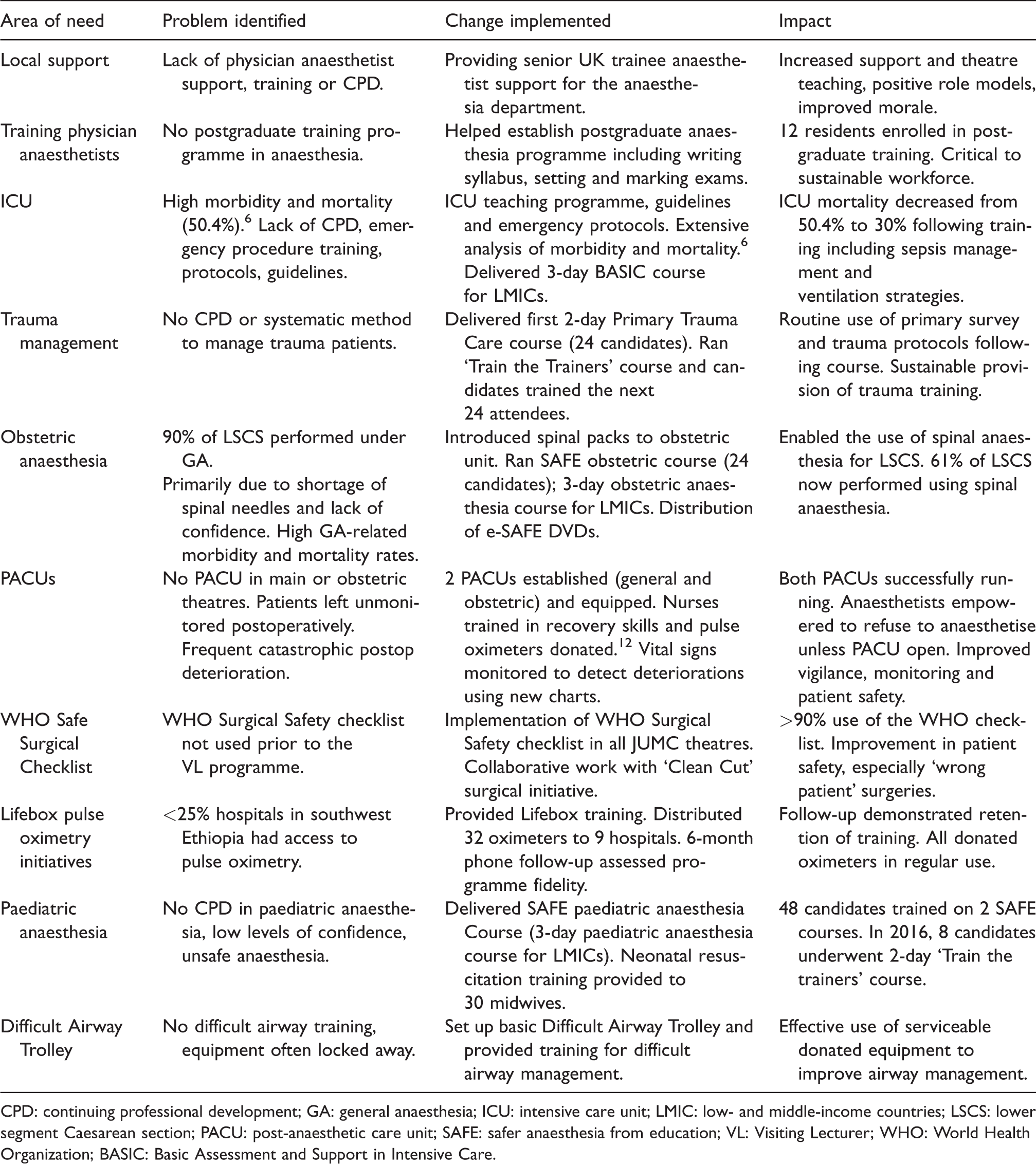
CPD: continuing professional development; GA: general anaesthesia; ICU: intensive care unit; LMIC: low- and middle-income countries; LSCS: lower segment Caesarean section; PACU: post-anaesthetic care unit; SAFE: safer anaesthesia from education; VL: Visiting Lecturer; WHO: World Health Organization; BASIC: Basic Assessment and Support in Intensive Care.
Establishment of a postgraduate physician training programme in anaesthesia
Since 2005, Jimma University has offered a generic three-year undergraduate BSc programme in anaesthesia. With increasingly specialised surgery being performed in line with JUMC’s expansion, a need for greater physician anaesthetist presence was identified. During the pilot period, the first VL assisted the Head of Anaesthesiology at JUMC in addressing the requirement for a postgraduate training programme in anaesthesia. Subsequent VLs further developed the syllabus in conjunction with Jimma University (Table 3). The first year of the programme focuses on basic sciences and the basis of anaesthetic practice. Subsequent years are more heavily weighted towards clinical anaesthesia. In their final year, residents are exposed to a range of subspecialties and must complete a research project in anaesthesia or critical care. Training is based on increasing levels of clinical responsibility, with careful supervision to support residents and maintain patient safety.
Key features of the postgraduate programme in anaesthesiology at Jimma University.
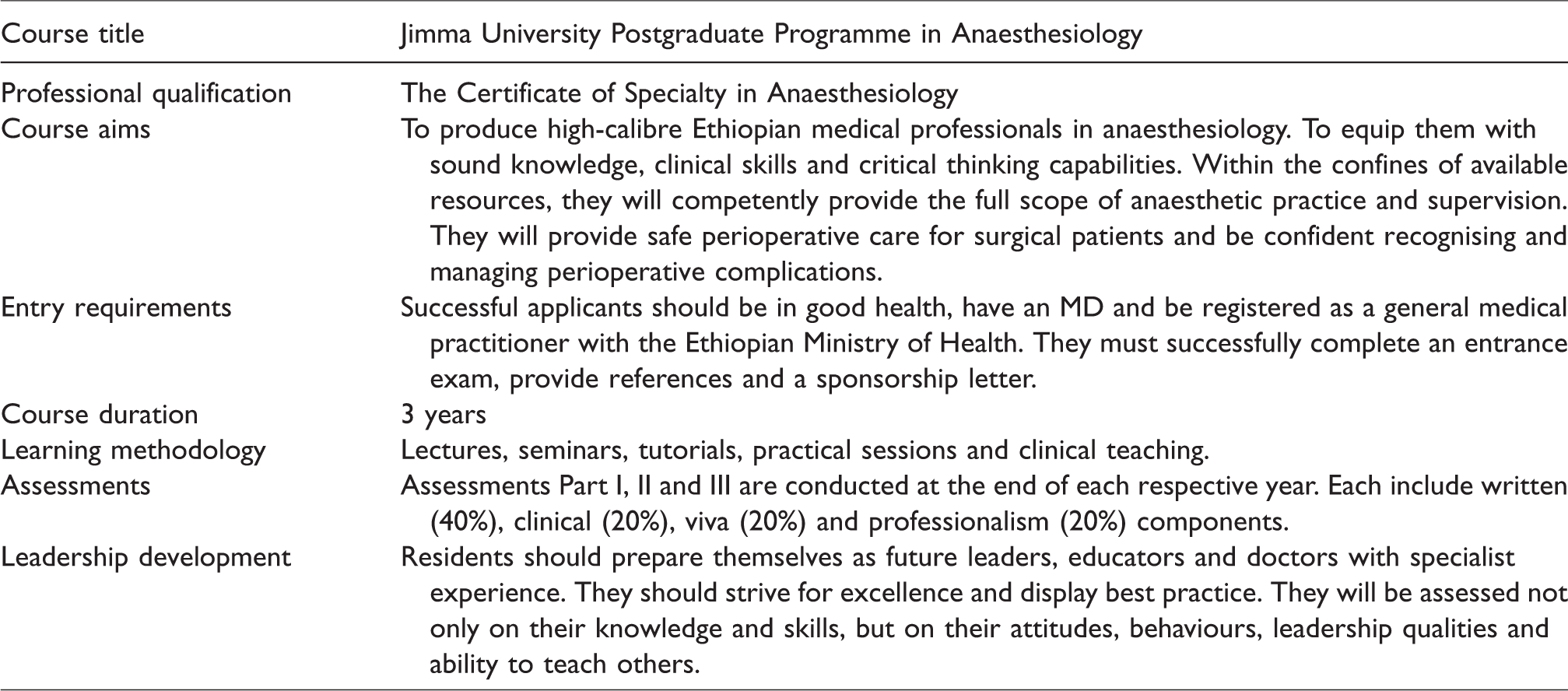
There are now 12 Ethiopian physicians enrolled in the three-year postgraduate physician anaesthesia programme, with three having recently completed their postgraduate training. With the addition of JUMC, there are now three Ethiopian schools providing postgraduate training to doctors wishing to gain the ‘Certificate of Specialty in Anaesthesiology’. A standardised nationally approved curriculum is currently under revision.
Training courses for LMIC settings
High-quality educational programmes can help to improve skills and knowledge, increase provider numbers and train future teachers and leaders. 18 Several purpose-designed courses cater for the specific demands of training LMIC healthcare providers, and external support from higher income countries helps to develop self-sustaining programmes. 19 Launched in 2010, Safer Anaesthesia from Education (SAFE) courses are an Association of Anaesthetists of Great Britain and Ireland (AAGBI) initiative. 20 The SAFE approach combines UK physician anaesthetists with local instructors who undertake a ‘Training of Trainers’ course to become future in-country faculty. The local instructors may be physician anaesthetists or NPAPs. The Primary Trauma Care (PTC) Foundation has adopted the same model for providing LMIC trauma courses. 21 PTC courses, SAFE Obstetric and Paediatric courses and Basic Assessment and Support in Intensive Care (BASIC) courses were all successfully introduced at JUMC with excellent feedback (Table 2). Some were locally adapted over subsequent courses to meet specific local requirements based on this feedback. Numerous Ethiopian anaesthetists have been formally trained as future faculty, facilitating the sustainable provision of high quality, locally delivered training. 18
The WHO Surgical Safety Checklist
As many adverse events in operating rooms are preventable 22 and the WHO Surgical Safety Checklist was one prevention initiative, 23 the checklist was locally adapted and first introduced to JUMC in 2012 using material from the ‘WHO Safe Surgery Saves Lives’ campaign. Videos were translated into Amharic, the principal language in Jimma, and the lead scrub nurses for each theatre were the focus of initial training by VLs. The nursing staff were given ownership of the checklist and they helped adapt it specifically for JUMC theatres. Having invested in its development, they were keen to see its use and felt empowered to encourage NPAP involvement. They were also inspired by an Amharic video showing a successful example of the checklist in use in another hospital in Addis Ababa.
Difficulties arose as a result of challenging entrenched hierarchical boundaries, particularly amongst surgical colleagues. Over the course of the VL programme, checklist use waxed and waned but an audit conducted in late 2017 showed it was used in over 90% of cases. More latterly, VLs were supported by a Lifebox Fellow launching a pilot of the Lifebox ‘Clean Cut’ campaign to help reduce rates of surgical site infection. This re-emphasised its importance and helped to maintain higher rates of WHO checklist compliance.
Lifebox pulse oximetry
It is internationally acknowledged that pulse oximetry is mandatory for safe anaesthesia provision.16,24 Despite this being a minimum requirement in 58 countries, a significant discrepancy between availability of oximeters exists; 25 in southwest Ethiopia less than 25% of hospitals had an oximeter. The Lifebox Foundation has been committed to delivering oximeters and training to LMICs since 2011. During an Operation Smile mission in March 2012, the Lifebox oximetry training programme was delivered to 13 NPAPs from nine hospitals in south-western Ethiopia and 15 oximeters were subsequently donated. Only two hospitals had a functional pulse oximeter in the operating room prior to the Lifebox donation.
After a period of six months, each NPAP who had received the initial Lifebox training was followed up by telephone and underwent a semi-structured interview in order to establish the efficacy of the training and sustainability of the equipment donation. Nine NPAPs (69.2%) from eight of the nine original hospitals were successfully contacted by telephone. They were all able to accurately answer knowledge questions designed to assess their understanding of the initial training. This demonstrated that the education and training delivered by the Operation Smile-Lifebox partnership was effective. In 100% cases, the pulse oximeters that had been donated were functioning and in regular use. Further, in their case logbooks, NPAPs cited specific examples of improvements to patient safety. A need for an additional 12 pulse oximeters in operating rooms and recovery areas in south-western Ethiopia was identified. As a result, a further training programme was run the following year where 17 more oximeters were donated (Table 2).
Introduction of post-anaesthetic care units
All patients who have undergone anaesthesia are at risk of postoperative complications. International standards for safe anaesthetic practice state patients should be recovered and monitored in specifically designated locations. 24 Prior to the VL programme, there was no such provision; JUMC patients suffered serious morbidity and mortality, left in corridors until anaesthetic effects had diminished. VLs successfully trained staff and equipped two designated post-anaesthetic care units (PACUs) in general and obstetric operating theatres. 26
In the obstetric unit, this was initiated by gaining permission from the university dean, the medical director and the senior obstetricians. The concept and process was then introduced to both obstetricians and midwives at two of their morning meetings. The lead midwife was thoroughly engaged in the process from the outset. He had previously specifically expressed an interest in neonatal resuscitation training for his staff. Thus, the VL then ran five neonatal resuscitation sessions for the whole department comprising 30 midwives. Whilst the first 30 minutes focused on neonatal resuscitation, the second 20 minutes talked through the PACU observation chart, the principles of effective handover, basic monitoring and how to escalate concerns.
In the maternity unit, the WHO checklist and PACU were introduced simultaneously; each PACU training session also involved the WHO checklist process. The WHO checklist was printed on the reverse of the new PACU observation charts. Observations included heart rate, respiratory rate, blood pressure, blood loss and urinary output. The hospital administration agreed to provide funding to staff the PACUs. Disused storerooms in the theatre complexes were identified and converted to basic PACUs. They were equipped with repaired disused beds and simple tables for the new observation charts. Curtains and a clock were sourced from the local market by the VL and Lifebox pulse oximeters were donated to allow heart rate and oxygen saturation monitoring.
The VL organised a pilot week during which they launched the project, following patients from theatre to PACU and to the ward, helping the midwives and theatre teams with the process. Following their training, the VL was impressed by how much interest and attention to detail the staff demonstrated. The PACUs are still in use over two years later. A large part of the success of the initiative was the ownership of the project by local staff. In particular, the lead midwife was a constant companion and an ambassador.
Spinal needle packs for maternity theatres
Wherever possible, the use of neuraxial analgesia and anaesthesia over general anaesthesia (GA) in obstetrics is widely accepted as optimal practice. 27 Despite this, maternity units in LMICs often struggle to implement such standards, with lack of equipment including spinal needles and poor training being common problems. Prior to the VL programme at JUMC, over 90% of lower segment caesarean section (LSCS) cases were conducted under GA.
One VL was able to provide training on the benefits of safe spinal anaesthesia to NPAPs and obstetricians using donated needle packs (Table 4) and as a result the hospital recognised the clear ongoing need, taking it upon themselves to provide an affordable and sustainable supply of appropriate equipment from within Ethiopia.
Contents of the donated single-use spinal needle packs that were used for training non-physician anaesthetic practitioners in the safe provision of spinal anaesthesia at Jimma University Medical Centre.
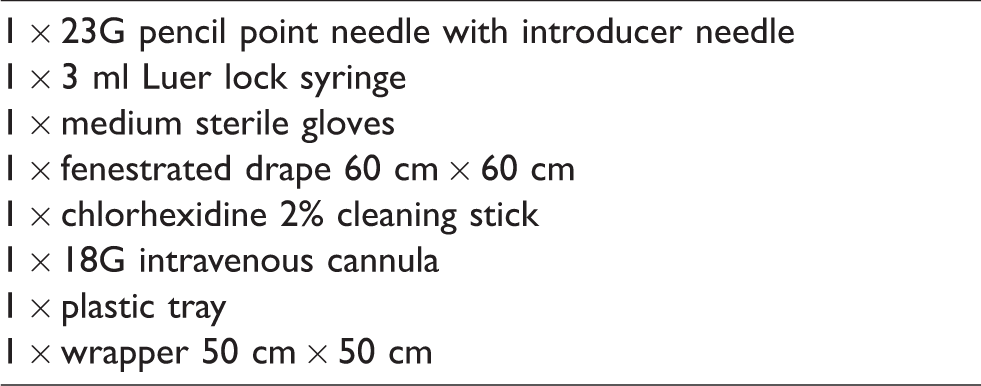
In 2016, data collected over a three-month period showed that single-use spinal needles were not only easily accessible but that the rate of LSCS performed under GA had fallen to 39% (150 out of 395 cases).
Improvements in critical care delivery
Baseline data collected at the start of the VL programme identified an all-cause mortality rate in JUMC ICU of 50.4%. 17 VLs introduced a weekly teaching programme for all ICU nursing staff run by the residents rotating through ICU. These sessions ran in eight-week blocks covering a variety of topics from fluid balance to nutrition and oxygen therapy. This also served to improve the dynamic between doctors and nursing staff.
Other initiatives focused on the introduction of protocols for the management of sepsis, head injury, ventilation and nasogastric feeding. Standardised proformas were developed for all ICU admissions, neurological observations and daily ward rounds to improve both quality of care and documentation. The daily ward round was further formalised, and the presence of a consultant, resident, intern and nursing staff was mandated to assist with communication and to maximise learning opportunities. Data collected from the admissions book over a one-month period following the implementation of these initiatives showed that the all-cause mortality rate had fallen to 30.0%.
Discussion
Over its six-year history, the VL programme has demonstrated significant sustainable impact. A key component to success has been partnerships built on local, national and global platforms. The development and maintenance of these partnerships has allowed collaborative working, appreciably enhancing the programme. They have been fundamental in the delivery of relevant, good quality, sustainable education and support. As an example, VLs worked alongside Swiss ‘Go Star’ trauma surgeons who also have a permanent presence in Jimma in the provision of trauma service support. In addition, two of the most recent VLs have been nationally recruited ‘Lifebox Fellows’ appointed by the Royal College of Anaesthetists. This has increased the project’s profile and credibility.
Challenges to a change in safety culture
Addressing the safety climate in Jimma’s operating theatres demanded significant and sustained commitment. The challenges to introducing change in a safety culture are significant and checklist implementation is not a quick fix.28,29
Over the course of the VL programme there has been regular monitoring of WHO checklist use and feedback with discussion. A key improvement has been the breakdown of previously well-defined hierarchical barriers between theatre health professionals. NPAPs and other theatre staff have been empowered to challenge surgical safety using the checklist as a tool. Unfortunately, frequent staff changes challenge the longevity of such an implementation and in periods where no VLs were present in Jimma, checklist use fell. Even after six years, a truly sustainable adoption of this simple, inexpensive and beneficial change has not been universally achieved.
The adoption and ‘buy in’ of the WHO checklist from surgical and anaesthetic staff proved more difficult than other more tangible initiatives involving physical entities such as the introduction of spinal packs and a PACU. These initiatives, whose impact on outcomes and patient safety were more immediately obvious, held greater appeal and were more likely to be adopted into daily practice. Much like the benefits of taking blood pressure medication, the benefits of the WHO checklist are perhaps more abstract, projected in time and difficult to immediately appreciate.
Issues surrounding medical equipment donation
The introduction and use of health technology in resource-poor settings presents numerous challenges including cost, sustainability, appropriateness and training. The telephone follow-up survey assessing the efficacy of the Lifebox oximeter donation programme showed that the devices were effective in the environment for which they were intended and were being used appropriately.
The procurement of spinal needle packs for training in the obstetric theatres is an example where specific needs-based donation can be successful.
Preparation and the importance of mentorship
Precipitating change in LMICs is demanding and fraught with cultural and political challenges. Whilst this was a unique opportunity for VLs to develop key transferable leadership, management, resilience, innovation and problem-solving skills, provision of adequate support and preparation was essential.
From the outset, the interview and selection process preferentially selected volunteer candidates with prior experience in global anaesthesia and working or living in LMICs. As such, although challenging at times, they were a self-selecting group of professional adult individuals with realistic expectations of situations with which they may have to cope. They all felt capable to adapt to the environment in which they had volunteered to work, and did so competently.
The Medical Director of Operation Smile personally briefed and met with all VLs before their departure for Ethiopia. Meetings involving all previous, current and future VLs doubled as debriefing and pre-departure briefings. Where possible, VLs overlapped by at least two days to permit an on-site handover in Jimma. This helped the new VL to settle in and facilitated sharing of relevant on-the-ground information. Where this was not possible, a pre-departure handover took place in the UK. VLs were also sent a comprehensive information pack designed by one of the VLs which included relevant local information and cultural differences. Each VL was required to produce a report upon their return and these were collated and made available for reference to all subsequent VLs using an online Dropbox folder.
Essential to this programme, Operation Smile, JUMC and Kent Surrey and Sussex Deanery provided VLs with valuable in-country and UK-based project mentorship, educational supervision and logistical support. Close working relationships between physician anaesthetist mentors in the UK and Ethiopia ensured that VL projects were in line with local requirements and their curriculum. Without these elements, the programme would not have been so successful.
Each VL was mentored by a consultant anaesthetist in the UK and the Head of Anaesthesiology at Jimma. Their UK supervisors required weekly reports so that progress could be evaluated and any problems and difficulties highlighted at an early stage. These reports served as a useful means for personal reflection, remote guidance and also as a resource to future VLs. In some respects, VLs felt they received better access to support and debriefing opportunities whilst in Ethiopia than in some situations working as trainees in the UK. Outside a prescriptive structure some VLs felt they had the autonomy to make the very best of their experiences.
Lessons learned
Development and maintenance of partnerships at all levels was key to the continued effective delivery of relevant, good quality, sustainable education and support. This included a longstanding partnership between Operation Smile and JUMC in which trust and confidence had been built up over a number of years between the UK and Ethiopian physician anaesthetists leading this project. Their good working relationship with Jimma University was also key to overseeing the work delivered by VLs and ensuring it remained relevant and of high quality. Instilling local ownership was fundamental to implementing change relating to the safety culture in operating theatres. Sound project mentorship, educational supervision and logistical support was crucial for the UK trainee anaesthetists driving clinical change and delivering education in a challenging low-resource setting.
Conclusion
Despite recent political disturbance, it is expected that the VL programme will continue to drive forward improvements in standards of surgical care at JUMC. Feedback from the two physician anaesthetists working at JUMC has highlighted improvements in both quality of training and safety of anaesthetic delivery following the introduction of the VL programme. The successful establishment of a postgraduate anaesthesia programme in providing a future physician anaesthetist workforce will be critical for the future provision of safe surgical care.
A simple direct consequence of senior UK trainees travelling to Ethiopia to support JUMC anaesthetic providers was to make them feel more valued and recognised on an international stage. This went some distance toward improving low morale in the specialty.
The profile for this project could be generalised to many healthcare settings in areas of educational need with an existing functional working relationship between local healthcare providers and a western counterpart. Voluntary schemes and partnerships have a key role in improving health worldwide and these can be mutually beneficial. 30 The further development of such international relationships would help progress towards 2030 targets in addressing the need for better global surgical services.
Footnotes
Acknowledgements
The feasibility pilot was jointly partially sponsored by Operation Smile, the Lifebox Foundation and the Emirates Foundation. The AAGBI and Royal College of Anaesthetists provided professional support. Laerdal Medical kindly donated a manikin for life-support training and B. Braun Medical Ltd donated spinal packs. The following additional VLs made the programme possible by volunteering their time in Jimma: J. Kilic, R. Stoddart, T. Bevir, A. Green, C. Dean, G. Harrington, N. Owen, B. Parsons.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kent, Surrey and Sussex Deanery and the Lifebox Foundation provided some funding for the VL programme.